Article Text

Abstract
Infection and sepsis are common problems in cancer management affecting up to 45% of patients and are associated with significant morbidity, mortality and healthcare utilisation.
Objective To develop and implement a whole of hospital clinical pathway for the management of sepsis (SP) in a specialised cancer hospital and to measure the impact on patient outcomes and healthcare utilisation.
Methods A multidisciplinary sepsis working party was established. Process mapping of practices for recognition and management of sepsis was undertaken across all clinical areas. A clinical pathway document that supported nurse-initiated sepsis care, prompt antibiotic and fluid resuscitation was implemented. Process and outcome measures for patients with sepsis were collected preimplementation (April–December 2012), postimplementation cohorts (April–December 2013), and from January to December 2014.
Results 323 patients were evaluated (111 preimplementation, 212 postimplementation). More patients with sepsis had lactate measured (75.0% vs 17.2%) and appropriate first dose antibiotic (90.1% vs 76.1%) (all p<0.05). Time to antibiotics was halved (55 vs 110 min, p<0.05). Patients with sepsis had lower rates of intensive care unit admission (17.1% vs 35.5%), postsepsis length of stay (7.5 vs 9.9 days), and sepsis-related mortality (5.0% vs 16.2%) (all p<0.05). Mean total hospital admission costs were lower in the SP cohort, with a significant difference in admission costs between historical and SP non-surgical groups of $A8363 (95% CI 81.02 to 16645.32, p=0.048) per patient on the pathway. A second cohort of 449 patients with sepsis from January to December 2014 demonstrated sustained improvement.
Conclusions The SP was associated with significant improvement in patient outcomes and reduced costs. The SP has been sustained since 2013, and has been successfully implemented in another hospital with further implementations underway in Victoria.
- nurses
- quality improvement
- process mapping
- health services research
- antibiotic management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Infection and sepsis are common problems in cancer management affecting up to 45% of patients and are associated with significant morbidity, mortality and healthcare utilisation.1–6 Patients with cancer are a unique population at increased risk of sepsis due to interventions such as chemotherapy, radiotherapy and complex or prolonged surgical procedures. However, most published international guidelines in this population focus on the management of neutropenic fever, and fail to address the full spectrum of patients across oncology, haematology, radiotherapy and cancer surgery, nor do they provide recommendations for the recognition and resuscitation of patients with sepsis.7–9 In a cancer hospital setting, sepsis is more common than neutropenic fever yet specialised guidelines are lacking.10
The major limitation of neutropenic fever guidelines is that the definition of neutropenic fever necessarily requires that the patient must have both fever and neutropaenia for initiation of antimicrobial therapy.7–9 In contrast, the diagnosis of sepsis using the systemic inflammatory response syndrome (SIRS) criteria or the more recent quick sepsis-related organ failure assessment (qSOFA) criteria,11 does not require the presence of fever. It is important to recognise that 30% of patients with severe sepsis do not have fever, and patients with neutropaenia may meet sepsis criteria without being febrile, leading to delays in administration of appropriate antimicrobial therapy.12
Standardisation of sepsis management using bundles of care has led to dramatic and sustained improvements in patients with severe sepsis or septic shock.13–17 We hypothesised that an optimal model for the management of infection in a cancer hospital would be to take a whole-of-systems approach to improving the recognition and resuscitation of sepsis in patients across their treatment journey, which might include surgery, chemotherapy and radiotherapy.
We undertook a quality improvement project in our cancer centre to identify existing processes and barriers to effective and efficient management of sepsis across the hospital, and to implement a hospital-wide clinical sepsis pathway (SP). The hospital-wide sepsis initiative, including the SP was implemented in March 2013. The aims of this study were to examine the impact of the SP intervention on process measures for sepsis recognition and management, and outcomes such as intensive care unit (ICU) admission rates, hospital length of stay (LOS), mortality and hospitalisation costs.
Methods
Context
Peter MacCallum Cancer Centre (PMCC) is a 100 inpatient-bed tertiary cancer hospital with haematology, medical oncology, cancer surgery and radiation oncology. As well as four wards, ambulatory areas include a chemotherapy day unit, a medical day unit, apheresis, hospital-in-the-home service, radiotherapy, diagnostic imaging and outpatient clinics. As there is no emergency department, patients were routinely admitted directly to the wards or through ambulatory areas. Cancer surgeries routinely performed include complex colorectal surgery (eg, pelvic exenteration), upper gastrointestinal surgery, breast and plastic surgery, head and neck surgery and sarcoma/skin cancer surgery. Neurosurgery, orthopaedic and thoracic surgery were generally performed at affiliated tertiary centres, although postoperative treatment including adjuvant radiotherapy and chemotherapy were administered at PMCC. Typically, patients present with sepsis at multiple sites throughout the hospital—medical day unit, ambulatory care/outpatients, chemotherapy day unit, apheresis, radiotherapy and inpatient wards. The hospital was moved to the Parkville precinct opposite Royal Melbourne Hospital in June 2016.
Definitions
The sepsis-2 (SIRS-based sepsis) criteria were used for this programme as it was developed prior to the publication of the sepsis-3 criteria.18 19 Clinical review criteria were represented as Between the Flags on the ward observation chart: SpO2 90%–95%, heart rate (HR) 120–130 beats , respiratory rate (RR) 25–30 breaths per minute, systolic blood pressure (SBP) 90–100 mm Hg, temperature >38°C or <35.4°C. Medical emergency team (MET) call criteria: SpO2 <90%, HR >130 beats per minute, RR >30 or <6 breaths per minute, SBP <90 mm Hg, altered conscious state, decreased urine output <0.5 mL/hour for >2 hours. Appropriateness of antimicrobial therapy was based on the National Antimicrobial Prescribing survey definition, and is a composite measure of choice based on indication, clinical guidelines, dose, route and allergy label.20
Overview of design
A mixed methodology exploratory sequential design was used to investigate barriers associated with efficient and effective inpatient management of sepsis.21 Hospital administrative data including International Classification of Diseases (ICD)-10 coding, the hospital antimicrobial approvals system and MET calls were used define the scope, burden and cost of sepsis. Concurrently, focus group interviews using lean methodology were completed to provide a comprehensive overview of sepsis management across all areas of the hospital. Results were used to inform the development and implementation of an evidence-based SP with evaluation of process and outcome measures. Finally, the resulting hospitalisation costs as associated hospital LOS were estimated. The project commenced in December 2011.
Focus group interviews
A sepsis working party was formed with medical, nursing and pharmacy representatives from the antimicrobial stewardship team, infectious diseases department, inpatient wards, specialty units and outpatient/ambulatory units. Members were clinical champions in their own area during the programme. Each member undertook direct observation and focus group interviews in an allocated clinical area. Three key areas were examined: (i) issues relating the identification of sepsis; (ii) issues relating to clinical review of patients with sepsis and (iii) issues relating to timely administration of first dose of antibiotic.
The focus group interviews were conducted by members of the sepsis working party using purposive sampling of junior and senior medical and nursing staff working across the hospital during January and February 2012. Process mapping was used to identify educational, clinical and infrastructural barriers to the efficient and effective inpatient and outpatient management of sepsis. This subsequently guided the development and implementation of the SP as described in the ’Results' section.
Impact analysis
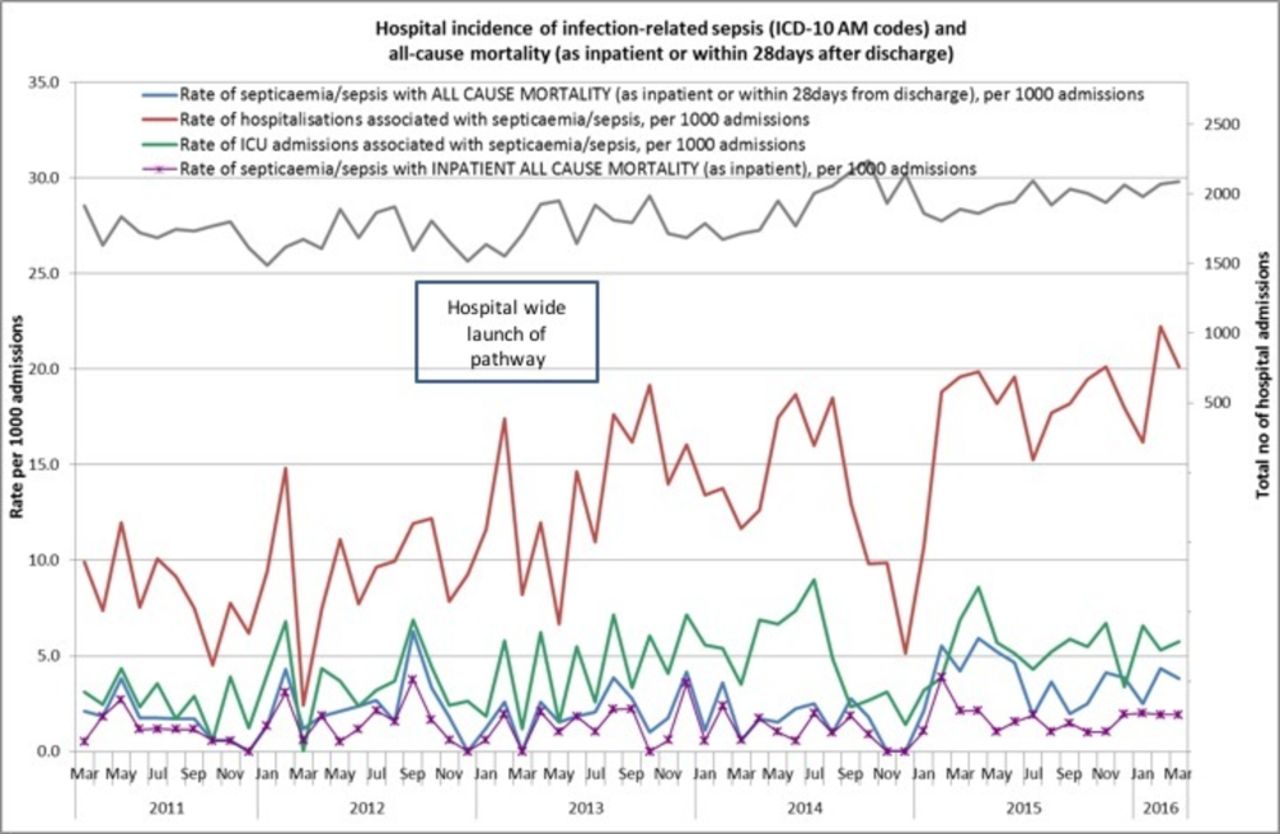
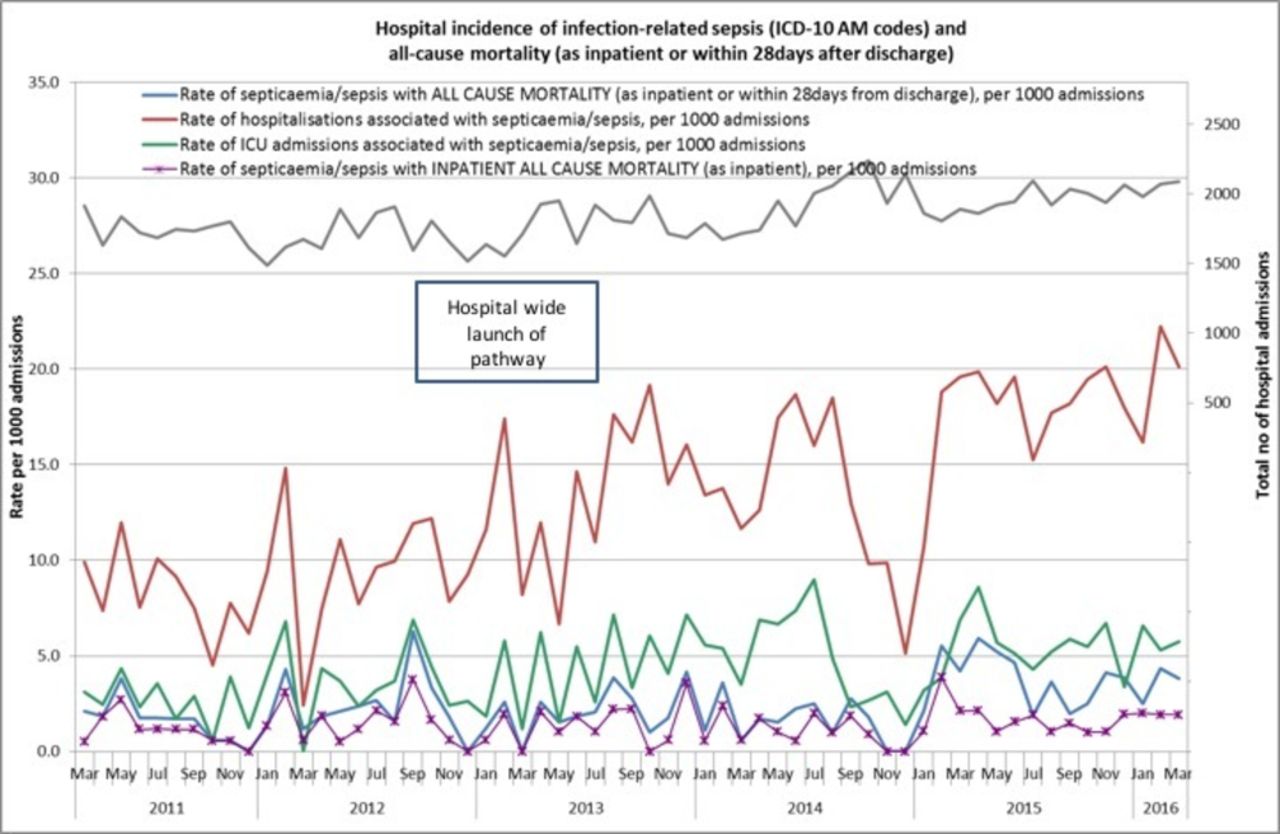
To estimate the burden of sepsis at PMCC, hospitalisations with an ICD-10AM (8th edition) coding for sepsis (online supplementary table 1)22 were matched with hospital administrative data including ICU admission and 28-day mortality. Coding data were extracted from March 2011 to March 2014 inclusive. Rates of sepsis, ICU admission and 28-day mortality were presented per 1000 admissions.
Supplemental material
The impact of the hospital-wide sepsis initiative was addressed through comparison of patient outcomes prepathway and postpathway implementation. For the prepathway (historical) cohort, patients were identified using hospital ICD-10AM coding and the antimicrobial approval system used for stewardship (Guidance, Melbourne Health, Australia). For the postpathway (SP) cohort, ICD-10AM coding and Guidance antimicrobial approval data were used in addition to the final audit page of each SP that was faxed to the Department of Infectious Diseases. Cases were also identified from the hospital-based electronic MET records system (RiskMan, Southbank, Victoria, Australia). Patients were excluded if they began treatment at another hospital or where sepsis onset was in the ICU. Demographic information (age, cancer diagnosis, admitting unit), sepsis recognition and management (vital signs, absolute neutrophil count, lactate level, fluid resuscitation and time-to-antibiotic) and outcome data (bacteraemia, ICU admission, hospital LOS, 30-day mortality) were collected from patient medical records.
The historical cohort presented from March to December 2012 and the SP cohort presented from March to December 2013, inclusive. A larger audit of all patients in the 2014 calendar year was retrospectively collected in 2015. Demographic information, sepsis recognition and management and outcome data in the historical and SP cohorts were compared and the SP cohort was further stratified by whether or not patients were entered onto the pathway. Administrative data and antimicrobial utilisation data were collected from 2011 to March 2016.
Statistical and cost analysis
A Χ2 test was used to compare categorical variables, and a Mann-Whitney U test was used to compare continuous non-parametric variables (Stata V.13.0, College Station, Texas, USA). All p values were two-tailed, and p<0.05 was considered to be statistically significant.
Hospitalisation costs of patients from the historical and implementation cohorts were extracted from the hospital’s administrative records, which reflected each patient’s hospital resource consumption. Costs included both direct and indirect costs and were categorised into relevant resource-use groups (such as allied health, ICU, nursing, imaging, medical, pharmacy, surgical and outside hospital care) for the entire length of their admission. A subset analysis according to cancer treatment modality was conducted where all medical patients (including haematology, medical oncology and radiation oncology (HMR)) were compared with surgical oncology patients.
Total hospital admission cost was the sum of all resource-use groups. The resource-use specifications are listed in online supplementary table 2. All mean costs of hospital resource use were reported with SD or 95% CIs. A t-test was used to test mean differences for those on the SP compared with the historical cohort and p values were reported. All costs were adjusted to 2017 Australian dollars using the Consumer Price Index.23
Results
Focus group interviews and gap analysis (February–March 2012)
Ambulatory areas in the hospital were evaluated separately to the inpatient areas as there were differences in staffing, workflow and access to equipment for the treatment of sepsis. The process maps for both ambulatory and inpatient areas are shown in online supplementary figures 1 and 2, respectively. These findings were distilled into three key focus areas that identified major gaps and hence key areas for improvement (table 1).
Barriers to appropriate sepsis management and corresponding interventions
Improve recognition and referral of sepsis across clinical areas.
Improve time to medical review.
Improved timeliness for the correct treatment of sepsis.
The actions taken to address each area are described in table 1. Importantly, a new six-bed area for acutely unwell patients requiring higher acuity care was opened in December 2012 and was used to minimise direct admissions to the ward, and for unplanned admissions from ambulatory care areas.
Sepsis pathway development (March–October 2012)
Based on results from the process mapping, several strategies to optimise sepsis recognition and management were identified and implemented. Central to the initiative was the development and implementation of a hospital-wide clinical pathway for the initial management of sepsis (first 24 hours). The pathway was adapted from the Clinical Excellence Commission Adult Sepsis Kills pathway for emergency departments and focused on timely and appropriate recognition, response and referral of patients with sepsis.24 Notable modifications to the pathway included (i) adaptation for inpatient use, (ii) relevance to cancer and immunocompromised patients particularly with regard to antimicrobial choice and (iii) that the pathway would be nurse-initiated.
Introducing the SIRS criteria into an early warning definition for sepsis was a major practice change as criteria differed from the existing clinical review criteria and MET criteria. When and if a patient met the proposed pathway definition of sepsis (two or more SIRS criteria, or hypotension with SBP <100 mm Hg plus an infection), nursing staff would notify the doctor using the Identify, Situation, Background, Assessment and Recommendation criteria,25 and commence the pathway including intravenous cannulation, two sets of blood cultures, venous blood lactate and routine bloods. This addressed the major structural barrier to prompt treatment as intravenous cannulation is necessary to administer fluids and antibiotics. The doctor was then required to review the patient within 30 min to chart the antibiotics and fluid orders. If a patient fulfilled MET criteria, then this would trigger a medical emergency team response, or if the patient had Goals of Care criteria limiting care then this would be heeded. The initial fluid resuscitation volume (10–20 mg/kg) of crystalline fluid was to be given as a rapid fluid bolus if the patient was hypotensive or had an elevated lactate (>4 mmol/L). The empiric antimicrobial recommendations were chosen to cover major pathogens in neutropenic fever or intra-abdominal sepsis postcolorectal surgery (which were the highest risk groups in the hospital). The initial antibiotic choice was piperacillin/tazobactam, cefepime for non-immediate hypersensitivity to beta-lactams, and ciprofloxacin plus vancomycin for immediate hypersensitivity to beta-lactams. Addition of gentamicin as a stat dose, and vancomycin were only recommended in the case of severe sepsis and in the case of vancomycin, additional indications for use such as suspected line infection, or known colonisation or infection with methicillin-resistant Gram-positive bacteria (online supplementary figure 3 for the SP document).
The SP protocol underwent extensive review and endorsement by key stakeholders within the hospital including senior representatives from the medical oncology, haematology, surgical and infectious diseases clinical units, senior nurses and nursing education, intensive care, palliative care, ICU liaison staff and clinical pharmacists. The pathway was developed as a medical record document, which would be filed with the patient’s record and would facilitate handover as well as high-quality clinical coding for sepsis. There were seven iterations of the pathway document prior to the first pilot.
Cycle 1 (pilot)
A small preimplementation pilot was performed in November and December 2012. The Medical Day Unit, haematology wards, the MET call team tested the form for usability and feasibility. The pathway was very well liked, and the only major change made to the document was the inclusion of the Goals of Care statement. This document was then printed as the medical record document and allocated a document identification number. During this period through to February 2013, education and training was commenced.
Cycle 2 (implementation)
The hospital-wide sepsis initiative, including the SP was implemented in March 2013. A comprehensive education campaign accompanied the SP implementation. A standardised presentation was developed and delivered to medical and nursing and pharmacy staff in all clinical areas by members of the sepsis-working group. Weekly email communiqués summarising key management principles and real-time audit results were also distributed to all clinical staff. A series of multichoice questions emailed to all staff was a popular initiative (online supplementary figure 2). Time to antibiotic initiation was the process measure that nursing staff preferred as best measure of performance in each clinical area. They became key drivers of the programme across the hospital.
Impact analysis
Overall, 323 patients were included in preimplementation and postimplementation evaluation. There were 111 patients in the historical cohort and 212 patients in the postimplementation cohort with 176 patients on the SP and 36 patients not on SP. Details of demographics, process measures and key outcomes are provided in table 2.
Patient demographics and clinical impact of implementation of whole of hospital sepsis pathway
Both cohorts were not significantly different except for the higher proportion of surgical oncology patients (22.7% vs 11.7%) and patients having surgery within 30 days (18.3% vs 6.3%) in the SP cohort (all p<0.05). The majority of surgical patients on the SP (85.0%) underwent colorectal (62.5%) and gastrointestinal surgery (22.5%).
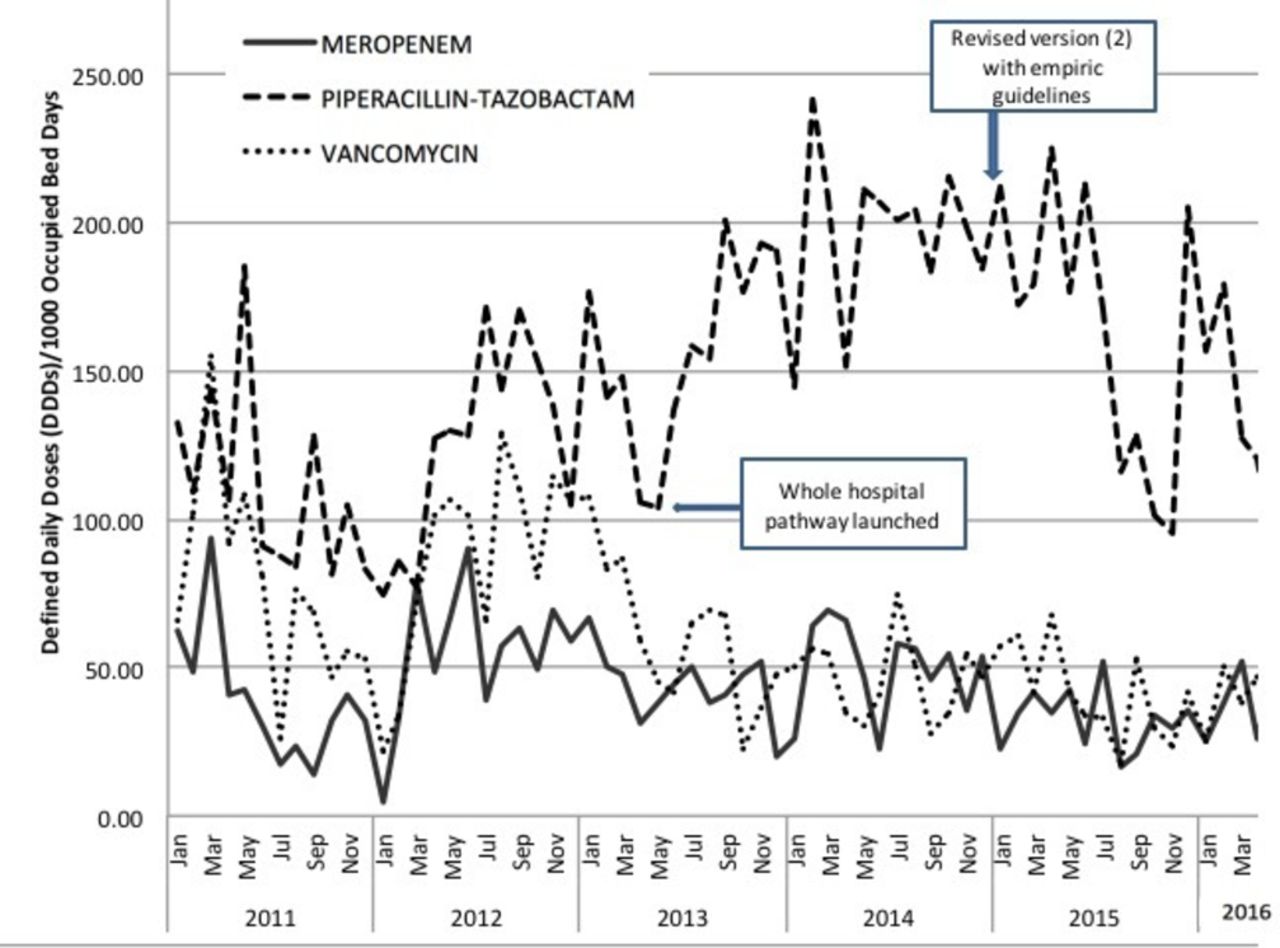
Following introduction of the SP, a significantly higher proportion of patients had lactate measured (75.0% vs 17.2%) and received the appropriate first antibiotic (90.1% vs 76.1%) (all p<0.05) while time to first dose of antibiotics was significantly shorter (55 vs 110 min, p<0.05) in patients on the SP compared with the historical patient cohort. The defined daily doses (DDD)/1000 occupied bed-days of vancomycin and meropenem also fell after the pathway was implemented (figure 1). Medical oncology patients on the SP received antibiotics most rapidly (45 min, IQR 30–100 min) followed by haematology patients (60 min, IQR 30–100 min), radiation oncology (60 min, IQR 38–272 min) and surgical patients (90 min, IQR 52–163 min), respectively.
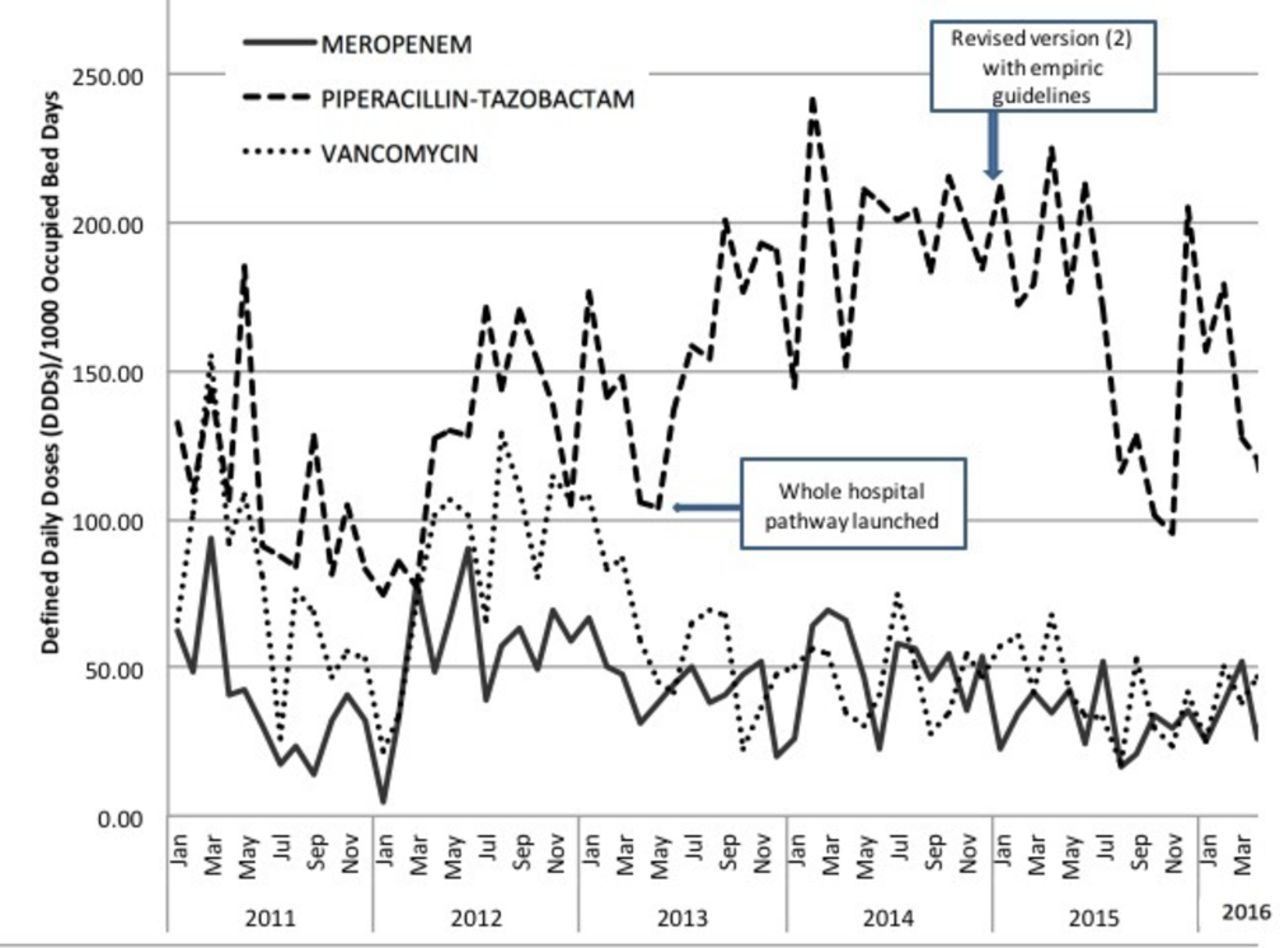
Impact of the sepsis pathway on utilisation of piperacillin/tazobactam, meropenem and vancomycin (as defined daily doses (DDDs)/1000 occupied bed-days.
Patients in the SP cohort on the pathway had significantly lower rates of ICU admission (17.1% vs 35.5%) and ICU LOS (7.5 vs 9.9 days) (all p<0.05). Sepsis-related mortality (5.0% vs 16.2%, p<0.05) and 30-day all-cause mortality (7.4% vs 18.9%, p<0.05) were also significantly lower following SP implementation.
The proportion of patients with normal SBP at sepsis recognition was lower in year 2 suggesting earlier recognition, although similar proportion required ICU admission (17.1% vs 18.3% in year 1 and year 2). There was poor compliance with the use of rapid bolus as well as recommended volumes. This may have been due to the fluid calculation required (by mL/kg) and general reluctance by medical staff to give larger boluses. The compliance with remainder of the pathway elements was maintained in the year 2 cohort from 2014 with improved antimicrobial appropriateness, but a reduction in the proportion of patients with two set of blood cultures. The pathway was associated with similarly improved patient outcomes. In year 2, there were a higher proportion of surgical patients and solid tumour patients in the non-pathway group.
The administrative coding data demonstrated that there was increased ascertainment of sepsis cases after the implementation but no concomitant increase in all-cause mortality or increased ICU admission (figure 2).
{kind=link}
{kind=link}
Burden of sepsis estimated from administrative data using ICD-10AM code preimplementation and postimplementation of sepsis pathway. ICD-10, International Classification of Diseases (ICD)-10; ICU, intensive care unit.
Cost analysis of implementation
Full costing data were available for 275 patients (91 historical and 184 SP cohorts). In the historical cohort, there were 80 HMR patients (87.9%) and 11 surgical patients (12.1%) while there were 147 HMR patients (79.8%) and 37 surgical patients (20.1%) in the SP cohort.
Table 3 shows the mean total hospitalisation cost per patient across the two cohorts and for each of the patient groups. Surgical patients incurred higher total admission costs compared with the HMR patient group. For both groups, the mean total admission cost was lower in the SP cohort. There was a significant difference in the admission cost per patient on the pathway between the historical and SP HMR groups of $A8363.17 (95% CI $A81.02 to $A16 645.32, p=0.048). Total admission cost was reflective of the hospital LOS.
Overall mean total hospitalisation cost (2017 Australian dollars) for historical and sepsis pathway cohorts by patient groups
For the majority of the resource-use groups (allied health, ICU, nursing, imaging, medical, pharmacy, surgical and outside hospital care), the cost incurred by historical cohort patients was higher than those in the SP cohort. The only resource-use group in which the SP cohort showed a higher cost than the historical cohort in both HMR and surgical groups was for pathology. There was a significant difference in ICU costs between the historical and SP cohorts of $A5470 (95% CI $A1780.21–9161.79, p<0.01) for HMR patients. For patients in the HMR group, the bulk of the total admission cost (between 36% and 41%) were for nursing services while in surgical patients, the majority of the cost was attributed to ICU cost (29% and 30%).
Cycle 3 (postimplementation and sustainability) 2014–2015
The Sepsis Working Party continued to monitor the programme with regular feedback from nurse unit managers in each area. While education relating to the pathway was integrated into medical staff orientation and nursing in-services, aspects of the pathway for which further education was required included: rapid volume fluid resuscitation and universal lactate testing (even if the SBP was normal). The pathway was modified at the end of a detailed audit of patients in 2014 with modification of fluids based on weight, lowering the lactate cut-off, clearer indications for antibiotics and inclusion of an empiric antibiotic table to assist definitive therapy, prompts for review of microbiology and clearer instructions for monitoring (see table 2 and supplement for version 2 SP document, MR63 SEPSIS Pathway_2015). This was associated with maintained low usage of meropenem and vancomycin, and a reduction in piperacillin/tazobactam (figure 1).
Sustainability and expansion of the SP pathway to other sites (2015-2018)
In June 2015, version 2 of the pathway was successfully implemented as part of the Western and Central Integrated Cancer Services programme into the oncology/haematology and bone marrow transplant unit at the Royal Melbourne Hospital (RMH). In 2016, the RMH (led by KT) was funded by Better Care Victoria (BCV) to implement the SP across the whole of the hospital and was formally launched in 2017 as the ‘Think Sepsis, Act Fast’ programme. The modification of the SP, implementation and results of this project will be published elsewhere, but this version is now adopted as the current version in PMCC (see online supplementary file) and retains the 30 min time to antibiotics recommendation for cancer patients. The key modifications of the pathway are included in table 4. In October 2017, BCV funded the scale up of the Think Sepsis, Act Fast programme to 23 hospitalsand 11 health services in Victoria.
Supplemental material
Version modifications of the sepsis pathway from 2013 to 2017 (see online supplementary file for pathway versions 2 and 3)
Supplemental material
Discussion
The introduction of a hospital-wide clinical pathway for the management of sepsis in a cancer hospital was associated with significant improvement in compliance with the core elements of the pathway and led to improved patient outcomes and reduced hospitalisation costs. This is the first study to examine the costs of sepsis in both neutropenic and non-neutropenic patients with cancer including surgical sepsis.26–29 The pathway was formally adopted into the partnering tertiary teaching hospital (Royal Melbourne Hospital) and has been endorsed by the Victorian state government for implementation into 26 further hospitals.
Process mapping the care of patients with sepsis, presenting key issues visually and as a gap analysis were essential to identify the core elements of the clinical pathway, to introduce structural changes around antimicrobials, venous blood lactate and fluid management and to identify the optimal mode of education by healthcare workers. Implementation studies of sepsis protocols have highlighted the importance of identifying structural barriers, knowledge gaps and competing priorities that exist in the hospital environment.30 31 A recognition that patients with cancer presented with sepsis in multiple and diverse environments in the hospital such as chemotherapy day unit, surgery32 outpatients, or even radiotherapy, staffed by clinical staff with different skill levels, highlighted the need for a standardised and broad reaching approach. Different observation charts were used across areas and triggers for clinical review and MET were not as sensitive as the SIRS criteria. Despite the potential for confusion, nursing staff embraced the new definition. Another important structural barrier identified was the lack of nursing staff able to cannulate, leading to delays in initiation of sepsis treatment while waiting for busy junior medical staff. Making available antibiotics for sepsis, and adequate numbers of rapid infusers for fluid administration on each ward was also necessary, as well as standardising the fluid on resuscitation trolleys.
In the cancer setting, nursing staff are accustomed to pathways and protocols for administration of analgesia and chemotherapy. In some clinical areas (eg, haematology), nursing expertise in managing very unwell patients led to a rapid adoption of the pathway. In other areas (eg, radiotherapy inpatients and surgery), more nurses needed more education and credentialing for procedures. A key facilitator for the success of this pathway was the change in practice to permit nurse-initiated care once a patient met sepsis criteria. Nurse-initiated care in sepsis has been successful in the emergency department and ICU setting.33 34 It also highlights the importance of clinical practices that facilitate staff empowerment and cultural changes, well-illustrated in mixed methods study of an implementation of a Rapid Response System in Northern Ireland.35 Senior medical staff support is another critical factor that has been shown to impact on efforts to change public hospital systems.36
While there is a perception that patients with cancer are somehow different, and that neutropenic fever is the most common manifestation of infection, the preimplementation and postimplementation data confirmed that only 40% of patients were neutropenic at the time of sepsis. Neutropenic fever largely influences empiric antibiotic choice. The Australian national consensus guidelines for the empiric management of neutropenic fever7 formed the basis of the initial antimicrobial recommendations. Piperacillin-tazobactam was also considered an appropriate option for the treatment of common infections (intra-abdominal sepsis, healthcare-associated pneumonia) acknowledging that the pathway managed the first 24 hours and that antibiotics would be reviewed following the sepsis workup. Appropriateness of antimicrobial prescribing increased from 75% to 90%, and was associated with a reduction in use of vancomycin and carbapenems, presumably as these were not recommended as part of the initial therapy. The overall usage of piperacillin-tazobactam (by DDDs) did increase, and this was addressed by including more directed options in the subsequent version of the SP.
Auditing of fluid administration from the paper medical records was difficult in the absence of an electronic medical record (EMR). The bolus fluid volumes, while increased, usually did not meet the 10–20/kg recommendation. There was an overall reluctance by medical staff to chart initial volumes >500 mL and subsequent iterations of the pathway have led to this volume as the preferred initial bolus (see version 3 (MR63_SP_2017), supplement).
With the publication of the updated sepsis criteria in 2016 and the adoption of the pathway by the RMH in 2017, the decision was made to retain the SIRS-based sepsis criteria as an early warning score but to include elements of severe sepsis (lactate, hypotension and altered mental state) (see version 3 MR63_SP_2017 , supplement). The results of the RMH implementation and the performance of pathway will be published separately. More recent publications including systematic reviews have demonstrated that the SIRS-based criteria correctly identifies one-third more patients with sepsis than does the qSOFA and may over diagnose sepsis,37 38 whereas qSOFA is slightly more specific and effective in predicting mortality from sepsis. In another study outside of ICU, patient with sepsis met ≥2 SIRS criteria 12 hours earlier than ≥2 qSOFA criteria.39 We believe that clinical pathways for high-risk patients should support the use of early warning criteria.
This hospital did not have an EMR where an alert trigger could be implemented using clinical observational criteria. The current evidence suggests that these alerts may be an effective intervention for sepsis.40–42 Nevertheless, this study demonstrates that the use of a paper-based clinical pathway using the SIRS-based sepsis definition can significantly improve the early appropriate treatment for sepsis. The clinical pathway was introduced as a formal medical record document that remained in the patient history and reinforced the programme’s importance to the clinicians and nurses. In future, the pathway could be adapted to an EMR order set format. The use of the document also enhanced the quality of the sepsis auditing process and medical coding (ICD-10AM), which we identified in the preimplementation period as being poorly done, and an observation that has been already reported.43 44
This is the first study to examine the costs of sepsis in both medical and surgical patients with cancer. The implementation of the SP protocol led to a significant reduction in patient hospitalisation costs and importantly, a significant improvement in 30-day all-cause mortality. While this study further adds to existing literature linking the effectiveness of protocols or sepsis bundles that better manage sepsis in reducing patient mortality,13–17 45 there is limited literature describing the economic impact of implementing a hospital-wide sepsis management pathway in patients with cancer. The implementation of SP in this study resulted in at least an average $A8363 reduction in hospitalisation cost per patient on the pathway compared with patients in the historical control group, which was largely driven by the shorter LOS. The lack of statistically significant difference in the surgical group was likely to be due to small patient numbers and large CIs. This reduction was translated across all resource-use groups except for pathology. Costing data were based on hospital cost rather than hospital charges, hence provide a true reflection of the healthcare resource used. These results highlight the SP protocol’s potential to improve the hospital’s efficiency in managing sepsis without compromising patients’ safety and outcomes and can similarly be used to assess and inform the allocation of resources to ensure sustainability.
While this study demonstrated that implementation of a hospital-wide SP in a cancer centre is feasible, may improve key patient outcomes and also potentially reduce hospitalisation costs, undertaking the evaluation study had some limitations. A retrospectively identified historical cohort preimplementation was used as the comparator to the postimplementation SP cohort. The quality of medical coding for sepsis significantly improved after the implementation of the pathway (from 63.7% to 81.9%), and was reflected in increased ascertainment of patients, and in particular the surgical cohort. We used additional data to accurately identify patients with sepsis. Use of administrative data for sepsis epidemiology and costing warrants further investigation.44 46 The compliance in process measures in patients who were not placed on the pathway was similar to those patients on the pathway, demonstrating that widespread practice change occurred after implementation. As this study was not a clinical trial, we cannot completely rule out other factors such as change in practice that might contribute to the difference in outcomes and costs that we observed. While the impact of the pathway was sustained, a more detailed understanding of why patients were not put on the pathway is necessary. Potential reasons include postsurgical patients who were not considered to be septic, end-stage cancer but without goals of care documentation or an oversight by busy clinical staff.
There is now compelling evidence that clinical pathways and bundles for the recognition and management of sepsis should be standard of care across hospitals. However, the implementation of a pathway requires a careful approach to understand the structural barriers and often unique issues experienced by clinical staff in both ambulatory and inpatient hospital areas. Antimicrobial stewardship programmes are ideally placed to lead a hospital-wide programme and to generate buy-in across clinical areas.47
Acknowledgments
The authors would like to thank the Sepsis Working Party, clinical nurse leaders (Delia Comodo, Kim Morris, Amy Haffenden, Jessica Willis) involved in the process mapping, development and implementation of the sepsis pathway and Ms Sok-Wee Yew for her assistance with data for costings.
References
Footnotes
Contributors KAT was the clinician lead for the SP since 2012, designed the data collection, contributed to the analysis and was the main author of this paper. SL was the AMS pharmacist and project officer during 2012/2013 and contributed to the study design data collection and authorship. JJ and GMH contributed to the data collection and implementation of the pathway, and review of the manuscript. BT contributed to SP sustainability and to authorship. MT undertook the cost analysis and contributed to authorship. KD supervised cost analysis. GV and AH collected 2014 data. VL contributed to database development and antimicrobial data. CB was the WCMICS project officer who assisted with the hospital implementation at both hospitals. LJW and MAS contributed to study design and authorship.
Funding This study was funded by Western and Central Melbourne Integrated Cancer Centre.
Competing interests None declared.
Patient consent Not required.
Ethics approval Peter MacCallum Cancer Centre Human Research Ethics Committee approved this study (Project No: 13/189 L).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Requests for access to data should be addressed to the corresponding author.