Article Text

Abstract
Introduction The most recent Global Initiative for Chronic Obstructive Lung Disease consensus recommends a 5-day course of corticosteroid (CS) therapy for acute chronic obstructive pulmonary disease exacerbations (ACOPDE). As inappropriate use of CS therapy is associated with adverse events, we implemented a peer-to-peer education intervention to improve adherence to guidelines for patients with ACOPDE admitted to a medical clinical teaching unit at a tertiary care university centre.
Methods Our study was a before–after design study with a concurrent control of a 15 min peer-to-peer educational intervention targeting medical residents at the beginning of a 4-week rotation for 12 consecutive months. Another medical teaching unit within the same university network, but at a different site, served as a concurrent control. The primary outcome was the proportion of patients who received appropriate duration of CS therapy (5 days) for ACOPDE during the intervention period as compared with the 12-month preintervention period at the intervention and control hospitals.
Results Following the intervention, there was an increase in the proportion of patients receiving appropriate duration of CS therapy (34.2% to 51.3%, p=0.02) at the intervention hospital and no significant difference at the control hospital (22.8% to 34.1%, p=0.15). This effect was maintained at the intervention hospital 3 months postintervention period.
Conclusion A short peer-to-peer educational intervention targeting medical residents on a clinical teaching unit improved adherence to appropriate duration of CS therapy for ACOPDE.
- clinical practice guidelines
- communication
- continuous quality improvement
- medical education
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- clinical practice guidelines
- communication
- continuous quality improvement
- medical education
- quality improvement
Introduction
Chronic obstructive pulmonary disease exacerbations (COPDE) contribute to long-term decline in lung function and cause serious morbidity and mortality.1 Systemic corticosteroids (CS) are the mainstay of therapy and are associated with shorter recovery, improved lung function and reduced hospital stay.2 The most recent Global Initiative for Chronic Obstructive Lung Disease consensus recommends a total duration of 5 days of CS for the treatment of COPDE.3 4 Since inappropriate duration of CS use is associated with adverse events,2 we aimed to optimise the duration of CS therapy (5 days) in adults hospitalised for COPDE on medical clinical teaching units (CTUs) of an academic medical centre with peer-to-peer teaching.
Methods
We used a before–after with concurrent control study design to determine the effect of a standardised 15 min educational presentation targeting internal medicine trainees on the optimal duration of CS therapy in patients admitted with COPDE. The presentation, by senior medical residents, occurred at the beginning of every 4-week internal medicine CTU rotation at one of two teaching hospitals of the McGill University Health Centre (Montreal, Canada) for 12 consecutive months (March 2014–February 2015). The other hospital’s CTU served as the control. The 15 min PowerPoint presentation consisted of a review of the current guidelines for CS use for patients admitted with COPDE, with an emphasis on limiting the duration of CS use to 5 days. Data from preimplementation period were also presented, and the proportion of patients who conformed to the guidelines was highlighted.
Retrospective medical record review was conducted preimplementation (P1) (June 2013–February 2014) and postimplementation (P2) (March 2014–February 2015) for all patients, ≥18 years, admitted with a COPDE to the CTUs at the intervention and control hospitals (i-CTU and c-CTU, respectively). Pregnant patients were excluded. Exit prescriptions for patients discharged before 5 days were reviewed for the total duration of CS therapy. To determine the sustainability of the intervention, we also examined the records of patients admitted to both CTUs 3 months following the end of the intervention (P3) (February 2015–April 2015). The educational presentation was not given during P3.
The primary endpoint was the change in the proportion of COPDE admissions during which patients received the recommended 5-day course of CS at the end of P2 compared with P1. Variables were compared using χ2 or Wilcoxon-Mann-Whitney test as appropriate.
Results
During P1, there were 85 COPDE admissions (70 patients) on i-CTU and 55 on c-CTU (51 patients), and 87 (77 patients) admissions on i-CTU and 39 (35 patients) on c-CTU during P2. Patients’ characteristics were comparable between the two sites (i-CTU vs c-CTU: mean age 74.3 (SD: 10.2) vs 74.0 (SD: 12.3) years, p=0.99; 48.3% vs 48.8% female, p=0.99; 37.4% vs 40.7% active smokers, p=0.67%; and 14.2% vs 12.8% on home oxygen, p=0.99).
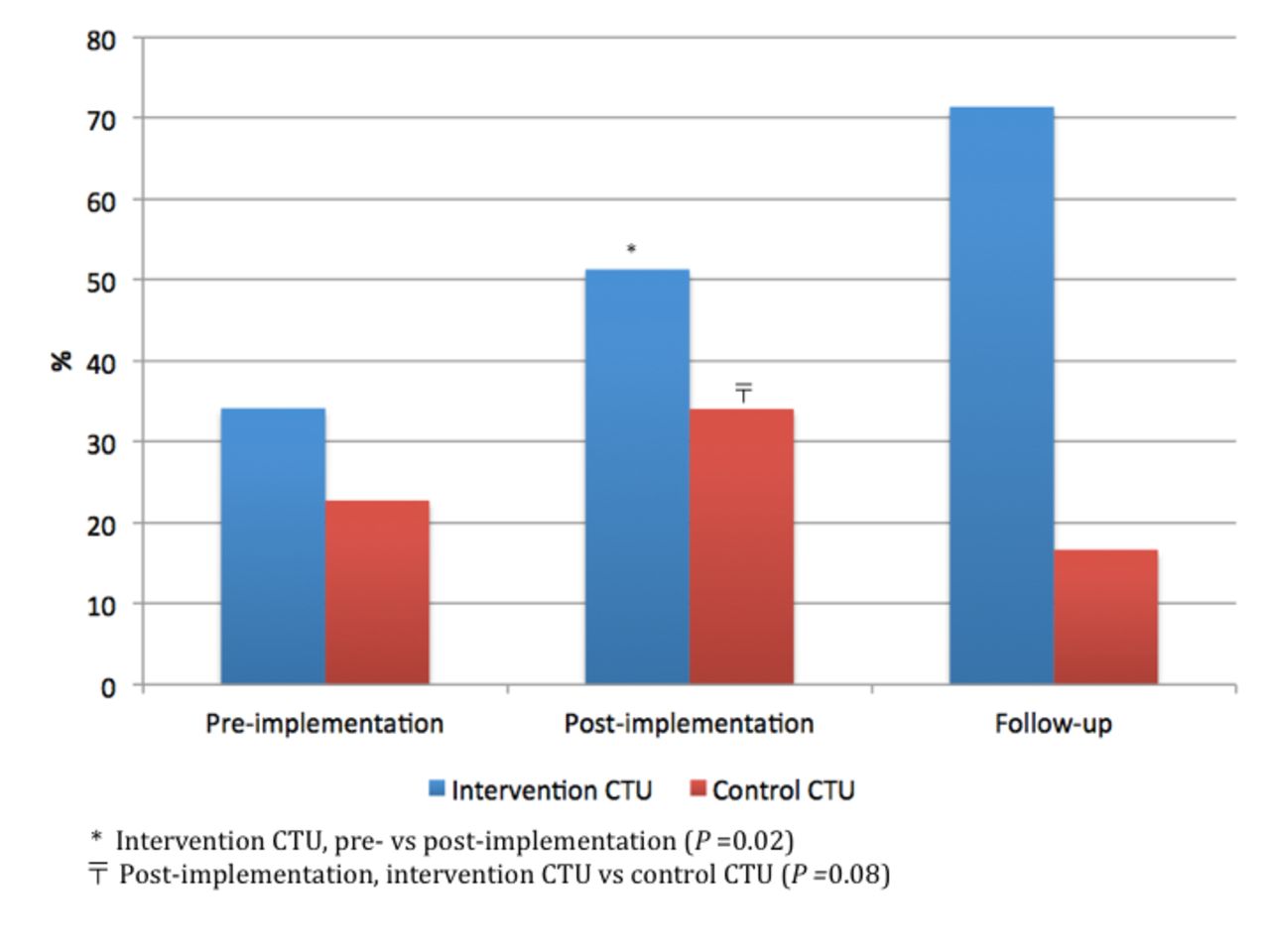
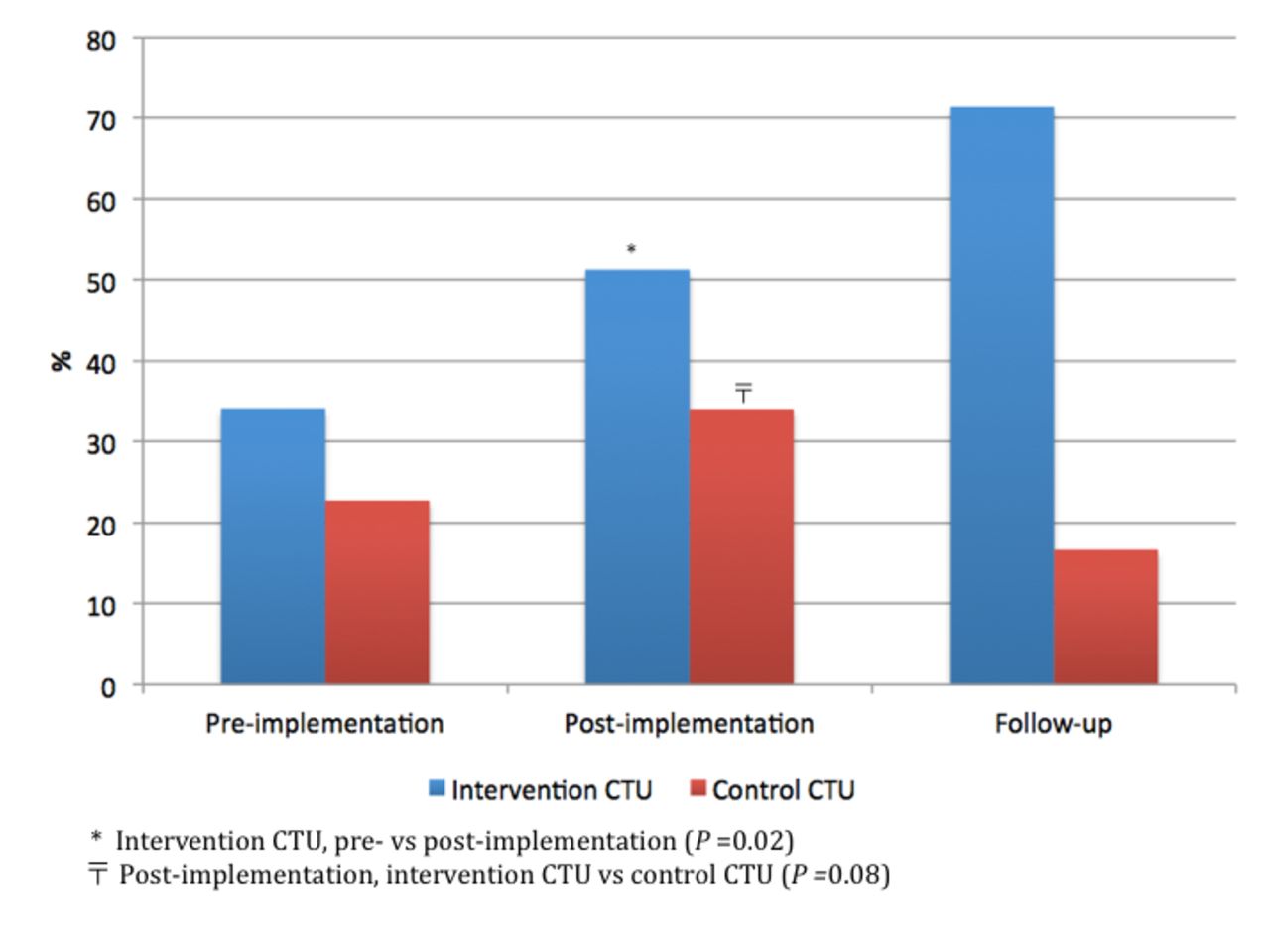
The median duration of CS use was 6 days for both i-CTU (range 0–38) and c-CTU (range 0–28) during P1 (p=0.47), and 5 days for both i-CTU (range 0–26) and for c-CTU (range 0–15) during P2 (p=0.89). During P1, 34.2% of COPDE on i-CTU and 22.8% on c-CTU were treated according to the recommendations. Following the intervention, there was an increase in the proportion of appropriately treated COPDE on i-CTU (51.3%, p=0.02), compared with no change on c-CTU (34.1%, p=0.15), with a trend towards optimal prescribing behaviour on i-CTU versus c-CTU (p=0.08) (figure 1). This effect was maintained during the 3-month follow-up period (i-CTU: 71.4%; c-CTU: 16.7%). Thirty-day readmission rates were similar and did not change following the intervention (i-CTU: 13.8% and c-CTU: 17.5% at the end of P2).
{kind=link}
Proportion of chronic obstructive pulmonary disease exacerbation admissions during which patients received 5 days of corticosteroids. CTU, clinical teaching unit.
Discussion
Implementation of a short educational presentation led to sustained improvement in a durable adherence to guidelines with regard to the duration of CS therapy in COPDE.
Our results contrast with those published by Hope et al,5 who documented no improvement in prescribing behaviour following a pharmacist-led educational intervention on CS guideline adherence. Although ensuring adherence to guidelines can be challenging, the success of our intervention may be due to the reliance on peer-to-peer teaching, which is at the heart of the CTU model. As the junior residents rotate through the CTU again as junior or senior residents, the practice becomes embedded within the CTU culture and may represent a strategy to translate clinical guidelines into sustainable practice.6 However, our intervention focused only on one aspect of improving prescribing practices, as we wanted to study the effect of peer-to-peer teaching. We did not include individual feedback to prescribers or CTU pharmacists involvement in continued guidance or instruction. Our system also does not have a physician order entry system to allow for automated suggestions. These factors may be responsible for nearly 50% of patients in the i-CTU not receiving guideline-adherent CS therapy for COPDE.
Footnotes
Contributors CM contributed to the conception, design, analysis, data interpretation, drafting and revision of the manuscript. JH contributed to the conception, design, analysis and interpretation of the data. DJ contributed to the conception, design, data interpretation, drafting and revision of the manuscript. LG contributed to the conception, design, data interpretation and manuscript revision. SNM contributed to the conception, design, analysis, data interpretation, drafting and revision of the manuscript. DJ accepts full responsibility for the work and/or the conduct of the study, had full access to all the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SNM: research grants paid to the institution (Amgen and Merck).
Patient consent Not required.
Ethics approval McGill University Health Centre Institutional Review Board ethics approval was obtained.
Provenance and peer review Not commissioned; externally peer reviewed.