Article Text

Abstract
Non-steroidal anti-inflammatory drugs (NSAIDs) are associated with more emergency hospital admissions due to adverse drug reactions than any other class of medicine. One way to tackle this is to ensure that patients understand how to take their NSAIDs in the safest way possible. The aim of this project was to ensure that key safety information is given to every patient, every time an NSAID is sold or dispensed. The project started as part of the Scottish Patient Safety Programme’s Pharmacy in Primary Care Collaborative. An NSAIDs bundle was developed, tested and implemented using the Model for Improvement as a framework, including multiple Plan, Do, Study, Act cycles. The bundle, and associated improvement package, was developed during phase I of the project and tested by seven teams (five pharmacies and two dispensing practices). Phase II tested the spread of the defined improvement package across an additional five community pharmacies and eight dispensing general practitioner practices. The project has resulted in the development of a simple package to improve communication with patients about NSAIDs, which should enable patients to take NSAIDs safely. Three key safety messages were developed, typical for a care bundle approach, and simple tools were employed to ensure every patient received these three key messages every time. The project aim of 95% compliance with the NSAIDs bundle within the seven initial sites by December 2015 was achieved (when an exclusion was applied). The spread of the defined improvement package to a further 13 sites was achieved by December 2016. By December 2017, all 81 community pharmacies in National Health Service (NHS) Highland had agreed to implement the NSAIDs bundle. In June 2018, a national NSAIDs bundle, based on the NHS Highland work, was introduced in community pharmacies across Scotland. We also believe that the approach could be replicated for other high-risk medicines.
- pharmacists
- quality improvement
- medication safety
- patient education
- continuous quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Section 1
Problem
Non-steroidal anti-inflammatory drugs (NSAIDs) cause preventable harm; they are associated with more emergency hospital admissions than any other class of medicine.1 2 Adverse events with NSAIDs are most commonly associated with gastrointestinal (GI) ulceration and bleeding, but can also cause cardiovascular and renal complications.3–5 NSAIDs are one of the most commonly prescribed drug groups in the UK. Within the National Health Service (NHS) Highland in 2016, 12.35% of the population had one or more prescriptions for an NSAID (approximately 41 000 out of 332 000 people). In total, there were 117 000 prescriptions for NSAIDs, costing approximately £670,000.6 Given the frequent use and levels of harm, there is a significant burden associated with NSAIDs to both patients and healthcare organisations.7 This also suggests there is significant opportunity for quality improvement.
Importantly, much of the harm can be prevented if NSAIDs are used appropriately. For example, careful consideration should be given when prescribing NSAIDs for the elderly due to an increased risk of adverse events due to polypharmacy and associated alterations in pharmacokinetics.8 There are also increased risks of GI disturbances associated with specific NSAID formulations and higher drug dosages.9 While safe prescribing is an essential element in reducing NSAID adverse events, there are also important interventions associated with patient self-care and administration. The focus of this project was to ensure patients had the correct information to enable them to take their NSAIDs as safely as possible.
NHS Highland covers a population of 332 000 people and is spread over 32 500 km2, which presents unique challenges in terms of equity of access to pharmacy services and associated medicine information. Pharmacists have a key role to play in the provision of medicines safety information, particularly in remote and rural areas.10 In remote communities, general practitioner (GP) practices often provide dispensing services in the absence of community pharmacies. Safety information about NSAIDs may be regarded as particularly crucial in remote areas where patients have reduced access to services and lengthy transfer times to hospital if an adverse event occurs. A local audit also revealed that patients in remote areas report buying more medicines online and do not always receive appropriate safety advice. Pharmaceutical community care within NHS Highland includes 81 community pharmacies (of which 52 are remote and rural) and 39 dispensing practices (37 of which are remote and rural).11 This project focused on remote and rural locations commencing with five community pharmacies and two dispensing GP practices (phase I), extending to a further five community pharmacies and eight dispensing GP practices (phase II) by December 2016. The work was initiated as part of the Scottish Patient Safety Programme (SPSP) Pharmacy in Primary Care Pilot, of which NHS Highland was one of four pilot sites.12 NHS Highland has an established history of improvement work in relation to the SPSP and Lean improvement methods, referred to locally as the Highland Quality Approach.
Background
NSAIDs are commonly used for their analgesic and anti-inflammatory properties in the management of pain relief.9 They are often selected over simple paracetamol due to both their lasting analgesic and anti-inflammatory effect. NSAIDs work by blocking cyclo-oxygenase (COX) enzyme, which reduces the production of prostaglandins. There are two types of COX: blocking COX-2 reduces the production of prostaglandins associated with inflammation, but blocking COX-1 reduces the production of prostaglandins which are important in protecting the gastric mucosa from the potential corrosive effects of stomach acid. Therefore, NSAIDs, which block the actions of COX-1 increase the risk of GI harm, such as ulcers and bleeding.13 These adverse events can also be reduced by patient self-management measures, including ensuring NSAIDs are taken with or after food, and early recognition and reporting of side effects.9 14 Another possible adverse event is an acute kidney injury when NSAIDs are taken while the patient is dehydrated.15 NHS Highland had previously produced a Medicine Sick Day Rules Card, which details the medicines that should be stopped temporarily during periods of sickness and diarrhoea, with NSAIDs being one of these.16
Yet, knowledge of the risk factors associated with NSAIDs is limited within the general population. A study exploring patients’ knowledge of commonly used medications found that only 17.7% were aware of the maximum recommended dose of ibuprofen and only 14% were aware of the contraindications.17 Others have found that many people using NSAIDs are largely unaware of the potential side effects.18 This evidence is further supported in a survey, which found that less than 50% of participants knew the potential side effects of NSAIDs despite the majority of the sample being well educated, with adequate functional health literacy.19
A recent study found that there was significant variation in patients receiving information from pharmacies, with those collecting new prescriptions receiving no advice on 58.1% of occasions.20 A study specifically examining public awareness of NSAIDs found that less than 35% of customers had been informed by a doctor or a pharmacist about their use, interactions and/or potential adverse effects.21 Research has shown that pharmacists can improve medication safety by providing patient education about high-risk medicines.22 23 Research has suggested that using an information sharing tool may increase usage of written information by patients.24 Community pharmacists and dispensing practices are well placed to address this knowledge gap due to their location and frequent interactions with patients, particularly in remote and rural settings.
The Institute for Healthcare Improvement created the concept of a bundle to deliver aspects of evidence-based practice. A bundle can be defined as a small group (usually no more than five items) of evidence-based interventions in relation to a specific aspect of care, which, when executed together, result in better patient outcomes.25 Given that there are simple interventions that would likely reduce patients’ risk of adverse events associated with NSAIDs, the team decided to devise, test and implement a NSAIDs bundle.
Section 2
Measurement
The aim of the first phase was to achieve 95% compliance with the NSAIDs bundle by seven community pharmacy and dispensing GP practice teams within NHS Highland by December 2015. The aim of the second phase was to test the spread of the NSAIDs bundle using a defined improvement package to a further 13 community pharmacy and dispensing practice teams by December 2016. The following operational definition to measure bundle compliance was established: divide the number of people meeting the bundle standard by the total number of people in the sample and multiply by 100. In accordance with best practice, the measure was initially tested in a single pharmacy for 1 month to determine the feasibility of data collection.26 A single staff member was trained on the bundle and data collection procedures (November 2014). This test identified that trying to apply all elements of the original bundle was problematic because the final two items within the bundle related solely to the prescribing of NSAIDs, whereas the other three could be applied to any supply of an NSAID (over the counter or on prescription). Therefore, a decision was made to separate these into two bundles. This project specifically reports on the patient information bundle (see online supplementary file 1: NSAIDs bundle) and not the prescribing bundle.
Supplementary file 1
Phase I (December 2014 to December 2015) involved seven teams (five pharmacies and two dispensing practices) recording bundle compliance for a random sample of 10 patients a fortnight. A standardised data collection tool, with a dichotomous ‘yes’ or ‘no’ response, was developed and tested to ensure consistency of data collection (see online supplementary file 2: improvement package for details of data collection tool). Data were submitted monthly to the Quality Improvement Facilitator for collation. The Pharmacy Data Analyst created run charts. The Quality Improvement Facilitator returned the charts to the teams to discuss and display.
Supplementary file 2
During phase II (January 2016 to September 2016), the same type of data was collected by the additional five community pharmacies and eight dispensing GP practices. The frequency of data collection was changed to weekly instead of fortnightly, as teams reported that this reduced confusion over whether or not the data required to be collected.
While bundles are designed around the concept of ‘all or nothing’,25 data were stratified into the individual elements of the NSAIDs bundle to highlight the progress or, otherwise, of specific aspects of the bundle during testing. Therefore, the following elements were also calculated as a process measure: percentage of patients informed to take NSAID with or after food, percentage of patients informed to report any GI side effects to their pharmacist or GP, and finally, the percentage of patients given a Medicine Sick Day Rules card. All data were collected by peer observation and reported anonymously. Discrete observation within teams may assist the team to take ownership of the observations and data.27
Design
Phase I: development of bundle and testing of data collection
The NSAIDs bundle was developed by the NHS Highland Scottish Patient Safety Programme Pharmacy in Primary Care Steering Group, which comprised representatives of community pharmacy, GP practices, NHS Highland and a patient representative. The initial step was to produce a driver diagram (see online supplementary file 3: driver diagram). A draft bundle was consulted on widely within NHS Highland pharmacy team and local contractor representative committees. Guidance was also received from the national SPSP Pharmacy in Primary Care Collaborative Steering Group.
Supplementary file 3
The bundle was tested in one pharmacy for 1 month before testing across seven teams (five pharmacies and two dispensing practices). Each pharmacy identified one or two people to lead the project, and these were the ‘away’ team. The away team participated in a learning event hosted by the National SPSP Pharmacy in Primary Care Collaborative, which covered an introduction to the Model for Improvement (MFI), the NSAIDs bundle and measurement. The team were encouraged to test and devise strategies to assist in implementing the NSAIDs bundle. Another learning event was held by WebEx 3 months after the project began, the aim being for teams to share learning with each other. In addition, the project Clinical Lead and Quality Improvement Facilitator visited each of the seven sites to provide support within the first few months of the project.
Phase II: further testing the spread of the NSAIDs bundle
From January 2016 to September 2016, the bundle was spread to a further five community pharmacies and a further eight dispensing GP practices. The teams were given the bundle, an improvement package (see online supplementary file 2: improvement package) and tools developed by the other teams during phase I. The teams were encouraged to test and devise their own strategies to assist in implementing the NSAIDs bundle. All data were collected on yes/no grids and sent to the facilitator weekly to plot on a run chart: again, individual sites were provided with their own run charts as well as a Highland-wide chart.
Additional data were collected in the eight dispensing GP practices only to determine whether patients understood the information given. The reason for exploring this in dispensing practices only was because advising patients on medicines was a new role for practice staff, whereas it was something community pharmacy staff were more used to.
The project Clinical Lead discussed the project with all 13 sites by telephone, followed up by a visit to launch the project. The Quality Improvement Facilitator also visited the five pharmacy sites. Ongoing support was provided by both the clinical lead and facilitator throughout phase II.
Strategy and improvement cycles
The entire project was structured using the MFI28 as selected by the national SPSP Pharmacy in Primary Care Collaborative Steering Group. The Steering Group provided coaching at the initial learning events for the collaborative, both for the NHS Highland project steering group and for the participating front-line teams. The overall structure of the project was based on part one of the MFI, often referred to as the three thinking questions. First, what are we trying to accomplish; second, how will we know that a change is an improvement; and third, what change can we make that will result in improvement? Teams were provided with a template of the MFI and encouraged to undertake Plan, Do, Study, Act (PDSA) cycles throughout the project (part two of the MFI). The following paragraphs summarise some key PDSA cycles, reported as a combined cycle from multiple teams.
PDSA cycles regarding training and awareness
All of the teams developed some form of NSAIDs training. The aim of the first PDSA cycle was to test this NSAIDs training. The hypothesis was that bundle compliance would improve if staff had an awareness and understanding of the bundle. Results of the first PDSA highlighted that training helped to improve bundle use, but that training was time consuming and not specific enough. In addition, teams which had only used verbal training identified that backing this up with written information would have been useful. Subsequent PDSA cycles and shared learning between the sites via a WebEx learning event helped refine and develop a 10 minute NSAIDs training package, delivered verbally with written resources. There is evidence to suggest that educational interventions alone do not usually sustain change.29
PDSA cycles regarding visual prompts
The aim of these PDSA cycles was to establish an effective strategy to remind busy staff to complete the bundle. Initial testing of highlighting the bundle on dispensing labels found that while this strategy helped on occasions, it did not always work, as people can purchase NSAIDs over the counter, as opposed to receiving a prescription. The next stage of testing was to use Post-It notes on both dispensary shelves and point of sale tills as a reminder; however, these tended to fall off. Further testing and learning from PDSA cycles resulted in the creation of an NSAID sticker for use on the dispensary and counter shelves at the points of sale to act as a visual prompt to provide the patient with the bundle elements. The use of visual prompts has been used to effectively influence staff behaviour in other improvement projects.30
PDSA cycles NSAIDs information cards
The aim of this ramp of cycles was to test whether patients found a NSAIDs Information Card useful (see online supplementary file 4: NSAIDs information card). The idea for creating an information card came from the patient representative on the local SPSP Pharmacy Steering Group. The hypothesis was that giving patients written information would help them remember the three important messages. While patients and customers reported the card was useful, the card had other beneficial effects. Learning from these cycles also found that the information card aided staff confidence in delivering the elements of the NSAIDs bundle. The NSAIDs information card was subsequently used as an aide memoire for staff (especially for less confident or new staff) as well as being a tool to reiterate the verbal messages. These were also found to be useful for housebound patients who do not collect their own prescriptions from pharmacy.
Supplementary file 4
Section 3
Results
Phase I results
Figure 1 shows the run chart displaying each of the three elements of the NSAIDs bundle. The monthly percentage compliance is the combined results for all seven pilot sites. It is not possible to annotate the combined results as each site tested various strategies to improve NSAID use at different points along this run chart. The first strategy for all sites was staff training.
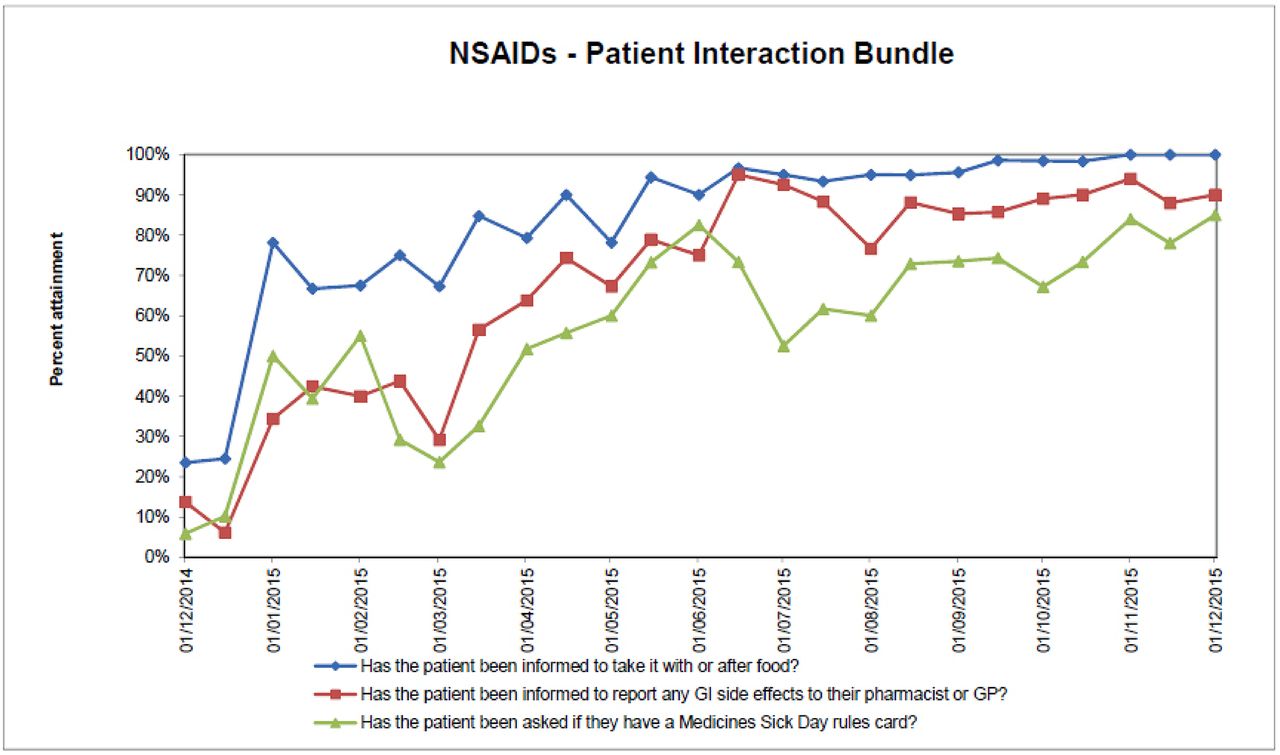
Run chart displaying three stratified elements of the NSAIDs bundle during the development phase. GI, gastrointestinal; GP, general practitioner; NSAID, non-steroidal anti-inflammatory drug.
Both bundle elements of informing the patient to take the NSAID with or after food, and the reporting any GI side effects show a steady improvement in compliance. The medicine sick day rules data demonstrate more variation. Where NSAIDs are sold in pharmacies for self-limiting conditions (eg, single episode of headache), it is not necessary, or appropriate, to provide the medicine sick day rules advice. The advice is only needed for people who take NSAIDs long term. Therefore, the target of 95% was agreed as impossible and inappropriate to obtain when over-the-counter sales were included.
Phase II results
In phase II, an improvement package of the strategies defined within year 1 to aid implementation of the NSAIDs bundle was spread to the new sites. Figure 2 shows the run chart displaying weekly data for the initial 10 weeks of the NSAIDs bundle implementation after receiving the improvement package. These sites demonstrated a very quick improvement in ensuring that patients received the three key messages—a baseline figure of 10% to above 90% in the space of a few weeks for bundle elements 1 and 2. For element 3 (on medicine sick day rules), the figure was around 70% in community pharmacy (which was appropriate, as explained above) and above 95% in dispensing practices (where there are no sales of medicines, just dispensing of prescriptions).

Run chart displaying weekly data after the introduction of the non-steroidal anti-inflammatory drugs (NSAIDs) bundle implementation package.
Phase II, part two results (dispensing practices only)
For dispensing practice staff, advising patients about medicines was a completely new role. Before this project, dispensing practice staff checked patients’ demographic details before handing out medicines, but did not routinely provide advice about how to take or use medicines. Therefore, additional data were collected at eight dispensing practices to assess whether patients’ knowledge about how to take their NSAIDs was improved by the intervention.
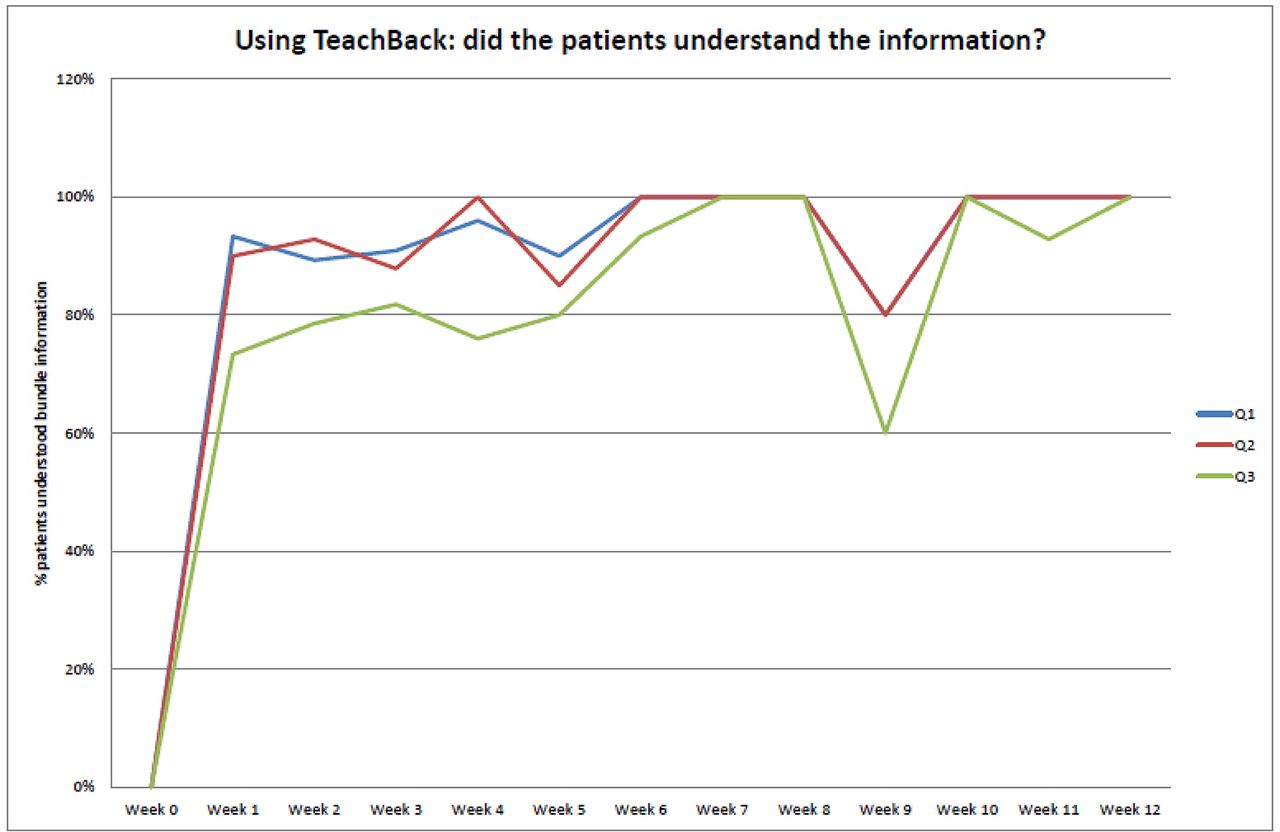
Dispensing practice staff were trained by the project Clinical Lead on how to use TeachBack, a recognised approach to check patient understanding of information given.31 Figure 3 shows staff-reported responses as to whether patients understood the information given, based on patient responses to a TeachBack approach. A dip is seen at week 9: staff reported that this was due to a holiday period when different staff were working in the dispensary to provide holiday cover. This highlighted the importance of ensuring all staff who work in the dispensary receive appropriate training.
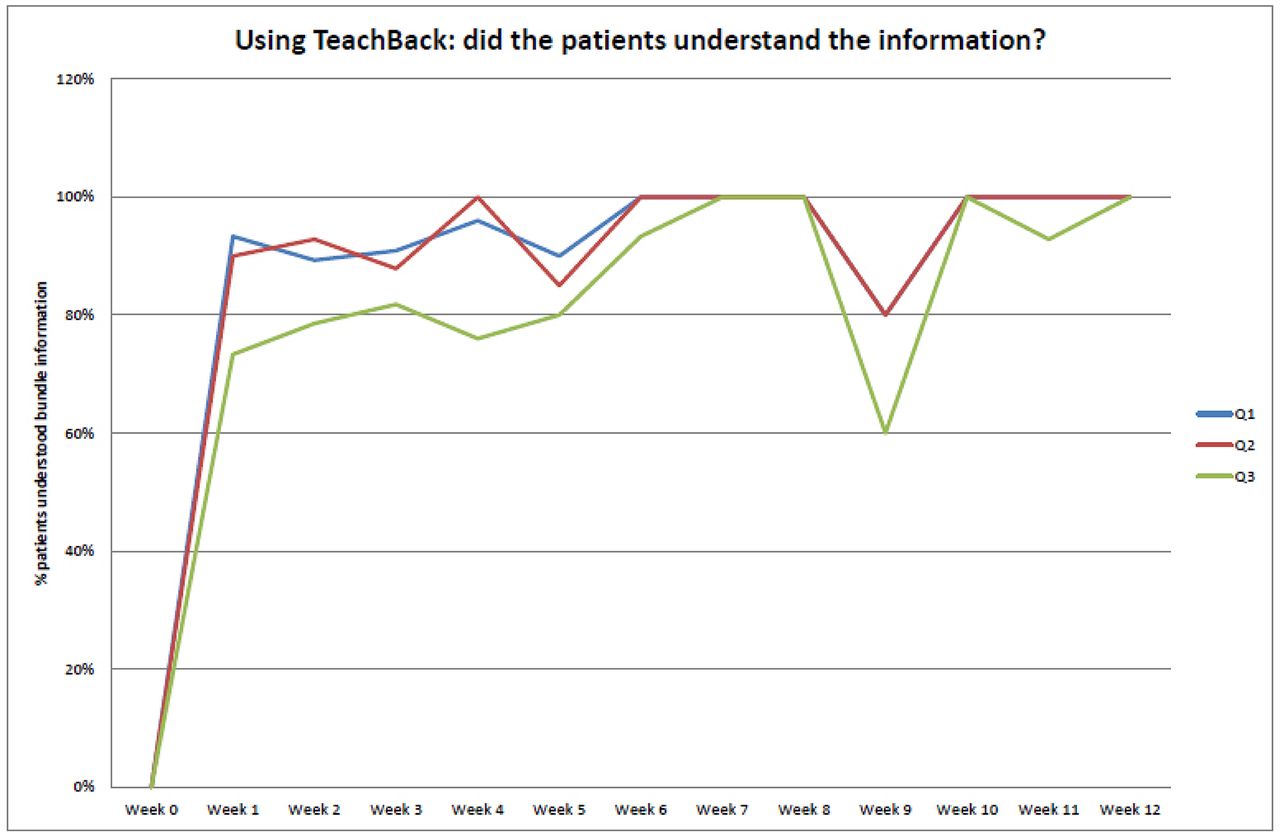
Run chart displaying weekly data on patient understanding of the non-steroidal anti-inflammatory drugs (NSAIDs) messages after the NSAIDs bundle package was introduced.
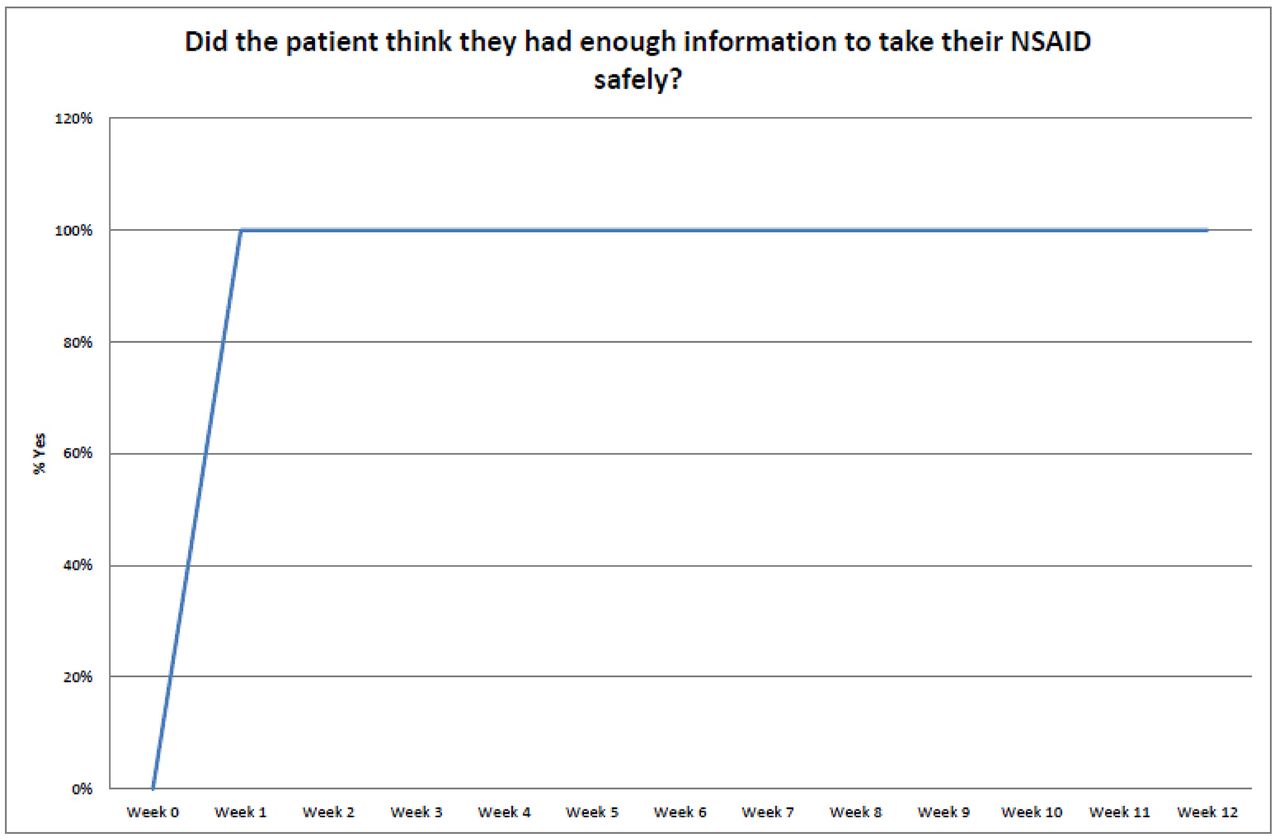
In addition, patients at the eight dispensing practices were asked to rate overall whether or not they had sufficient information to take their NSAID safely. This was achieved by asking the patient to anonymously place a ball into a ‘yes’ or ‘no’ box. Balls were counted by practice staff at the end of each week. The results are shown in figure 4, with a universally positive response from patients sustained over a 12-week period, demonstrating that dispensing practice staff were able to successfully deliver advice on NSAIDs following the introduction of the NSAIDs bundle and improvement package.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chart displaying weekly outcomes data on whether patients reported having enough information to take a non-steroidal anti-inflammatory drug (NSAID) safely after the NSAIDs bundle package was introduced.
Lessons and limitations
The project aim was to ensure that key information is given to every patient, every time an NSAID is sold or dispensed, so that patients know how to take NSAIDs safely. For this to be achieved, there was a need to make the ‘right thing, the easy thing to do’. This was achieved by devising an NSAIDs bundle. We believe one of the key elements of the project’s success was encouraging the teams to test and devise strategies to assist in implementing the NSAIDs bundle within their own context. The approach empowered the entire pharmacy team, rather than relying solely on the pharmacist, which is likely to have increased reliability in busy community pharmacies. It also enabled the NSAIDs bundle to be used in dispensing practices, where there is no pharmacist. The development of an improvement package with strategies driven by front-line staff is likely to have improved buy-in to the project and front-line ownership.27
The team found PDSA cycles useful in terms of iterative testing and learning before attempting to spread the intervention more widely. The PDSA approach is also likely to have contributed to increasing staff confidence to test various strategies to support use of the NSAIDs bundle. This may be due to the psychological safety inherent in small tests of change, as opposed to full-scale implementation.32 We believe that the approach taken in this project was the correct one; small tests of change with seven teams, developing an improvement package driven by front-line staff, testing the spread of that package on a small scale and then spreading more widely.
The main project limitation was in relation to outcome data. Although the project delivered improvements to processes in patients receiving consistent messages around NSAID safety, we have not been able to demonstrate improvements in terms of outcome measures. Our ultimate aim was to reduce the number of hospital admissions due to adverse effects of NSAIDs, specifically GI effects and acute kidney injury. The reasons we have not been able to demonstrate this outcome measure is twofold: the initial pilot sites were small in number, so any action would not have had a statistically significant effect on hospital admissions; and the adverse events associated with NSAIDs have multifactorial causes, resulting in challenges in determining cause and effect.33 Now that the bundle is being rolled out across all locations with subsequent larger samples, a next step is to measure whether it has an impact on the number of hospital admissions due to adverse effects of NSAIDs.
Another limitation is that data were collected on a sample basis, so there is a potential for an inaccurate reflection of the overall picture. However, this bias is unlikely as all sites reported similar data. Although bias cannot be excluded due to the use of observation data, on balance this approach was selected due to the necessity for engagement, ownership and trust with all participating teams.
Additionally, the problem with achieving compliance with the medicine sick day rules element of the bundle in community pharmacies (as already described) could have been overcome if the bundle had been adjusted to include an exclusion element. Responses to this element of the bundle would then be ‘yes’, ‘no’ and/or annotated with an ‘E’ for exclusion. This would have enabled a more accurate reflection of bundle implementation.
Patients in remote and rural areas rely on dispensing practices for supply of medicines, and therefore it is essential to ensure that medicines safety information is provided to these patients, as it should be to patients in urban areas via community pharmacies. A significant improvement achieved within the project was the transformation of the role of dispensing practice staff in remote and rural areas. Historically, dispensing practice staff in these areas issued medicines without providing any verbal advice. Although advice was provided within the GP consultation, this advice was not reinforced at the point of dispensing or given at all during subsequent issues of repeat medicines. Through this project, dispensing practice staff reported feeling empowered for the first time to provide key medicines safety advice. Through this project, they started to provide advice on NSAIDs and achieved compliance with the bundle. This empowerment extended beyond NSAIDs, for example, drawing patients’ attention to pre-printed warning labels on dispensed medicines labels.
While improvement work is context specific,34 sharing the strategies tested and subsequently defined as an improvement package in phase I with sites in phase II accelerated the bundle implementation in phase II. An improvement pack was designed for all remaining sites to assist them, although the opportunity for teams to devise their own strategies for implementation continues to be encouraged.
Conclusion
In summary, it was clear that before this project, patients were receiving limited information about the interventions to reduce the risk of NSAIDs adverse events. The consequences of these adverse events can be serious for both patients and healthcare resource. Yet, simple interventions, such as the NSAIDs bundle reported in this project, have the potential to reduce these events.
This initiative achieved an improvement in the consistency of NSAIDs patient information through a defined improvement package. That package has now spread to all pharmacies in NHS Highland. Pharmacies in four other Scottish NHS boards have begun testing and using the NSAIDs bundle. In November 2017, it was announced that a bundle around improving communication with NSAIDs would be included in the national community pharmacy contract in Scotland from April 2018.35 In June 2018, a national NSAIDs communication bundle was published, which is based on the NHS Highland NSAIDs improvement package.36
We believe that this project has implications beyond NSAIDs. It is well known that many medicines have adverse effects that can be prevented if patients know how to take them properly and take actions to mitigate the risk.22 Using PDSA cycles and a bundle approach to communicate key safety messages could be replicated for other high risk medicines.
Acknowledgments
Staff and patients of all community pharmacies and dispensing practices who participated in this project, especially the initial seven teams who developed the improvement tools that went on to form a key part of the improvement package (five community pharmacies in Brora, Ullapool, Kyle of Lochalsh, Islay and Lochgilphead (Argyll Pharmacy) and two dispensing GP practices in Scourie and Kinlochbervie, and Acharacle). Also, Mary Morton, Catriona Sinclair, Fiona Duff, John Braynion (SPSP Pharmacy in Primary Care Steering Group; support throughout the project), Fiona Riddell (Community Pharmacy Business Manager, NHS Highland; support for phase III), Jill Gillies and Andrea Smith (SPSP Pharmacy in Primary Care national team; support for phases I and II), Ros Gray and Neil Houston (Scottish Quality and Safety Fellowship, support for phase II), Elaine Mead (Chief Executive, NHS Highland; Executive Sponsor of entire project), Ian Rudd (Director of Pharmacy, NHS Highland; support throughout the project) and Rob Polson (Subject Librarian, for assisting with literature searching).
References
Footnotes
Contributors CM designed and managed the project, and was the project Clinical Lead. CM, TB and HMcD facilitated all aspects of the project, including site support for data collection, strategy testing and PDSA methodology (HMcD initially and TB subsequently). Both TB and HMcD inputted and collated data. TB analysed the data. CM and MB drafted the paper and all authors revised before agreeing the final version.
Funding NHS Highland received funding from the Scottish Patient Safety Programme to undertake the initial pilot. All seven sites in the initial pilot received funding to enable staff members to attend learning events as part of the pilot. All community pharmacies in NHS Scotland are funded through the national pharmacy contract to undertake some quality improvement work and the package developed in this project aimed to meet this requirement.
Competing interests None declared.
Patient consent Not required.
Ethics approval This work met criteria for operational service improvement work exempt from research ethical review.
Provenance and peer review Not commissioned; externally peer reviewed.