Article Text

Abstract
Background In a busy stroke centre in Ireland, care for acute stroke was provided by a mixture of general physicians. In acute ischaemic stroke, speed is essential for good outcomes.
Aim To improve acute stroke services and decrease door-to-needle (DTN) time to less than 60 min by December 2016 in patients with acute ischaemic stroke who are eligible for intravenous thrombolysis.
Design: A quality improvement (QI) project was undertaken in a 438 bed, acute, university hospital.
Methods Mixture of qualitative and quantitative data collected. A process map and driver diagram were created. Interventions tested with Plan-Do-Study-Act cycles. Times compared between July and December 2015, January and July 2016, July and December 2016, when a new stroke team and pathway were introduced.
Results Between July and December 2015, the total number of ischaemic strokes was 216. 17 were thrombolysed (7.8%). Median door-to-CT (DTCT) time was 36 min (range 21–88). Median DTN time was 99 min (range 52–239). Between July and December 2016, there were 214 ischaemic strokes. 29 were thrombolysed (13.5%). 9 were seen directly by the stroke team during normal hours. With stroke team involvement, median DTCT time was 34 min (range 14–60) and DTN time was 43.5 min (range 24–65).
Conclusions This project led to a significant and sustained improvement in acute stroke care in our hospital with the use of quality improvement techniques. A comprehensive protocol, recurrent and ongoing staff education, and good communication helped to mitigate delays and further enhance care provided to patients presenting with stroke. The approach described may be valuable to the improvement of other services.’
- quality improvement
- hospital medicine
- healthcare quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Stroke is a leading cause of death and disability worldwide, and over 7000 people are admitted to hospital every year in Ireland with stroke.1 Currently, the recognised treatment for acute ischaemic stroke is intravenous thrombolysis with alteplase, administered with greatest effect and safety within 4.5 hours from symptom onset.2
Time is brain in the face of the loss of 1.9 million neurons and 13.8 billion synapses for every minute delay in treating a large vessel ischaemic stroke.3 In an increasingly congested, acute hospital system, patients with stroke can fall foul of many avoidable interruptions in the swift assessment and treatment required for best outcomes. National guidelines recommend a door-to-needle (DTN) time of less than 60 min and its effect is greatest when given as early as possible.4
In one of the busiest acute stroke centres in Ireland, care for acute stroke was undertaken by a mixture of general physicians. Time is lost when inefficient processes are involved.
Aim
The primary aim was to decrease the DTN time to less than 60 min by December 2016 in patients with acute ischaemic stroke who are eligible for intravenous thrombolysis.
Methods
Design
This project was designed as a quality improvement project with a functional, weak matrix-type structure. This is a hybrid model overlaid on the regular functioning of the hospital.
Setting
The project was conducted in a 438 bed, acute, Irish university hospital. Until July 2016, the medical team on call for the day reviewed all patients with suspected stroke. At the time, the CT scanner was located outside of the Emergency Department (ED).
Local data from 2015 demonstrated that the DTN time was a median of 99 min. Significant delays were occurring in the pathways and processes of treatment after arrival to hospital at several stages, including referral, assessment, imaging and administration. Prior to the beginning of the project, a paper based, acute ischaemic stroke protocol had existed within the hospital.
At the beginning of this project, CT cerebral angiograms were not routinely performed in the context of acute ischaemic stroke and many radiographers required extra training for this procedure.
Ethics
Ethics committee review was not required for this project as it was a quality improvement project for already existing practices and treatments in the hospital.
Intervention
DTN time was chosen as a key performance indicator (KPI) that could be effectively improved and potentially lead to better patient outcomes and could be used as a marker of the efficiency of the pathway.
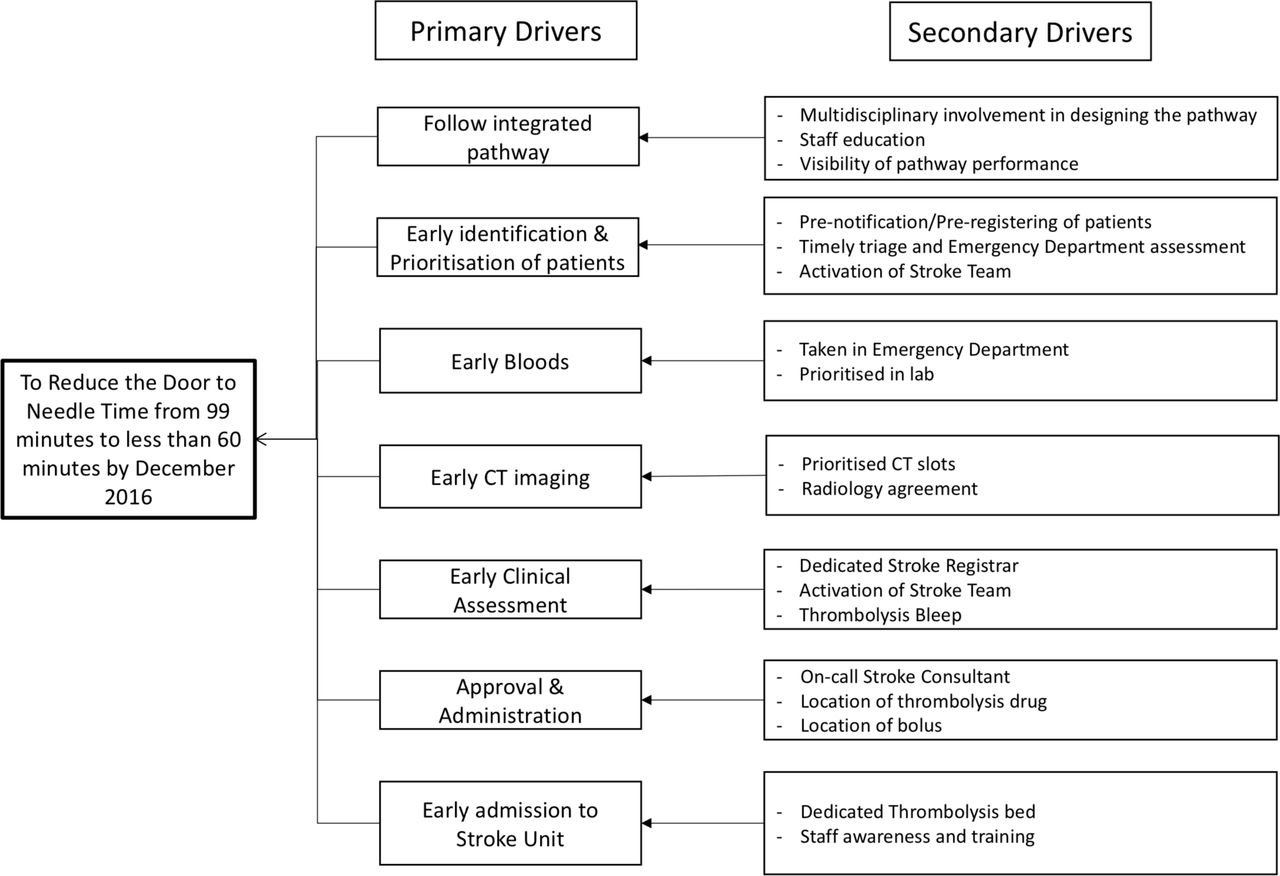
A process map was created outlining the steps in the patient journey from arriving in the ED to receiving treatment (figure 1). A driver diagram was produced to highlight the seven primary drivers for improvement (figure 2). The primary drivers were: (1) early identification and prioritisation of patients, (2) follow an integrated pathway, (3) early clinical assessment, (4) early bloods, (5) early CT imaging, (6) approval and administration, and (7) early admission to the stroke unit. Changes were implemented on a model of rapid Plan-Do-Study-Act (PDSA) cycles.
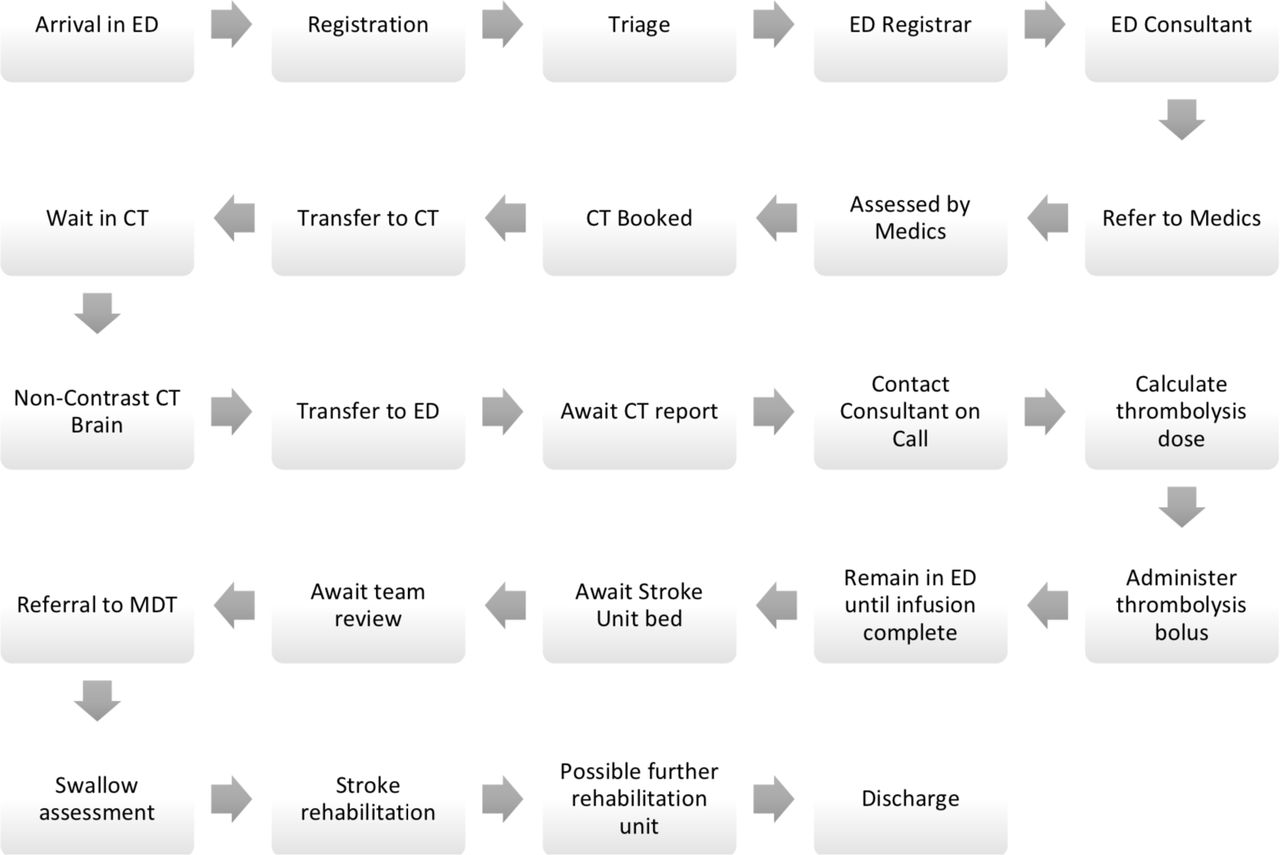
Process map. ED, emergency department; MDT, multidisciplinary team.
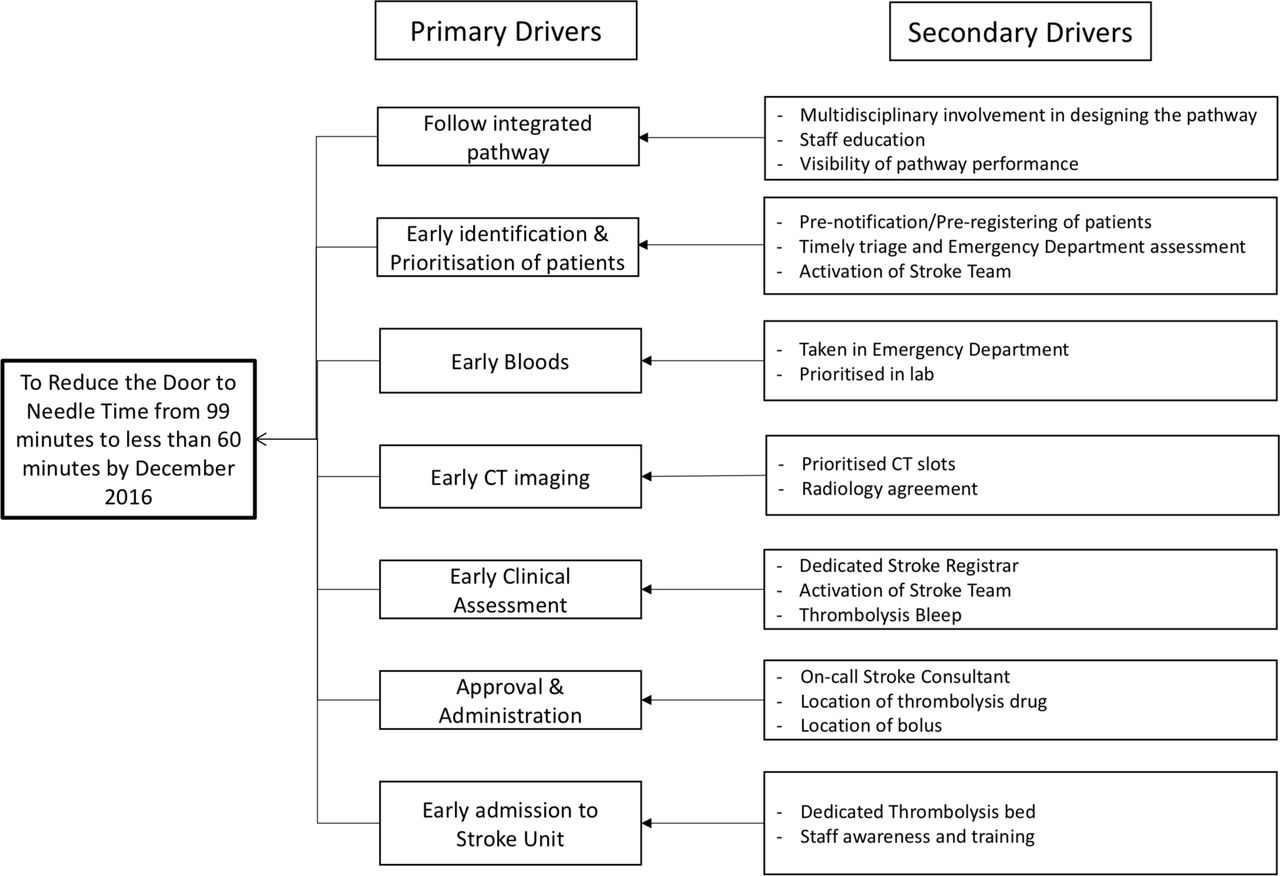
Driver diagram. ED, emergency department.
Follow an integrated pathway
The acute ischaemic stroke protocol was revised and during the course of the project many different versions were produced.
Included were changes for booking CT scans and transfer procedures. For example, if a porter was not immediately available to transfer the patient to the Radiology department, the stroke team would transfer the patient themselves.
New step-by-step decision algorithms for thrombolysis and thrombectomy were included so that, in the absence of the stroke team or out-of-hours, any doctor would be able to quickly and easily follow the steps required. PDSA cycles were employed to assess how each iteration performed.
Other sections added included management of adverse events, calculating an Alberta stroke programme early CT score and modified Rankin Scale (mRS). The patient information pages were made easier to understand and explain for both patients and staff. While thrombectomy is not carried out at the study site, an algorithm, information and contact details for the neuroradiology specialist centres were included.
Early identification and prioritisation of patients
Preregistration of patients before their arrival in the ED was not possible with the electronic system available and so CT scans could not be booked before arrival.
Once notified by an incoming ambulance, ED triage notified the ED registrar and the stroke team. The patient was brought straight to the resuscitation room. Recognition of the urgency of stroke and overlapping of tasks helped speed patients through the initial ED section of the pathway. Through PDSA cycles, other iterations of this pathway where ED staff did not play as central a role resulted in longer times.
Early bloods
A standardised set of bloods were drawn for testing, labelled as urgent and processed rapidly by the laboratory. Unless a specific suspicion existed, for example, as to the use of anticoagulant medication, the results were not to delay the administration of intravenous thrombolysis if the patient was otherwisesuitable.
Early clinical assessment
A post for a stroke registrar was created and they carried a bleep specifically for stroke calls. The stroke clinical nurse specialist (CNS) assisted the registrar on assessments. ED staff were informed, the bleep number was displayed prominently and the times when it would be active highlighted. Entries for the on-call stroke consultant as well as the stroke registrar were also made in the daily on-call list, accessed through the hospital intranet. The existence of the team and pathway was also widely publicised throughout the hospital, both informally and at consultant meetings.
The stroke team (CNS and registrar) provided rapid assessment of patients, both newly arrived in the ED and existing inpatients. Familiarity with the pathway, assessment criteria, contraindications and local procedures facilitated faster movement of patients through the various steps of the pathway.
Early CT imaging
On arrival in the Radiology department, a higher degree of urgency was attached to these patients and they were granted priority over those already waiting.
In the beginning, a non-contrast CT brain and a contrast CT cerebral angiogram were bundle-booked via the online National Integrated Medical Imaging System Radiology Information System. If there were no contraindications to thrombolysis seen on the non-contrast CT, the CT angiogram would automatically proceed. Concerns were raised regarding the capacity of the department to handle the number of CT angiograms that would result and that some patients may undergo unnecessary investigations. As a result, the two scans were decoupled and a checking step introduced whereby the stroke consultant must request the CT angiogram (usually via the stroke registrar) following review of the patient and the non-contrast images. Subsequent referral to the neuroradiology specialist centre was possible if suitable for transfer for thrombectomy.
Discussion and communication with both radiographers and consultant radiologists was a significant and crucial activity throughout the course of this project.
Approval and administration
A new on-call stroke consultant rota was devised, operated by nine consultants, and provided ready access 24 hours a day, 7 days a week to an experienced stroke physician who could make a final decision regarding thrombolysis and referral for thrombectomy. During normal working hours, the stroke team administered the bolus of intravenous thrombolysis while the patient was in the CT scanner.
Early admission to stroke unit
A bed in the hyperacute stroke unit was ring-fenced for patients who had acutely received intravenous thrombolysis. Once the initial bolus had been given and the infusion started in the Radiology department, the patient was transferred directly to this bed for post-thrombolysis monitoring and care.
Training sessions were held for the nurses on the ward so that they would be more comfortable in managing these patients as, until this time, patients had been returned to ED for completion of treatment. Completing the infusion on the ward was not immediately and universally accepted. A survey of opinions of all staff involved with stroke regarding their main concerns was carried out. Arising from this and a follow-up survey, further targeted training and education sessions were implemented on a monthly basis.
Governance structures
A monthly governance meeting for stroke was established in conjunction with a named consultant radiologist. Patients who had been thrombolysed, undergone thrombectomy, suffered complications, complex scenarios and deaths were discussed. This meeting provided opportunity for discourse on problems that had arisen with any aspect of the stroke pathway or a patient’s care.
Data collection
DTCT and DTN times were recorded for all patients who presented with symptoms of acute stroke and were subsequently treated with intravenous thrombolysis between July and December 2016. Data from the equivalent period in 2015 were used as comparator.
The time period of July–December 2016 was subdivided on the basis of whether or not the stroke team was directly involved in the initial care and treatment of a patient or if it was a general medical team.
Anonymous, written feedback was collected from staff via questionnaires.
From July to December 2016, mRS was recorded on admission and discharge and discharge destination noted.
Results
Between July and December 2015, the total number of ischaemic strokes was 216. Of these, 17 people received intravenous thrombolysis (7.8%). Median DTCT time was 36 min (range 21–88) and median DTN time was 99 min (range 52–239) (figure 3).

Door to CT (DTCT) and door to needle (DTN) times (July–December 2015).
Between July and December 2016, the total number of ischaemic strokes was 214, median DTCT time was 45.5 min (range 14–155), median DTN time was 82.5 min (range 24–210). Of these, 29 patients were thrombolysed (13.5%), of whom nine were directly seen by the stroke team during normal hours. One patient was omitted from comparison because they were thrombolysed outside of normal protocols on request of family.
Between July and December 2016, out-of-hours or without the involvement of the stroke team, median DTCT time was 50 min (range 20–155) and DTN time was 107.5 min (range 57–210). With stroke team involvement, median DTCT time was 34 min (range 14–60) and DTN time was 43.5 min (range 24–65).
Between July and December 2016, the median times for general medical team involvement were 32% and 59.5% higher for DTCT and DTN times, respectively, than the dedicated stroke team. Figure 4 shows a comparison between the DTN and DTCT times from those patients thrombolysed by general medical teams between January and July 2016 and the patients thrombolysed by the stroke team between July and December 2016.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Door to CT and door to needle time (min) in 2016 for thrombolysed patients prior to and after stroke team intervention; red line demarcates beginning of project.
Comparing the stroke team’s time with the general medical team between July and December 2015, median DTN time was 56% faster.
The staff survey received 29 responses. Forty-one per cent were nurses. Seventy-two per cent of respondents rated the stroke service as good or excellent. The main concerns expressed were training and policy documentation.
For July–December 2016, mRS data were similar for both groups. The average preadmission mRS, discharge mRS and discharge destinations are detailed in table 1.
Average mRS, discharge destination of patients for stroke team and general medical team, July–December 2016
During a follow-up period between July and December 2017, there were 145 patients with acute ischaemic stroke, of whom 21 were thrombolysed (14.5%). The median DTCT time was 26.5 min (range 11–98), the median DTN time was 67 min (range 19–155).
Discussion
This project indicates that it is possible to reduce DTN time for thrombolysis using quality improvement techniques, such as a streamlined pathway, dedicated stroke team and a stroke consultant available 24/7 for advice and decision-making leading up to thrombolysis and/or referral for thrombectomy.
Procurement of urgent neuroimaging was facilitated by a team who regularly communicated with the radiology staff. Figure 4 demonstrates a reduction in DTN time and also a reduction of the gap between DTCT and DTN times reflecting better procedures and the removal of redundant steps.
Many strokes happen outside of normal working hours when the stroke team of CNS and registrar were not available. Out-of-hours, there may be staff who are not as conversant with the protocol and therefore more hesitant at each stage. Out-of-hours CT scans had to be discussed between stroke and radiology consultants before approval. An off-site CT radiographer had to called in. Porter staff were not a factor as patients would be transported by a doctor and nurse if required.
To improve KPIs out-of-hours, several initiatives were undertaken since completion of the project. For example, a novel, simulated, stroke training programme was established in January 2018 to ensure that all medical registrars who partake in the on-call rota are stroke trained. There will be a CT-trained radiographer on site to reduce delays in getting the CT performed. A monthly stroke governance meeting has been established as well as quarterly meetings chaired by the Clinical Director focussing on KPIs. Finally, a new ED opened in 2017 which has a CT scanner located in the ED.
With a solitary registrar and stroke CNS, it is not uncommon for training days or annual leave to disrupt team continuity during the day and reduce the number of patients seen directly by the team. Extending hours of operation is one option but incurs extra investment costs. Instead, expanding stroke training as above should result in better value for money by utilising existing resources.
Observation of a follow-up period in 2017 revealed a sustained improvement in thrombolysis rates (7.8% in 2015, 13.5% in 2016, 14.5% in 2017). Median DTCT and DTN times also improved (2015: 36 and 99 min, respectively; 2017: 26.5 and 67 min, respectively).
A significant limitation of this project is the smaller number of patients thrombolysed directly by the stroke team. As mentioned, many of the patients who were thrombolysed happened to attend the hospital at weekends or at night during the period of study, when the stroke team was not operational. However, this does not reflect the far higher number of patients presenting to the ED with stroke-like symptoms that the team assessed directly but were not suitable for intravenous thrombolysis. These patients were more rapidly assessed, admitted, had neuroimaging, appropriate treatment started or were referred to another specialty. Thus, there were unintended beneficial consequences derived from involvement of the stroke team. The small numbers also preclude any significant inference of influence on mRS or discharge destination. The numbers referred to the regional centre for thrombectomy were not specifically recorded for this project, but future evaluations of performance will include this metric.
Change itself can be difficult and good communication was a vital constituent of this project. The team endeavoured to involve as many people and disciplines as possible in any changes being made to the pathway. After a thrombolysis case, the stroke registrar spoke to staff involved so any problems could be discussed. Feedback was encouraged at all stages, both formally and informally. These interactions afforded positive visibility of the pathway and staff felt they had ownership of the pathway.
Certainly, there may have been unintended consequences for other patients, such as longer waiting times for either inpatient or outpatient CT if an urgent scan was required for a patient with stroke. Extra resources were required such as training CT radiographers in angiography, and the time to read extra scans. With a potentially higher number of patients being treated, higher numbers of complications may occur.
Most, but not all, of the primary and secondary drivers were fully addressed during the time period, and further work continues on the improvement process, such as regular education and training sessions for doctors and nurses. Recruitment of Advanced Nurse Practitioner posts may disentangle some staff resource restrictions such as only allowing a doctor to prescribe or administer thrombolysis. Regular audit and public display of results will help with pathway visibility and encourage staff engagement.
The acute ischaemic stroke pathway collates in one document advice regarding stroke care, adverse effects, thrombectomy, serving as an efficient care bundle aiding in the understanding and navigation of the steps for comprehensive assessment and treatment no matter the specialty of the admitting doctor.
With respect to extrapolating service improvements to other projects, pivotal learning points include an objective task analysis of the patient journey to expose redundancies or duplications. For example, some activities in figure 1 were discarded, such as referral to medics, transfer and waiting times. Others were operated in parallel or merged, such as referral to stroke team, booking scans and assessments. An improvement in patient flow is evidenced not only by reductions in DTN time but also in the gap between DTCT and DTN.
Encouraging continuous communication via feedback loops for all staff involved helps to achieve buy-in as actions are materially linked to downstream events. Publicising results within an institution and good governance structures allow recognition and replication of accomplishments and swift correction of problems.
In conclusion, this project led to a significant and sustained improvement in acute stroke care in our hospital with the use of quality improvement techniques, a new hospital acute ischaemic stroke protocol and dedicated stroke team. A comprehensive, comprehensible protocol, recurrent and ongoing staff education using novel teaching techniques like simulated training and good communication will help to mitigate delays and further enhance the care provided to patients presenting with stroke. The approach described may be valuable to the improvement of services other than stroke.
Acknowledgments
The project team would like to acknowledge the contribution of all patients and their families, the help and enthusiasm of staff from all departments in the hospital and neuroradiology centres.
Footnotes
Contributors KMcG produced the process map, driver diagram, tested PDSA cycles, worked as the stroke registrar on the team assessing and treating patients, rewrote the integrated pathway, liaised with all relevant staff members, departments and regional specialty centres, set up and chaired governance meetings, presented at educational sessions conducted surveys, results and data entry, wrote and submitted the paper. NC was the stroke CNS on the team assessing and treating patients, oversight of stroke unit ward, results and data entry, helped with PDSA cycles, presented at educational sessions, advice on integrated pathway, attended all governance meetings. DL was a consultant on the stroke rota, advised on improvements, facilitated communication between departments, attended all governance meetings. JMcM was a consultant on the stroke rota, advised on improvements, facilitated communication between departments, attended all governance meetings. MO’C was a consultant on the stroke rota, advised on improvements, facilitated communication between departments, attended all governance meetings. CP was a consultant on the stroke rota, advised on improvements, facilitated communication between departments, attended all governance meetings. EM assessed and treated patients, reviewed and piloted integrated pathway, attended all governance meetings.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.