Article Text

Abstract
The practice of delayed cord clamping (DCC) in premature infants has proven benefit to the neonate. In a community-based perinatal centre, the practice of DCC for more than 60 s for premature infants with gestational age of <35 weeks was identified to occur infrequently at 20% in 2013. The perinatology group in conjunction with nursery, labour and delivery, and obstetric staff sought to improve adherence to the best practice of DCC for premature infants. In an effort to achieve this goal, we developed an evidence-based clinical practice guideline, included key stakeholders in its development and provided timely feedback to delivery providers about DCC performance. The frequency of DCC for this population improved from 19.5% in 2013 to 85% in 2017. The success in improving this best practice is attributed to the involvement of the multidisciplinary team who developed the guideline, and the sustained improvement was encouraged with the continued reaffirmation of DCC goals to delivery providers.
- healthcare quality improvement
- pdsa
- quality Improvement
- clinical practice guidelines
- continuing education, continuing professional development
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- healthcare quality improvement
- pdsa
- quality Improvement
- clinical practice guidelines
- continuing education, continuing professional development
Problem
In a community teaching hospital in Denver, Colorado, with an obstetric delivery service of more than 4500 deliveries per year and a level 3 neonatal intensive care unit (NICU) with approximately 500 admissions per year, we wanted to standardise the best practice of delaying the clamping of the umbilical cord for at least 60 s in infants with a gestational age (GA) at birth of less than 35 weeks’ gestation after a delayed cord clamping (DCC) frequency of 20% at our hospital was identified in 2013.
Background
The practice of immediate cord clamping (ICC) overlooks the possibility of benefit to the neonate that occurs during delayed umbilical cord clamping. The WHO has recommended DCC for all infants after birth in low-income and middle-income countries.1 There is cumulative evidence about the benefits for all infants of delaying the clamping of the umbilical cord for 30–60 s after birth. For term infants, this offers higher iron stores and decreases iron deficiency anaemia, a major issue in low-income and middle-income countries.1 In 2017, the Committee on Obstetric Practice of the American College of Obstetricians and Gynecologists (ACOG)2 reaffirmed its support of the practice of DCC for preterm infants, when feasible. The American Academy of Pediatrics endorsed that recommendation.3
The preterm infant has further benefits from DCC. By improving the intravascular volume of the premature, blood pressure is stabilised, preventing the use of inotropic agents,4 and increases their haematocrit,5 decreases the chances of needing a blood transfusion,4 increases superior vena cava flow,6 and decreases the chances of developing all forms of intracranial bleed and necrotising enterocolitis.7 A recent systematic review,8 in which a recent large randomised clinical trial was included,9 concluded that DCC in premature infants reduces hospital mortality by 32%.
DCC does not appear to interfere with delivery room resuscitation. An observational study of preterm infants that were treated with DCC demonstrated that they required less delivery room resuscitation than those with ICC.10 The benefits of DCC in all term infants in industrialised countries, however, need to be weighed against the possibility of more infants developing significant jaundice and needing phototherapy.11
Contraindications to DCC include severe blood group incompatibility manifested as fetal hypervolaemia (hydrops fetalis), maternal HIV-positive status with high viral load, and suspected fetal polycythemia or hypervolaemia, intrauterine growth restriction (IUGR) due to maternal smoking, recipient of twin-to-twin transfusion, or known Down’s syndrome.
Setting
Saint Joseph Hospital (SJH) is a not-for-profit organisation located in the metropolitan area of Denver, Colorado. It is a general hospital with the largest number of deliveries in the state. Babies are delivered by a large group of practising obstetricians, obstetrics-gynaecology (Ob-Gyn) residents in training and midwives. Unique to our system is that one or more members of the neonatal team—neonatal nurse practitioners (10 NNPs) and neonatologists (8)—attend the deliveries of all preterm infants. Neonatologists attend only those of less than 28 weeks’ gestation.
Baseline measurement
DCC up to 30 s was implemented in our institution in 2002 for premature infants born below or at 32 weeks’ gestation. This practice was not implemented as a formal quality improvement (QI) initiative but rather as a best practice, presented by AFP as a clinical practice guideline (CPG) that was disseminated to obstetricians, neonatologists and nurse practitioners. The practice was documented in an electronic database (Neodata) that has been used in our NICU since 2001. There was poor compliance with the practice, and the reason for not delaying the clamping of the cord was not documented. DCC was not practised for infants with GA between 32 and 35 weeks’ gestation.
We used the frequency of DCC for very low birth weight (VLBW) during 2013 as a baseline measurement. We chose that period of time since there was not a proactive discussion or review of the literature about the benefits of DCC during that year.
Aim
The aim is to increase the frequency of DCC for at least 60 s for all eligible premature infants with GA of less than 35 weeks’ gestation from 19.5% to 80% by the end of 2016. A driver diagram was created to guide our QI initiative (see figure 1).
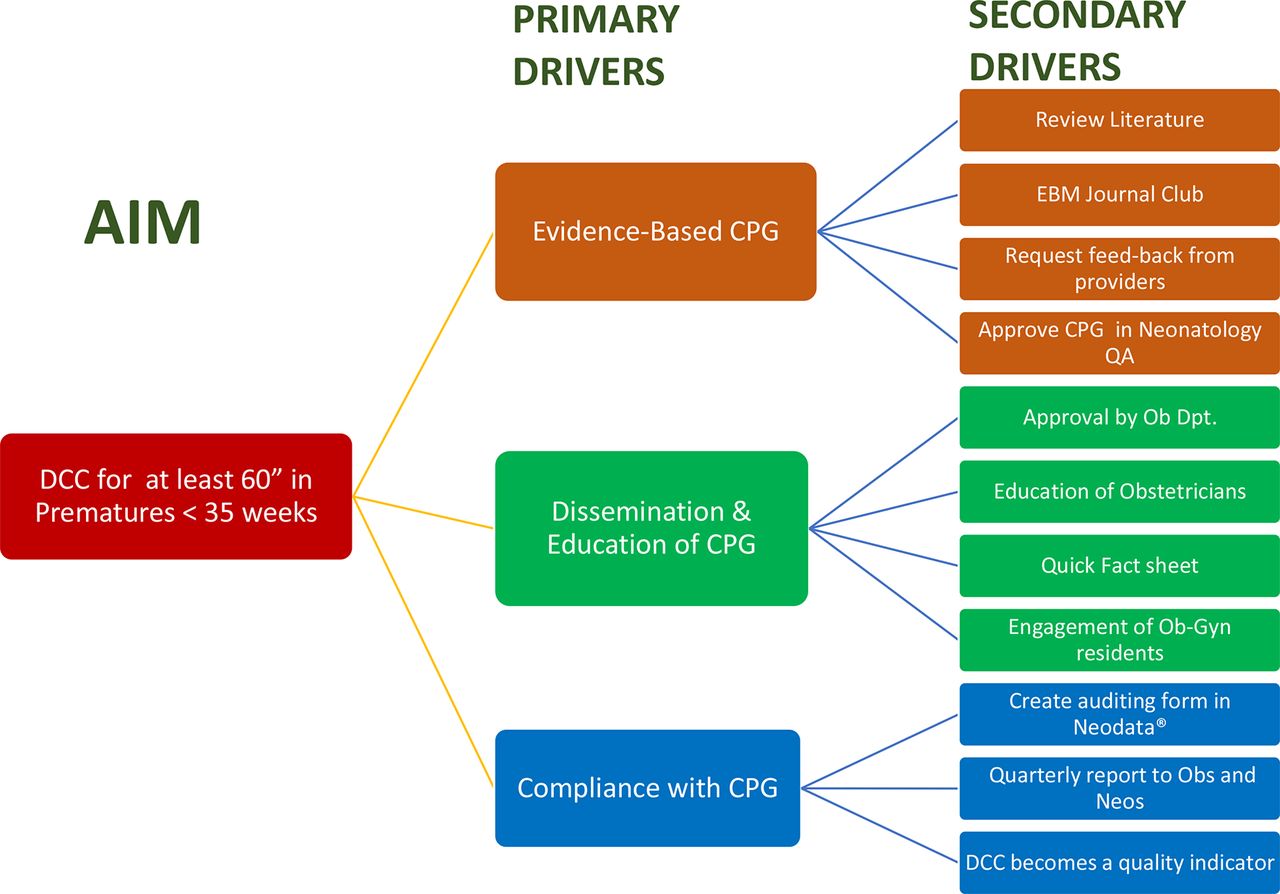
Driver diagram. The secondary drivers were implemented as four PDSA cycles to support our three primary drivers: create an evidence-based CPG (brown), educate providers about the guideline (green), and check and encourage compliance with the guideline (blue). CPG, clinical practice guideline; DCC, delayed cord clamping; EBM, evidence-based medicine; PDSA, plan, do, study, act.
Tests of change
The Model for Improvement12 was used as the framework to guide our QI work for this new practice. Several PDSA (plan, do, study, act) cycles were carried out. The process of implementation of a new practice in our NICU has been standardised and in 2011 was described in a peer-reviewed publication.13
PDSA 1: create a CPG
Plan
In December 2013, a neonatologist (AFP) asked the SJH librarian to do an extensive review of the literature using the PICO approach about clinical trials performed in premature newborns (P) comparing DCC (I) with early cord clamping (ECC) (C) and their outcomes (O). Pertinent articles were selected by another neonatologist (MD) and then assigned for review to the neonatologists and NNPs of our NICU. Articles were discussed in the January 2014 Evidence-Based Journal Club.
Do
Based on the conclusions of the journal club, AFP created a CPG that was presented to other members of the department for review and suggestions using the department electronic weekly newsletter ‘Wednesday News’ in February 2014.
Study
The guideline with all the suggested modifications was approved by the Neonatology Quality Assurance Committee in March 2014. This multidisciplinary approach to create and implement CPG has been in practice in our department since 2002.13
Act
Details of the procedural guidelines included a step-by-step fashion of how to perform DCC for at least 60 s.
PDSA 2: dissemination and education of CPG
Plan
The goal of this PDSA was to inform all members of the delivery team about the potential benefits of DCC and the details of the procedure.
Do
A communication-based strategy was implemented to disseminate the guideline to all providers, to identify champions in other departments and to address possible barriers to DCC implementation. AFP delivered a presentation about the DCC to NNPs, neonatologists, NICU nurses, Ob-Gyn physicians and residents during department meetings, and to other groups of practising obstetricians, midwives, nurse educators and residents in obstetrics.
Study
Information obtained during the presentations allowed us to identify important champions: We identified that the practice of DCC was going to be largely implemented by prompting of the obstetrical team by the NNPs or neonatologists attending the deliveries. We also identified that the ‘buy-in’ of the Ob-Gyn residents was necessary since they were consistently present in most deliveries. A first-year resident in Ob-Gyn (JC) volunteered to be the champion for his peers.
Act
A laminated, one-page summary of the guideline was attached to the computer monitors of the nurses and physicians of the labour and delivery area of the hospital. Rates of DCC were obtained quarterly from a computerised system adjunct to the medical record (Neodata). A field was created in that medium to record the performance of DCC, lack of performance and reasons for the latter, together with other information that might contraindicate DCC. Neodata queries yield databases amenable to analysis in Excel. The DCC guideline was made readily accessible to all providers by placing it in the protocol section of the Neodata. After the initial presentation to the residents in obstetrics, JC became part of the QI team. His role was to educate his peers about the benefits of DCC and also to give periodic feedback to other residents and faculty about the DCC performance. He also became the presenter of the DCC guideline to the new residents during the June introductory lectures in 2015, 2016 and 2017.
PDSA 3: DCC, a quality indicator
Plan
At the end of 2014 the leadership of Colorado Permanente Medical Group (CPMG) requested the neonatologists to select one or more quality indicators as a measure of productivity of our department. The neonatologists decided to incorporate DCC as one of those indicators for our department in 2015.
Do
Starting in 2015, a neonatologist (JB) provided quarterly updates about DCC to the neonatologists and to the CPMG leadership.
Study
Strategies to improve compliance with the guideline were discussed in the monthly department meetings.
Act
By the end of 2015, the successful implementation of the guideline was communicated to the CPMG leadership. Our department received recognition for the successful implementation of this practice.
PDSA 4: checking for CPG compliance
Plan
In July 2015, we tried to identify the reasons for the lack of compliance with DCC guideline.
Do
After each delivery, the NNP or neonatologist entered performance (or lack thereof and reasons for lack) into the Neodata. The neonatologist reviewed each delivery and discussed DCC performance with the NNP, especially when and why if not performed.
Study
Neodata was queried quarterly to assess compliance with the practice change and reasons for non-compliance. We identified that the most frequent reasons for not performing DCC were ‘Infant too sick’ and ‘Forgot to do it’.
Act
Actions were taken to improve compliance. AFP shared graphic displays of the performance and frequencies of the reasons for not compliance with different groups of providers via email and the ‘Weekly News’. The obstetric resident involved in the QI project (JC) used the same graphs during the monthly educational meetings and encouraged their peers to continue this best practice.
Results
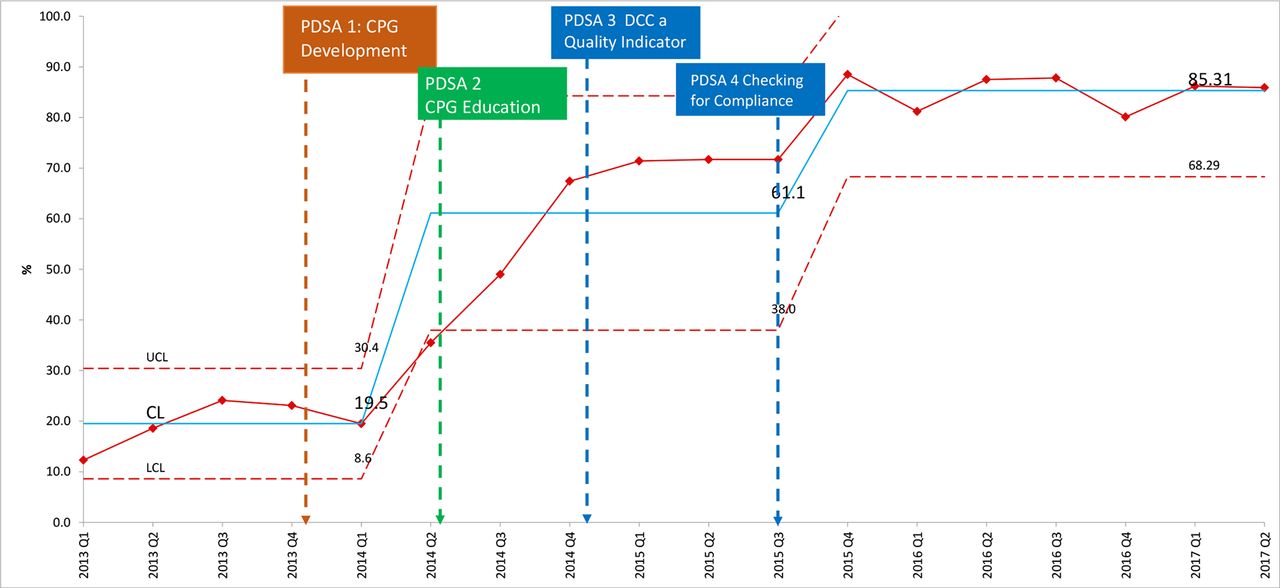
Between 1 January 2013 and 30 June 2017, 1050 premature infants with GA of less than 35 weeks’ gestation were born at SJH and then admitted to the NICU of the same hospital. The statistical process control chart (figure 2) shows the quarterly performance for DCC during those 4.5 years.
{kind=link}
{kind=link}
Delayed cord clamping performance and PDSAs. The frequency of delayed cord clamping for at least 60 s (blue line) is shown by quarterly performance in this control chart. It increased from 19.5% in 2013 (baseline observation) to 85% after the third quarter of 2015. The initiation of the implementation of the four PDSA cycles is demonstrated by the respective coloured arrows. CL, control limit; CPG, clinical practice guideline; DCC, delayed cord clamping; LCL, lower control limit; UCL, upper control limit; PDSA, plan, do, study, act.
A significant increase in the DCC rates of premature neonates <35 weeks GA was observed from 19.5% in 2013 to 85% in 2017.
Lessons and limitations
The strengths of this intervention included the formulation of a guideline using a multidisciplinary approach that has worked in our NICU for a few years,13 the capacity to monitor quarterly performance using a database and the ability to provide prompt feedback to delivery providers regarding DCC compliance. The practice of DCC was largely implemented by prompting of the obstetrical team by the NNPs and or the neonatologist present in the delivery room. NNPs were clearly the most important ‘drivers’ for DCC since they attend to most of the preterm deliveries. The ‘prompting’ about DCC has evolved recently to be a part of the ‘brief’ discussion of the perinatal team prior to the delivery of a preterm infant.
Obstetricians and midwives may have been motivated to be compliant with DCC by ACOG statements2 and by the recommendation of DCC in the Neonatal Resuscitation Program (NRP).14 It is very important to state that all nurses in the labour and delivery area, as well as new OB residents, are required to take the NRP certification exam soon after they start working in our hospital.
The limitations include the necessity of periodic reintroduction of the guideline; the obstetric practice of active management of the placenta is often performed reflexively based on traditional training; and new resident staff requiring training in best practices. This last hurdle of training new staff is a difficult one as it occurs annually with the matriculation of new residents. These physicians in training are required to learn many new practices regarding patient care, only one of which is DCC in the preterm infant. This issue is currently addressed by yearly reintroduction of the DCC guideline at resident didactics and by the continuation of NRP certification during their first month of training.
The DCC performance improved with the intervention and it surpassed the expected 80% for those prematures that did not have a medical condition where DCC was contraindicated. The number of cases when there was an opposition of the obstetrician to perform DCC was minimal during the period of this intervention. The DCC performance appears to have stabilised after the fourth quarter of 2015.
Conclusion
In a perinatal centre located in a community hospital in Denver, the implementation of DCC for premature infants with GA <35 weeks was very successful, increasing from 19.5% in 2013 to 85% in 2017. This successful implementation of an evidence-based guideline was achieved, thanks to a progressive engagement, feedback and education of key stakeholders. In our case we believe that the NNPs and the Ob-Gyn residents were the most important group of providers that contributed to this project’s success. This improvement could be replicated in other institutions by identifying champions, monitoring DCC rates, periodically reminding providers on this best practice and identifying possible institution-specific barriers. Our team hopes to sustain adherence with periodic reminders of this best practice as necessary until the practice is standardised. The next steps for this implementation would include prompt identification and response to providers who are unable to offer an indication for not performing DCC during deliveries where DCC did not occur. This direct method may help reduce the occurrence of reflexive active management of the placenta and allow for an opportunity to perform DCC.
Acknowledgments
The authors would like to acknowledge the neonatal nurse practitioners at Saint Joseph Hospital in Denver (Lynn Miller, Theresa Nowadzky, Jeanne Burks, Britt Carlson, Amanda Duran, Terry Mendoza, Sheila Wheeler, Manoj Sebastian, Carey Lemmons and Kathryn Brecht), as well as the Ob-Gyn residents and obstetricians.
Footnotes
Contributors AFP: author of the guideline, and educated the neonatologists, NNPs, obstetricians and midwives about the guideline. He also created the graphic displays of DCC performance and shared this information with neonatology and OB providers. He wrote both versions of the manuscript. AR: reviewer of the literature for the creation of the DCC guideline, and as NICU Medical Director promoted the inclusion of rate of DCC in premature infants as a quality indicator. MF: reviewer of the literature for the creation of the DCC guideline and contributed to the development of the DCC guideline. MD: organised and conducted the Evidence-Based Journal Club. He selected the literature that was reviewed for the development of the DCC guideline. JB: reviewer of the literature for the creation of the DCC guideline. He created the queries in Neodata that were used to assess DCC compliance. He also updated CPMG about the progressive improvement of this quality measurement. He reviewed and contributed to the generation of the second draft of this manuscript. EL: reviewer of the literature for the creation of the DCC guideline. MC: reviewer of the literature for the creation of the DCC guideline. JC: resident champion. He provided education to the Ob-Gyn residents about the DCC guideline and offered them feedback about the performance of this QI initiative. He also contributed to the writing of the first manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval This quality improvement (QI) project was presented to the Institutional Review Board of Saint Joseph Hospital for their consideration. The IRB qualified the project as a QI project.
Provenance and peer review Not commissioned; externally peer reviewed.