Article Text

Abstract
Aims The Scottish Inpatient Diabetes Foot Audit conducted in 2013 revealed that 57% of inpatients had not had their feet checked on admission, 60% of those at risk did not have pressure relief in place and 2.4% developed a new foot lesion. In response, the Scottish Diabetes Foot Action Group launched the ‘CPR for Feet’ campaign. The aim of this project was to raise awareness of the ‘Check, Protect and Refer’ (CPR) campaign as well as improve the assessment and management of inpatients with diabetes.
Methods A quality improvement project underpinned by Plan-Do-Study-Act (PDSA) methodology was undertaken. The first and second cycles focused on staff education and the implementation of a ‘CPR for Feet’ assessment checklist using campaign guidelines, training manuals and modules. The third and fourth cycles focused on staff feedback and the implementation of a ‘CPR for Feet’ care bundle.
Results Baseline measurements revealed 28% of patients had evidence of foot assessment. Medical and nursing staff reported to be largely unaware of the ‘CPR for Feet’ campaign (13%). Fifty-two per cent of inpatients with diabetes had their feet assessed and managed correctly following the second PDSA cycle. After completion of the third and fourth PDSA this number improved further to 72% and all staff reported to be aware of the campaign.
Conclusions The introduction of a ‘CPR for Feet’ care bundle improved the assessment of inpatients with diabetes.
- diabetes complications
- foot disease in diabetes
- checklist
- care bundle
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Foot disease is a life-changing complication for the patient with diabetes and is associated with increased morbidity and mortality. It accounts for more hospital bed-days than all other complications of diabetes and its prevalence is steadily rising in the UK.1 A total of 130 patients undergo limb amputation per week as a result of diabetes. In Scotland alone, there are 490 amputations a year.2
According to the Scottish Inpatient Diabetes Foot Audit 2013, 2.4% of inpatients develop new foot lesions while in hospital, with 57% of patients not receiving any foot assessment during their inpatient stay.3 In order to reduce the associated morbidity, diabetes-related foot complications should be considered during inpatient stays with prompt and effective prevention and management.3
A quality improvement project was undertaken at Glasgow Royal Infirmary to improve the assessment of inpatient diabetes foot complications through improving awareness of the ‘Check, Protect and Refer’ (CPR) approach to foot assessment. To achieve this we designed and implemented a simple checklist based on new guidelines as set out by the National Health Service (NHS) Scotland.3 This checklist encouraged foot assessment and appropriate referral of inpatients with diabetes who were receiving their care on three specific medical wards. ‘CPR for Feet’ checklists were made available to all three wards and assessments were carried out by nursing and medical staff following educational sessions. Four separate Plan-Do-Study-Act (PDSA) cycles were conducted and, after cycles 1 and 2, the checklist evolved into a final care bundle which was tested in cycles 3 and 4.
Problem
The increasing prevalence of diabetes represents a serious health concern globally; with a growing clinical focus on the education, prevention and management of this multisystem disease.
The National Institute for Health and Care Excellence (NICE) estimates that more than 5 million people will have been diagnosed with diabetes by 2025 in the UK alone, making it one of the most common chronic diseases faced by our healthcare service.4 The frequency of patients developing complications is even more alarming, with peripheral vascular disease affecting one in every three patients over the age of 50.4 Life expectancy can decrease by 15 years secondary to the development of complications.4
Foot ulceration is defined as ‘a localised injury to the skin and/or underlying tissue, below the ankle’. In a person with diabetes, ulceration is associated with peripheral arterial disease and peripheral neuropathy, often in combination.5 Patients presenting with long-standing, undiagnosed foot ulceration are at higher risk of amputation than those diagnosed at an earlier stage.5 It is estimated that at least 10% of patients with diabetes will suffer a foot lesion during their lives.5 Foot complications arising in a patient with diabetes have a significant financial burden on the NHS with increased bed occupancy and prolonged inpatient stays. NHS Diabetes published a report in 2012 which estimated that approximately £650 million is set aside for the treatment of foot ulcers or amputations each year in the UK.5
More than 80% of amputations in people with diabetes are a result of foot ulcers.4 According to NICE, both type 1 and type 2 diabetes mellitus are the most common cause of non-traumatic limb amputation. Five years on from the onset of a foot ulcer developing, a patient’s mortality rate may rise to 50%, with up to 70% patients dying within 5 years of having had an amputation.4 Therefore, the need for increased foot screening in hospitalised patients has become a priority for the Scottish Government, as set out in the Diabetes Action Plan 2010.2
Unfortunately, despite the availability of guidance, there is still a wide variation in practice across NHS settings.2 This is evident when looking at the various foot care screening programmes that have been implemented across the UK. Factors influencing this variability include individual trust policies and the availability of healthcare professionals with expertise relevant to the management of foot complications in diabetes.5
Background
The aim of the St Vincent Declaration6 was to reduce the burden and complications of diabetes in European member states. In particular reduce the numbers of limb amputations in diabetes for gangrene by 50% in a 5-year period.6
Twenty-five years later, in 2014, the Scottish Diabetes Survey reported that 4.9% of the patients with diabetes currently have foot ulceration.7 The Scottish Inpatient Diabetes Survey undertaken in November 2013 reported that 2.4% of these patients develop a new foot ulcer during their stay in hospital.7 These figures are predicted to inevitably increase with the trends in current population particularly given the rising number of people being diagnosed across the UK with diabetes.8 It still remains clear that without ongoing prevention strategies, the cost of diabetes and its complications will pose a significant challenge to the NHS of the future.
More recently, the NICE guidelines issued in January 2016 set out best practice recommendations for prevention and management of foot problems for inpatients with diabetes.4 This includes:
Each hospital having a care pathway for people with diabetic foot problems who need inpatient care.
A named consultant should be accountable for the overall care of the person, and for ensuring that healthcare professionals provide timely care.
Refer the person to the multidisciplinary foot care service within 24 hours of the initial examination of the person’s feet. Transfer the responsibility of care to a consultant member of the multidisciplinary foot care service if a foot problem is the dominant clinical factor for inpatient care.
The named consultant and the healthcare professionals from the existing team should remain accountable for the care of the person unless their care is transferred to the multidisciplinary foot care service.
The Scottish Diabetes Foot Action Group (SDFAG) launched the ‘CPR for Feet’ campaign following the results of the 2013 Scottish Diabetes Inpatient Foot Audit. It was introduced throughout Scotland in April 2015 with the main objective aiming to eradicate foot lesions in inpatients with diabetes.
Funding made available by the SDFAG ensured a ‘CPR for Feet’ poster was available on every Scottish hospital ward.3
Baseline measurement
The aim of this project was to improve the proportion of inpatients with diabetes receiving a foot assessment by raising awareness of the ‘CPR for Feet’ campaign across general medical wards with a specialist interest in diabetes at a large Glasgow teaching hospital. It set out to improve the consideration of foot disease in inpatients with diabetes by both medical and nursing staff.
We aimed to achieve this by identifying and developing a simple tool to aid staff in their approach to diabetes foot assessment and ultimately improve the diagnosis and management of diabetes foot complications.
The aim was to have this project carried out over a 6-month period within these wards and conduct PDSA cycles to identify a potential intervention that could be introduced to improve foot assessment. Longer term, we hoped that this intervention could be implemented across all hospital wards at Glasgow Royal Infirmary.
A snapshot of current practice across the three wards was conducted with all 25 concurrent patients with known type 1 or type 2 diabetes identified. We recruited these patients consecutively by identifying those who meet inclusion criteria on consecutive admission to the wards. The medical notes for the current admission were reviewed and specifically assessed for any documented evidence of foot assessment. The only inclusion criterion was that these patients had known and documented type 1 or type 2 diabetes at time of presentation to hospital. We found that 28% of these patients had documented evidence of foot assessment, usually carried out during acute admission period. However, the timing of these assessments was not consistent and no formal identification tools were used to aid assessment.
In addition to the above snapshot, members of both medical and nursing staff were interviewed on their awareness of the ’CPR for Feet’ campaign. Staff members were asked verbally for a yes or no response if they were aware of the current campaign and these responses collected. Two of the 15 questioned (13%) were aware of the initiative while the remaining 87% denied knowledge of the campaign. Medical staff questioned ranged from foundation to consultant level with nursing staff ranging from newly qualified to senior charge nurses.
This was taken as our baseline measurements to inform PDSA cycles. The outcome of this initial measurement confirmed that not all patients with diabetes were having foot assessment during their inpatient stay. There was found to be a clear lack of awareness on the ‘CPR for Feet’ campaign among medical and nursing staff.
Design and strategy
Our project consisted of four PDSA cycles as detailed below and represented in the flow diagram (figure 1). Although the original project was based on a checklist, following feedback from staff, we realised implementing a care bundle would potentially yield greater results in terms of identifying patients with diabetic foot complications, while also aiding staff in their decision-making.
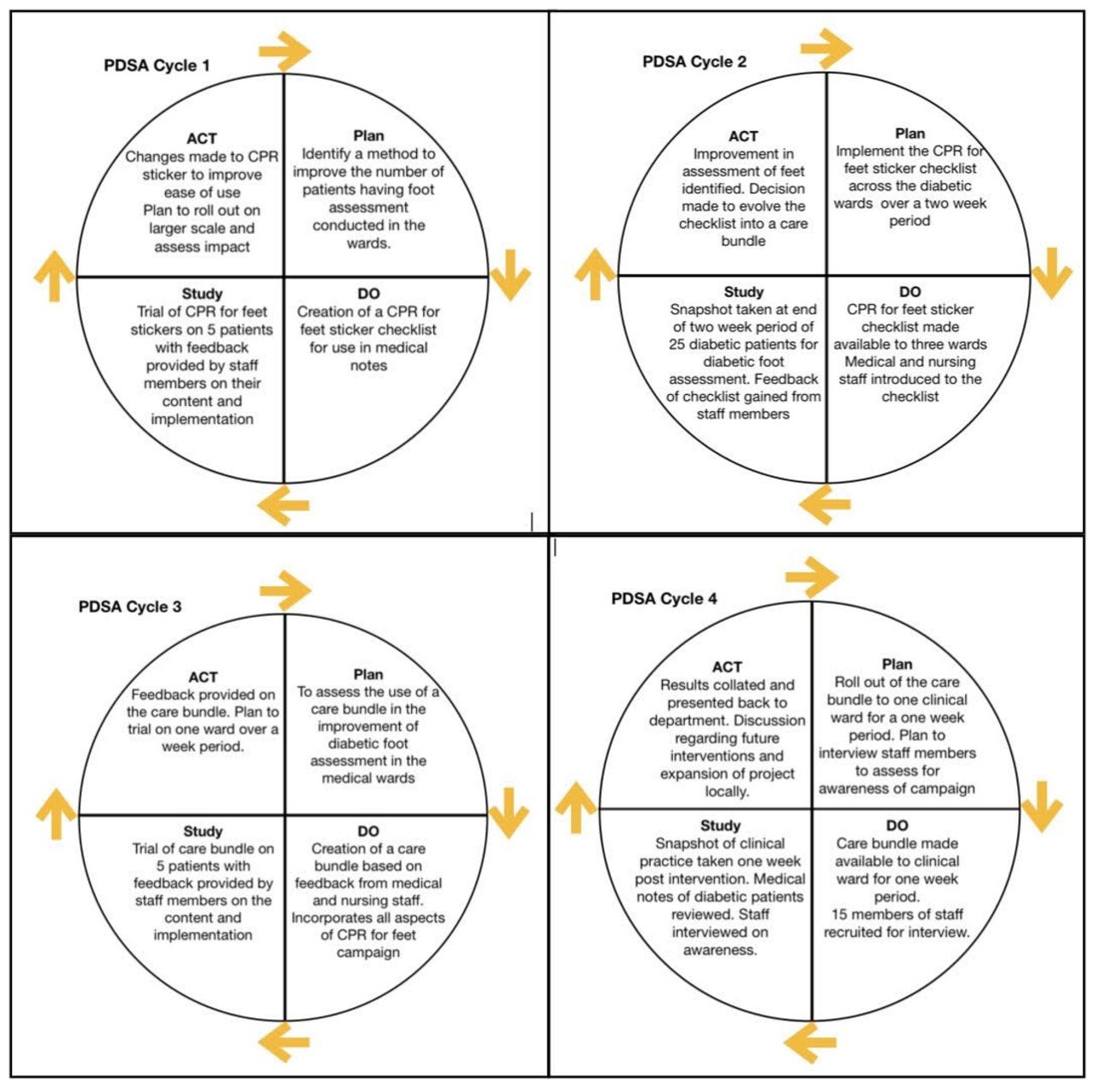
Plan-Do-Study-Act (PDSA) cycles in flow diagram format. Four cycles were conducted on the PDSA method of quality improvement. Each cycle represented separately in the diagram with the main features of each intervention detailed.
We felt this was a realistic quality improvement project to be performed in a busy inpatient setting.
Staff had access to a LearnPro module highlighting awareness of the campaign. Staff were interviewed and specifically asked if they were aware of the current ‘CPR for Feet’ campaign. Fifteen members of staff were asked at the end of cycle 4.
Bias was eliminated as much as possible as both authors did not take part in implementing the newly designed intervention on these wards. We also selected patients who met inclusion criteria based on consecutive patient admissions to the ward to avoid selection bias.
Each PDSA cycle was run for 2 weeks and usually began at the start of each month. Our project ran for 6 months in total from baseline measurement to dissemination of the results.
PDSA cycle 1
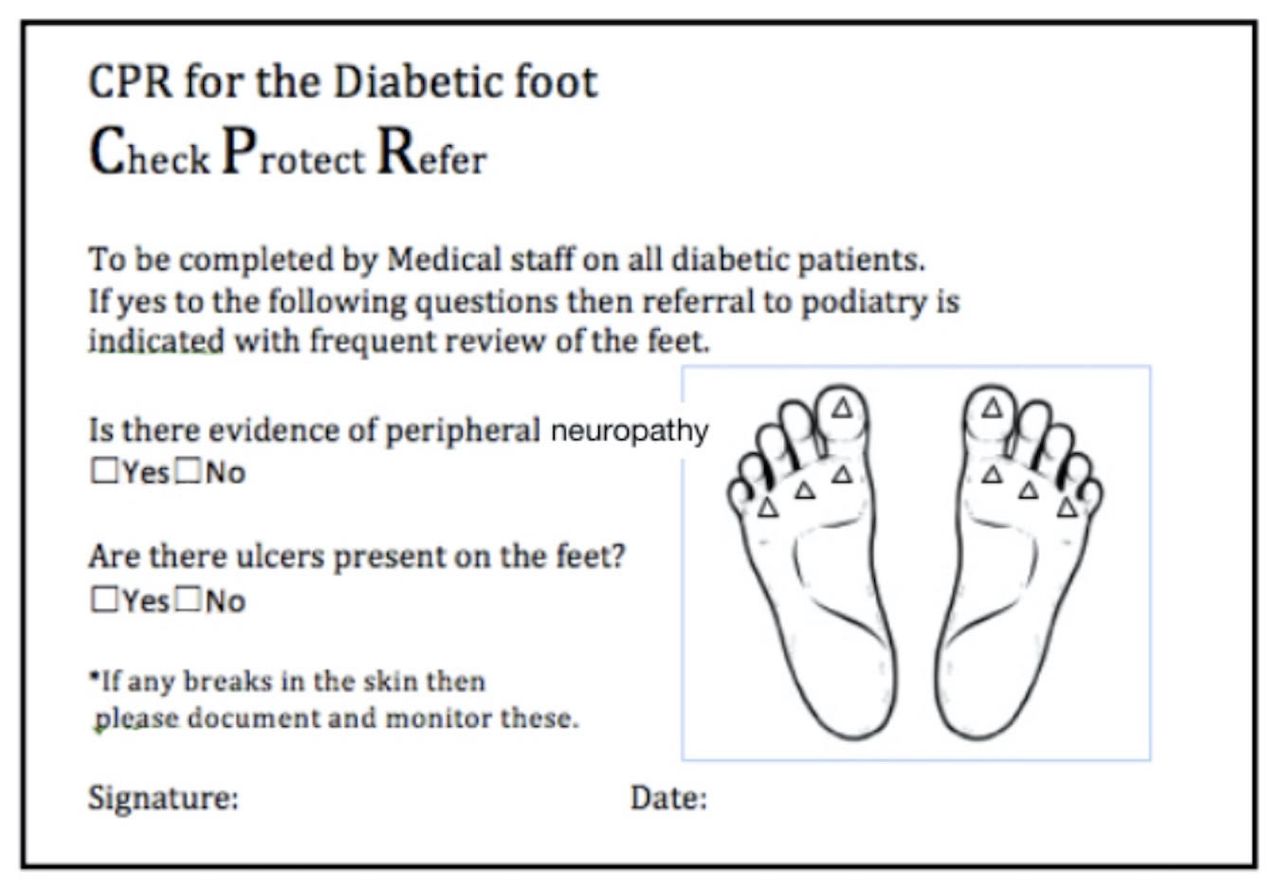
The initial cycle began with the creation of a sticker checklist (figure 2) which could be placed into written medical notes. These were placed in all patient note trolleys and easily accessible to medical and nursing ward staff. This sticker checklist was designed to mirror the ‘CPR for Feet’ posters which were visible on all wards. This addition to the notes aimed to encourage identification and assessment of diabetic foot complications. The questions on the sticker checklist asked: Has the patient previously had ulcers documented? Are there ulcers present? Is there evidence of peripheral neuropathy? The first cycle trialled these new checklists on five patients and feedback was obtained. The cycle also involved raising awareness of the problem to key members of ward staff, including giving education sessions based on the ‘CPR for Feet’ campaign and the emphasising the importance of recognising and treating the complications of diabetic foot ulcers.
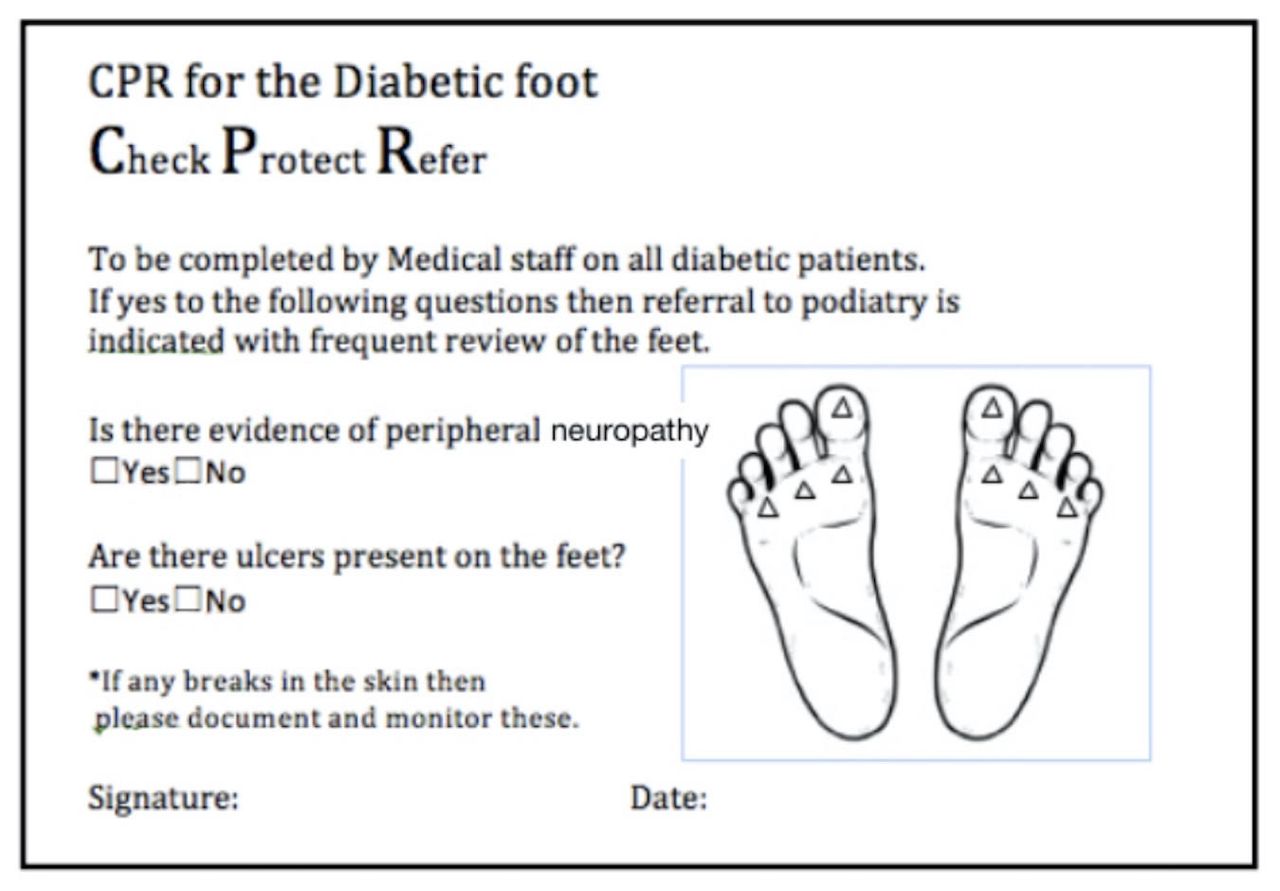
‘CPR for Feet’ sticker checklist. Used in Plan-Do-Study-Act (PDSA) cycles 1 and 2 with aim to improve frequency of assessment for diabetic foot complications. Adhesive sticker made available to clinical staff and to be placed into medical notes on ward assessment.
PDSA cycle 2
Feedback obtained during the initial cycle allowed for improvements to be made to the ‘CPR for Feet’ stickers. Changes were made to both the size and format of stickers. This meant they were easier to complete and insert into patient’s notes by both medical and nursing staff. It was important to ensure the intervention was user friendly and could easily be adopted into current clinical practice. At the end of a 2-week period of the stickers being available to staff we conducted a snapshot of current practice on 25 patients with diabetes across the three wards on consecutive admissions and reviewed their case notes. We identified if patients had received a foot assessment and if this was completed using the newly introduced sticker.
PDSA cycle 3
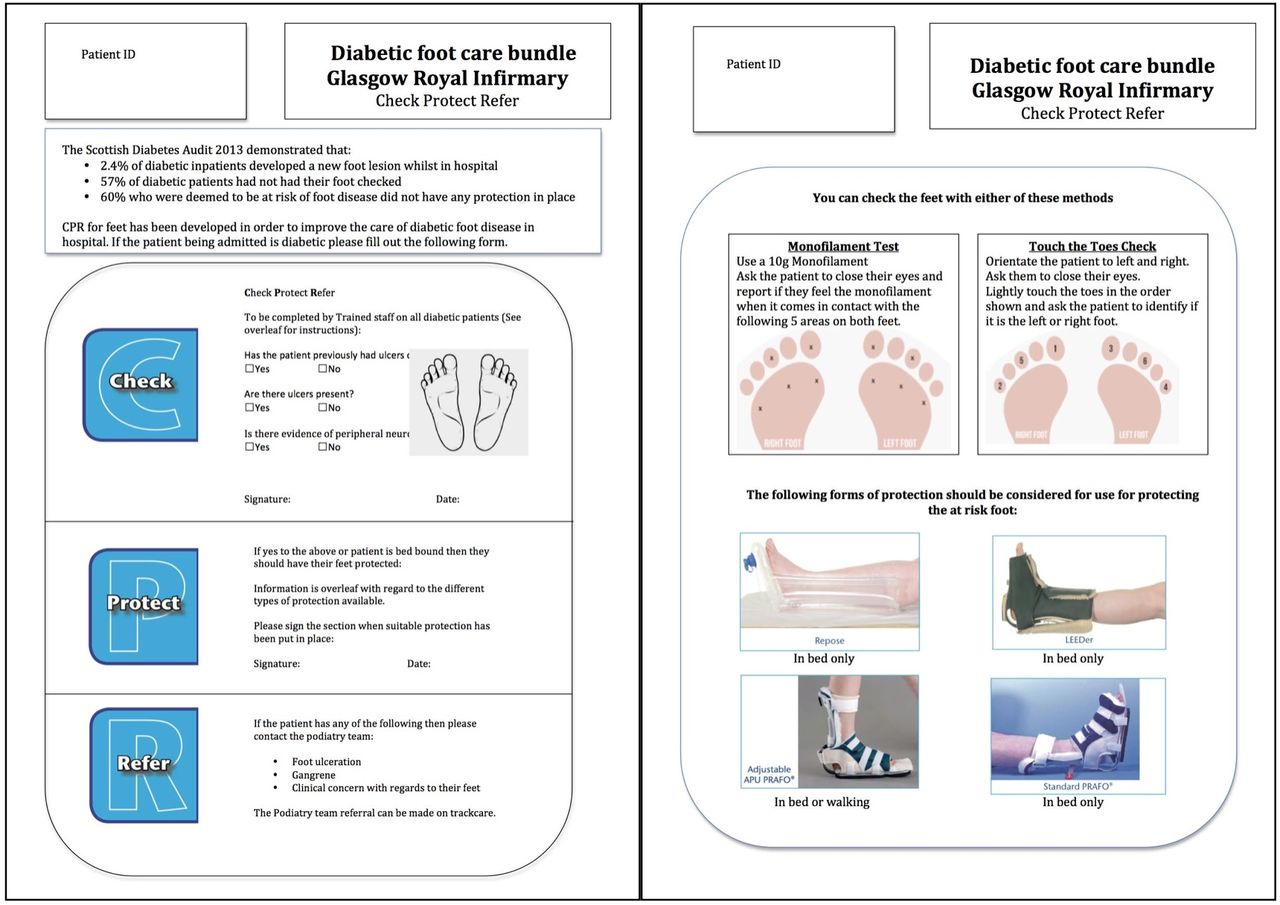
Prior to cycle 3 and following feedback from clinical staff, a care bundle was developed which was to be placed in the patients’ ward admission notes (figure 3). It incorporated all aspects of the ‘Check, Protect and Refer’ ethos of the campaign. Important key members of staff indicated they felt they lacked training in assessment of foot neuropathy and subsequently were not confident in undertaking foot assessment. Aiming to address these concerns, two options for the assessment of peripheral neuropathy were detailed with diagrams explaining the process. Other issues which had arose included lack of knowledge regarding subsequent steps in the management process, and difficulties in remembering to actively insert the stickers into the medical notes when a patient with diabetes was identified. The new bundle addressed both of these issues and it became a core component of a patient with diabetes admission, with information available on the local referral process for staff to consult. This care bundle was initially trialled on five patients with feedback obtained.
{kind=link}
{kind=link}
{kind=link}
Diabetic foot care bundle. Used in Plan-Do-Study-Act (PDSA) cycles 3 and 4. Double-sided A4 document made available to clinical staff. Incorporating all aspects of the ‘CPR for Feet’ campaign. Includes advice on protection and referral process. Provides staff information on assessing for peripheral neuropathy via two methods.
PDSA cycle 4
The final cycle was conducted on one ward in order to focus the implementation of the care bundle to one clinical unit. The ward was provided with the care bundle and added them to hospital ward admission packs. At the end of a 1-week period the medical notes of the patients on the ward were reviewed in a snapshot of clinical practice. Eleven of the patients in the ward had a documented history of diabetes and were therefore eligible for medical note review to assess whether a foot assessment had taken place and if the care bundle had been completed.
Results
Our aim was to improve the proportion of patients with diabetes who received a foot assessment by raising the awareness of the ‘CPR for Feet’ campaign. This was achieved by the development of a care bundle in partnership with ward staff.
Cycle 2 assessed the impact of the ‘CPR for Feet’ sticker on patient care. At the end of the 2-week period a snapshot of clinical practice was conducted. Of 25 patients, 13 (52%) had assessment of feet conducted—all of these had been done using the ‘CPR for Feet’ assessment sticker which had been completed by both medical and nursing staff.
The final care bundle was implemented in PDSA cycles 3 and 4 as a response to clinical staff feedback and attempted to further improve ease of use while bringing together elements from all aspects of the ’CPR for Feet' campaign. It also had an initial five-patient trial with feedback directing cycle 4.
Cycle 4 was conducted on one ward and the care bundle was available for a 1-week period to the inpatient team.
At the end of this period a further snapshot of clinical practice was conducted. Eleven patients with diabetes were identified as current ward admissions. Of these 11 patients, eight (72%) were found to have received a foot assessment using the ‘CPR for Feet’ care bundle.
Staff feedback was positive to the intervention and no significant issues were reported with this new format. Fifteen staff from across the clinical unit were questioned at the end of cycle 4 with regard to the ’CPR for Feet’ campaign and all 15 reported awareness of the campaign (100%). This was a significant result given 87% of staff interviewed at the start of the project had been unaware of the ‘CPR for Feet’ campaign.
Our results demonstrate that we have increased the proportion of assessment and awareness of the ‘CPR for Feet’ campaign. We have achieved this through multiple PDSA cycles and the development of a care bundle in partnership with ward staff. Our intervention was a simple tool yet one which we felt to be realistic and easy to implement in a busy inpatient ward setting.
Lessons and limitations
Prior to intervention only 28% of patients had documented foot assessment during their inpatient stay, with medical and nursing staff reporting they were largely unaware of the ‘CPR for Feet’ campaign. Following the issue of the sticker checklist, there was a notable improvement with 52% of patients with diabetes having their feet assessed by completion of the second PDSA cycle. With staff feedback, education and development of a care bundle this increased to 72% of inpatients with diabetes receiving assessment of their feet by the end of cycle 4. Both medical and nursing staff were familiar with ‘CPR for Feet’ campaign and aware of its role in inpatient diabetes care.
The ‘CPR for Feet’ care bundle was a small and simple intervention that did produce positive change to patient care within our hospital. The project followed the PDSA methodology which allowed for the creation of a care bundle that had not been envisioned when the project was initially conducted. Obtaining staff feedback was key to this implementation which inadvertently increased interest in and attitude towards the project with key staff members.
The project does involve a small cohort of patients and future projects will want to increase the number of patients involved and extend this bundle to a wider range of clinical specialities not only exclusive to general medicine. On a local level, it was positive to see the number of diabetes foot assessments undertaken increased from 28% to 72% after intervention. It is hopeful this could be replicated on a larger scale in future. We aimed to ensure the ongoing use of the bundle by involving a range of medical and nursing staff. Medical staff conducting direct patient care in the ward setting will often rotate specialties and hospitals and therefore new staff may not appreciate the importance of continuing this intervention. Involving nursing staff in the direct creation of the care bundle encouraged confidence in completing diabetic foot assessment and will hopefully allow them to encourage new medical staff to engage with this aspect of diabetic assessment.
In future we would also aim to provide education in a more formal setting, such as junior doctor teaching sessions or at hospital grand round. The project would also benefit from ongoing quality improvement activity to measure the sustainability of the results. We aim to continue this at Glasgow Royal Infirmary by future rotations of doctors. Finally, it is important to consider that this is a small but important intervention in the management of diabetic foot complications. Our project focused specifically on the check aspect of the ‘CPR for Feet’ campaign.
Future work in this area should focus on referral to the foot team while also considering the impact on patient outcomes over time. Indeed, recent work in the USA has provided guidance for the management of diabetes foot complications as well as recommending steps to implementation of successful programme for limb preservation.9 10 Core components of this include establishing a pathway for urgent referrals, readmission alerts for known ‘at risk’ patients and careful discharge planning of those identified as having diabetic foot complications.
Conclusion
This project demonstrates that the introduction of the ‘CPR for Feet’ care bundle can improve the foot assessment in inpatient diabetes. The care bundle ultimately aims to improve patient outcomes and we see this as a first step in improving the care provided to the large cohort of patients with diabetes encountered on general medical wards and beyond. It demonstrates how a simple intervention can be implemented into a clinical unit by junior members of staff and subsequently create change that will benefit patients. We hope it will guide other junior doctors to take the first step into quality improvement.
Acknowledgments
The authors acknowledge all the staff of wards 3, 4 and 5 at Glasgow Royal Infirmary for their engagement with this project. They also thank the Glasgow, North-East Quadrant Podiatry team for introducing the CPR campaign in the wards.
Footnotes
Contributors ROR and RMD contributed equally to project design and implementation, under the supervision of JGB. ROR and RMD wrote the first draft. JGB wrote the second draft. KAH and JMK revised critically for intellectual content and errors. All authors approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.