Article Text

Abstract
Our aim was to test the feasibility of interprofessional, workplace-based learning about improvement through a 4-week placement for one medical and two pharmacy final year students in an Acute Surgical Receiving Unit (ASRU). The target was insulin because this is a common, high-risk medicine in this ASRU and the intervention was medicines reconciliation. Baseline data were collected from 10 patients and used to construct a cause and effect diagram and a process map through feedback and discussions with staff. Hypoglycaemia occurred in four patients but hyperglycaemia occurred in eight patients, of whom six were placed on intravenous insulin infusion (IVII). We estimated that £2454 could be saved by preventing one patient from going on IVII. The students designed and tested a sticker to improve medicines reconciliation for insulin patients. An online form was created to capture clinician feedback on the layout and usability of the sticker. The intervention was associated with improvements in the reliability of medicines reconciliation. The students’ work contributed to a larger project to reduce the risk of hypoglycaemia in the ASRU. This proved beneficial in enabling the students to engage with the clinical team. Nonetheless, it was challenging for students from two Universities to get a shared understanding of improvement methods and work effectively with the clinical team. The students said that they learnt more about quality improvement in a working healthcare environment than they would ever learn in a classroom and they valued the opportunity to work with students from other healthcare backgrounds in practice. Despite the additional staff time required to support students from two Universities, both have supported continuation of this work.
- medical education
- medication reconciliation
- healthcare quality improvement
- reminders
- teamwork
CCBYNC
Statistics from Altmetric.com
Problem
Insulin is a high-risk medicine for hospital inpatients. The 2016 National Diabetes Audit of hospital inpatients reported that 20% of insulin patients had one or more episodes of hypoglycaemia and that 4% of patients had diabetic ketoacidosis during their admission.1 In comparison with other inpatients, patients on surgical wards are at greater risk of insulin prescribing errors1 and patients undergoing emergency surgery are at greater risk of insulin adverse events.2
The Acute Surgical Receiving Unit (ASRU) at Ninewells Hospital receives adult emergency admissions from a widespread area—Dundee, Perth, Fife and sometimes further afield. The ASRU has 27 beds with an additional six bedded assessment bay and two assessment rooms. Patients only tend to stay on the ward for 24–48 hours and are then either discharged or transferred to parent wards. The ASRU pharmacy team were concerned about the accuracy and completion of insulin prescribing and its potential impact on patient care.
As part of an innovative approach to interprofessional education (IPE), the School of Medicine at University of Dundee and the School of Pharmacy & Life Sciences at Robert Gordon University in Aberdeen brought final year students from medicine and pharmacy together to work on a 4-week quality improvement project as a method of widening their IPE experience. The students were supported with online learning resources through the IHI (Institute for Healthcare Improvement) Improvement Practicum.3 The University of Dundee has 5 years experience with using the IHI Improvement Practicum to enable medical students to learn about improvement.3 However, no previous project has involved students from other healthcare professions. This quality improvement forms part of a larger IPE project funded by NHS Education for Scotland which aims to design, deliver and evaluate IPE for medical and pharmacy students from the two institutions.
Background
Hypoglycaemia is a term used to describe when the level of blood glucose falls below 4 mmol/L.4 Patients with diabetes are more likely to experience hypoglycaemia due to irregular blood glucose control. In severe cases, hypoglycaemia can cause convulsions, loss of consciousness or even a coma.4 A study of 33 497 hospital inpatients exposed to hypoglycaemic agents in the USA found that hospital costs were increased by 30% in surgical patients with one or more hypoglycaemic episodes.5
Medicines reconciliation is a formal process used to obtain and verify a complete and accurate list of a patient’s medication. It forms part of the clerking process when admitting patients to Ninewells hospital. In the ASRU, inaccurate medicines reconciliation processes could result in insulin being unnecessarily withheld from patients causing hyperglycaemia or in excessive dosing causing hypoglycaemia. Use of standardised forms for medicines reconciliation was one of five interventions that were identified as likely to be cost-effective for the NHS in a model-based economic analysis.6
Measurement
Working closely with the diabetic team, the ASRU pharmacy team identified five key elements for accurate medicines reconciliation for insulin patients:
Insulin name
Insulin device
Daily dose(s)
Time of administration of each insulin dose
Time of administration of last dose prior to admission
Data were collected by three students (one medical, two pharmacy) for consecutive insulin-dependent patients admitted to ASRU over the 4-week study period.
For this project, baseline data were collected over a 1-week period from 10 insulin-dependent patients in the ASRU. An online Google form was designed to collect the data. Three data sources were used: the medicines reconciliation form in the admissions documentation, the insulin prescription and diabetes monitoring record and the variable rate insulin infusion (VRII) record also known as a sliding scale.
Insulin dose was documented in all 10 patients but recording of the other four items was less reliable: insulin device (three), daily dose (eight), time of administration of first dose (nine) and time of administration of last dose (two). Six patients had hypoglycaemia, eight patients had hyperglycaemia and six patients were put on VRII. No patient had all five items documented.
Design
A cause and effect diagram (figure 1) was constructed based on ward observations and clinicians’ feedback in order to capture the possible causes of hypoglycaemia in insulin-dependent patients. A process map was created to demonstrate the journey of an insulin-dependent patient on acute admission to ASRU (figure 2). Although this was based on ward observations and clinicians’ feedback, we did study the NHS Tayside admission policy as well.

Cause and effect diagram for hypoglycaemia in the Acute Surgical Receiving Unit.
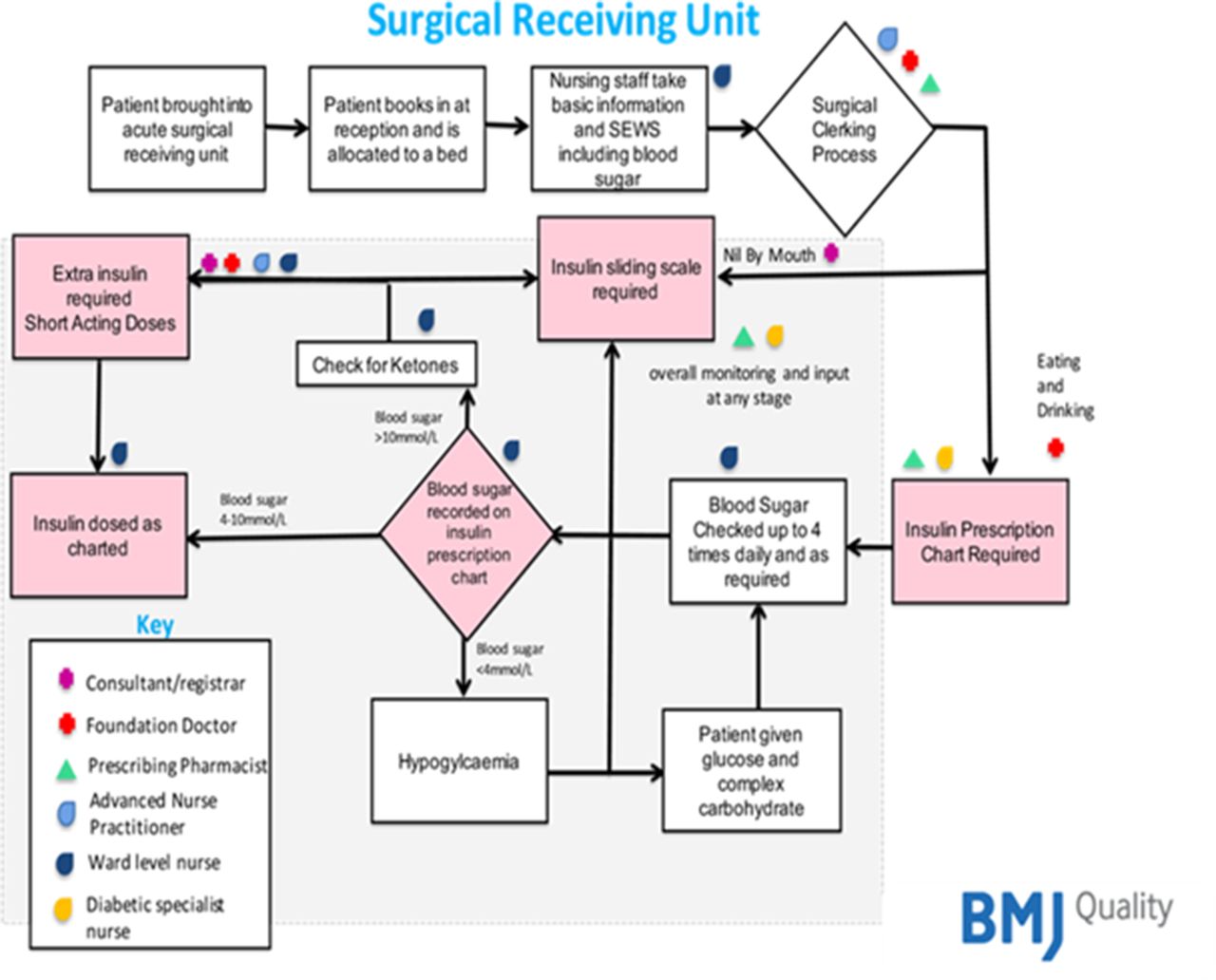
Process map for insulin prescribing and detection of hypoglycaemia or hyperglycaemia on the Acute Surgical Receiving Unit.
We used PDSA (Plan Do Study Act) cycles and discussions with relevant clinicians to design an intervention in the form of a sticker, which was pink to be consistent with the colour already in use for other insulin paperwork in NHS Tayside. The sticker was placed in the admission documentation to capture the four essential insulin details required when admitting insulin-dependent patients which are: insulin name, type of device, dose and time of administration of insulin and last dose taken prior to admission.
Strategy
An online Google form was created to capture clinician feedback on the layout, usability and identification of the sticker in the admissions document. The team used a cloud-based collaborative tool, Slack, which provided students and staff with an online space to share information and resources as well as a communication platform.
The intervention was based on two tests of change, each with multiple PDSA cycles: sticker layout/design and sticker identification/position. Feedback was obtained using the Google ‘sticker feedback form’. Feedback was analysed and used to inform the next iteration of the sticker.
The initial testing involved introducing the clinicians to the project in order to get their buy-in. Initially, the insulin stickers were placed into a number of the admission documents in the ASRU with the expectation that while they are being used to admit patients they would also capture any insulin-dependent patients being admitted within a defined timescale. This test was later repeated because no insulin-dependent patients were captured during this initial test and the timescale was therefore increased. The subsequent test also generated no results and it was concluded that this was due to the low number of insulin-dependent patients admitted to the ward during our testing periods. As a result, we decided to obtain the clinicians’ feedback on the sticker’s usability through a mock simulation using patient admission scenarios. This was repeated with modified versions of the sticker until a final version was agreed. In total, there were three rounds of feedback involving 11 clinicians.
Further testing focused on the implementation of the final sticker into the admission form and continuing to gather clinicians’ comments. Patients were followed up to collect data on any hypoglycaemic and hyperglycaemic episodes and the accuracy of insulin prescription after implementing the stickers.
The final version of the sticker was printed and placed in the admission documents used by clinicians in one ward location. Some patients continued to be missed from the audit due to the fact that multiple locations were used to store admission documentation. The testing continued by ensuring there were enough stickers to cover all admitted patients and they were available in different locations. To help the admitting doctors in ASRU engage in the process, they were encouraged to raise awareness of the insulin sticker during ward handover periods and also help with the design and use of posters to raise awareness of the sticker intervention and the risks of hypoglycaemia. After completion of a number of insulin stickers, the clinicians were contacted to take their feedback by calling them on their bleep numbers and emailing them.
Results
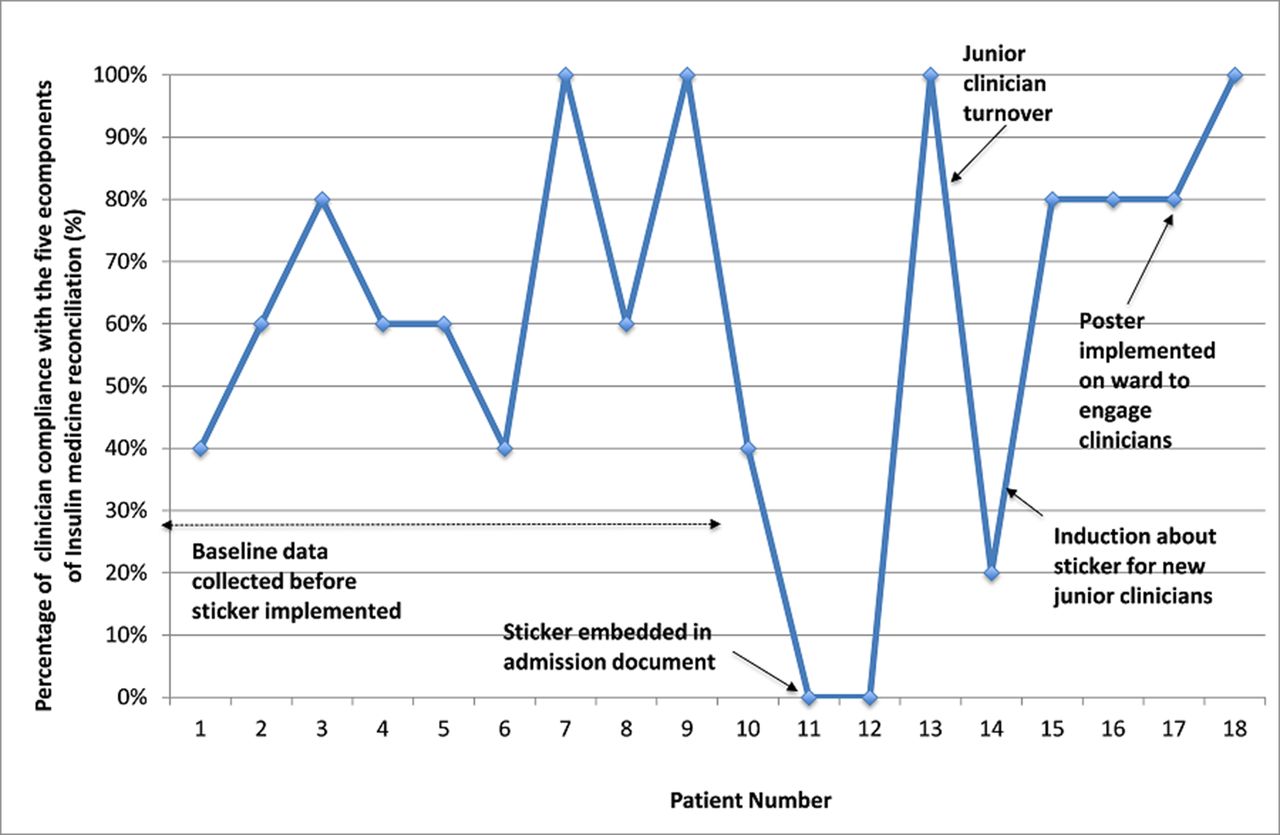
A total of seven insulin-dependent patients were admitted after sticker implementation and five patients had the sticker filled out by clinicians during medicines reconciliation. One doctor did not see the sticker and another doctor was interrupted during the process. Overall, clinician compliance with the sticker increased gradually and after a Foundation Year doctor rotation for the subsequent 5 days, 100% compliance with the insulin sticker for a further five insulin patients was achieved (figure 3).
{kind=link}
{kind=link}
{kind=link}
Run chart of clinician compliance with Insulin medicine reconciliation documentation prior to and after sticker intervention on the Acute Surgical Receiving Unit.
Before sticker implementation, no patients had all four components of insulin medicine reconciliation completed accurately whereas after the intervention four components (name, device, daily dose and time of administration) were being completed 100% of the time by clinicians and the time of the last administration completed 57% of the time which was an improvement from the baseline of 20% (figure 3). Although the patient numbers studied in this project are too small to make any conclusive findings, the increase in insulin medicine reconciliation seen from 64% to 91% over the 4-week course of this project would suggest however that the designed sticker can help improve outcomes if successfully implemented. It is anticipated that more frequent use of the sticker over a longer period of time would help improve familiarity and compliance and would therefore further improve and sustain these observed improvements
Before the start of this project, the ASRU team were focused on reducing the risk of hypoglycaemia in their insulin-dependent patients. However, we found that hyperglycaemia was more common during our 4-week observation period and that this resulted in 6 of 10 (60%) of baseline patients being put on sliding scale insulin. We used the BMJ Cost Calculator to estimate a saving of £2454 per patient prevented from going on a sliding scale. In the postintervention period, two (29%) of seven patients required a sliding scale. Again, the number of patients is small but these results would suggest that use of sliding scale should be included as an outcome measure in future improvement projects.
Lessons and limitations
Learning from this project was multifaceted and related to the project itself and the background learning that the students completing the project gained. Quality improvement science was a new concept for the pharmacy and medical students involved and work to understand the process was occurring while the project was being undertaken. The students’ work contributed to a larger project to reduce the risk of hypoglycaemia in the ASRU. This proved beneficial in giving the students’ improvement project a head start but required time to get a shared team understanding at the appropriate level. Limitations of the project included engagement of staff on the ASRU who rotated regularly and were variable in their engagement in undertaking interventions. The number of insulin-dependent patients admitted to the unit also varied with spells of no admissions meaning that real-time testing of interventions was difficult. Despite this, engagement was achieved and clinicians on the unit could see the benefits of the project. Continuing this piece of work to improve insulin-dependent diabetes care now sits with the ASRU team and thus engagement will be expected to be easier due to having local ownership for a longer time period.
Another limitation to the project was that learner outcomes were not formally assessed. Nonetheless, the students’ feedback indicated that they learnt about identifying and overcoming barriers to introducing an apparently simple change in clinical practice. Their experience with the insulin sticker was similar to results from research findings on the use of surgical checklists7–9 in that the reasons for failure were that staff failed to complete the sticker, found the content to be confusing or unnecessary and perceived that completing the sticker wasted time. They learnt about systems thinking and design10 through process mapping, tests of change and estimation of the costs of VRII (table 1). They commented that they ‘learnt more about quality improvement in a healthcare environment than they ever would in a classroom’ (box 1). In addition to facilitating learning, working with clinical teams meant that they contributed to improving patient care. Although the focus of the project was on designing and testing the sticker, the most lasting impact has been the identification of unplanned VRII as an important outcome measure because it is common, wastes resources and is a potentially avoidable cause of prolonged hospital stay (table 1). A recent integrative review identified 10 previous studies of approaches used to teach quality improvement to preregistration healthcare professionals: However, only one of these 10 studies demonstrated impact on patient care.11 Moreover, although the studies included examples of teaching to medical, nursing and pharmacy students, there were no examples of interprofessional learning.11 At the University of Dundee, we have been using the IHI Improvement Practicum since 2011 and have several examples of completed projects documenting impact on patient care.12 However, this is our first example of interprofessional student-led improvement.
Estimated cost per patient requiring insulin by sliding scale prescription
Comments from students about their experience and its impact on their practice
‘As a pharmacy student, clinical experience in a hospital setting is limited. Working in a clinical area provided the opportunity to engage with the multidisciplinary team, building confidence and a sense of resilience.’
‘Working collaboratively proved to be challenging at times requiring compromise.’
‘Students learn more about QI in a working healthcare environment than they would ever learn in a classroom. It provides the opportunity to work interprofessionally with students from other healthcare backgrounds in practice.’
‘Students get to experience real patient and staff interaction in a clinical environment and learn about all the challenges QI projects face during intervention implementation and sustainability.’
‘From a post-graduate perspective this inter-professional project helped set me up for work as a pre-registration pharmacist. I became confident working/communicating with members of the MDT. I learnt how different MDT members have different priorities for providing patient care.’
The use of technology proved to be both a strength and a limitation. Several applications and online tools were used to record data, gather feedback, analyse and represent results, such as Google drive, Google forms and Slack. The latter was particularly useful as an online communication platform to discuss any issues when the team were apart and also allowed supervisors to follow progress remotely. However, challenges included limited access to computers and meeting rooms for preparing tasks and writing up aspects of the project. iPads were used to complete the online forms but reviewing them required an internet connection and an intermittent signal occasionally led to the loss of the information.
The additional IPE aspect was beneficial with students from different professional backgrounds learning about the training and role of members of the multidisciplinary team. The students gained an appreciation of the time required to reach a consensus view on how to approach aspects of the project. This appreciation arose from them having different experiences of the clinical environment, requiring them to use their different knowledge and skills to reach a compromise on shared priorities and solutions. In addition, the pharmacy students required some orientation as they were exposed to a new clinical environment and using NHS Tayside paperwork which differed from NHS Grampian. However, they were able to undertake shadowing with clinical pharmacists and diabetic specialist nurses which was of value to their professional development. Student reflections were positive (box 1).
An important lesson for NHS Tayside was that early attempts by the team to take this work forward failed due to lack of time and staff resource. There are renewed efforts however to revisit this improvement project in 2018 with a committed multidisciplinary team of young pharmacists and junior doctors as a shared collaboration.
One of the main lessons for the Universities was that the scope and scale of the improvement effort was restricted by choosing a relatively rare patient population. In future, assigning student improvement teams to a problem that is more frequent or has a process measure that is more frequent may allow for more rapid testing within a 4-week Student Selected Component.
Conclusion
This first phase of a wider quality improvement project, which aimed to ‘improve the reliability of insulin prescribing and decrease the risk of hypoglycaemia in insulin dependent patients by 50% within 72 hours of admission to hospital’ resulted in the development of a sticker intervention which was shown to improve compliance with insulin medicines reconciliation. Over a 4-week period, compliance increased from 64% to 91%. The target of 95% compliance was not met due to the limited timescale for this first phase. Despite there being some challenges engaging staff due to high turnover, the majority thought the intervention was beneficial and that it was a useful prompt for asking patients about their insulin. The potential to release cost savings by reducing the number of patients requiring an intravenous insulin infusion was also identified. Ownership of this phase of the project has been handed to the ward clinicians who will continue to collect data to measure the impact of this intervention.
From the perspectives of the Robert Gordon University and the University of Dundee, this work demonstrated the potential for pharmacy and medical students to learn improvement methods by testing change in the workplace. We plan to increase capacity for interprofessional learning on quality improvement in the future.
Footnotes
Contributors VT and PD (first and last authors) are coleads for the Patient Safety SSC (Student Selected Component). All other authors made equal contributions and are listed in alphabetical order by surname. VT, PD, AA, IR and AS designed the educational intervention and provided academic supervision for the students. SB designed the improvement intervention and was the clinical supervisor for the students. SA-S, IC and RF designed and tested the changes and measures for improvement. All authors contributed to writing up results and commented on drafts of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional data from this study.