Article Text

Abstract
Microbial resistance to antibiotics is a serious global health problem compounded by antibiotic overuse and limited investment in new antibiotic research. Inappropriate perinatal antibiotic exposure is increasingly linked to lifelong adverse outcomes through its impact on the developing microbiome. Antibiotic stewardship may be the only effective preventative strategy currently available. As the first tertiary neonatal unit in the UK to collaborate in an international quality improvement programme (QIP) with Vermont Oxford Network (VON), we present the results of our antibiotic stewardship initiative.
The QIP was officially launched in January 2016 and aimed to reduce antibiotic usage rate (AUR) by 20% of baseline by 31st December 2016 without compromising patient safety. A multidisciplinary team of professionals and parent representatives shared good practices and improvement strategies through international webinars and local meetings, devised uniform data collection methodology and implemented a number of carefully selected ‘Plan–Do–Study–Act’ cycles. Run charts were used to present data and, where appropriate, statistical analysis undertaken to compare outcomes.
The QIP resulted in a sustained reduction in AUR from a baseline median of 347 to 198 per 1000 patient-days (a reduction of 43%). The proportion of culture-negative sepsis screens where antibiotics were stopped within 36–48 hours increased consistently from a baseline of 32.5% to 91%. The antibiotic days per patient at discharge reduced from a median of 3 to 2 days, and there was a reduction in practice variation. Our annual mortality and necrotising enterocolitis rates for the VON cohort (<30 weeks or <1500 g) were the best ever recorded, 5.5% and 1.4%, respectively. Audits confirmed a high level of staff and family awareness of the QIP.
The QIP achieved a sustained reduction in antibiotic use without compromising patient safety. Our challenge is to sustain this improvement safely.
- antibiotic management
- critical care
- quality improvement
- quality measurement
- teamwork
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Problem
Microbial resistance to antibiotics is a serious global health problem compounded by antibiotic overuse and limited investment in new antibiotic research. There are specific concerns that inappropriate antibiotic exposure in the perinatal period can lead to both short-term and lifelong adverse outcomes. In contrast, the neonatal population is vulnerable to infection and antibiotics could be lifesaving. The only effective strategy is to rationalise and reduce the inappropriate use of antibiotics. Implementing change in this setting would require strong evidence of benefit that outweighs the risk for the population, the weight of a powerful collaborative to influence a paradigm shift, strong clinical leadership and partnership with families. Our neonatal unit (NNU) was the first in the UK to collaborate in an international quality improvement programme (QIP) with the Vermont Oxford Network (VON) and the Centers for Disease Control and Prevention (CDC) to rationalise and safely reduce antibiotic use. In January 2016, a multidisciplinary team of professionals agreed a SMART aim to reduce antibiotic usage rate (AUR) on the NNU by 20% of baseline by 31st December 2016 without compromising patient safety.
Singleton hospital hosts a 24-bedded NNU in Swansea, the second largest city in Wales. It serves a population of 1 million in South West Wales, a mixture of dense urban and sparsely populated rural areas. The unit provides comprehensive medical intensive care for all newborn infants from 23 weeks gestation onwards. Surgical care is provided at the regional centre in Cardiff. The unit caters for 10 000 births in the region and manages approximately 100 very low birthweight infants a year; 20% of all admissions are out born. The unit employs 125 whole time equivalent staff members. However, the number needed to influence this multidisciplinary team is significantly higher due to part-time working and trainees on rotational placements.
In this paper, we report our experience of developing and managing a QIP on safe reduction of antibiotic usage in a tertiary NNU conforming to the ‘Standards for Quality Improvement Reporting Excellence’ (SQUIRE 2.0) guidelines.1
Background
Microbial resistance to antibiotics has risen rapidly over the last two decades with emergence of super-resistant microbial strains that do not respond to the commonly used antibiotics. Antibiotic use increases the presence of resistance genes in the bacteria and further exposure selects for different sets of resistance leading to development of multidrug resistance organisms (MDROs) in the gut microbiota. Studies confirm a much wider spectrum of antibiotic resistance genes in the gut microbiota of preterm babies who had received antibiotics.2–4 It is probable that MDROs persist in the host microbiome for a lifetime and may even be passed to the next generation. The situation is compounded by limited investment in new antibiotic research; only two antibiotic classes have been introduced in the last 50 years with very few new products in the pipeline.5 New antibiotics will take many years to filter into clinical practice, and until then, the only effective strategy is high-quality antibiotic stewardship.
The magnitude of this serious global health problem is highlighted by the 2014 WHO report, warning of the dangers of a postantibiotic era, in which common infections and minor injuries could be fatal.6 This has prompted calls in the USA and the UK for national action plans to combat antibiotic resistance.7 US President Barack Obama published a white paper that led the CDC to launch a collaborative QIP with VON, the world’s largest neonatal benchmarking organisation.8
NNUs are traditionally at risk of antibiotic overuse. The setting is highly emotive and the perception of risk is high as it concerns a vulnerable and immunologically immature population, exposed to many invasive procedures and with a high incidence of clinical instability, often erroneously attributed to infection. It is common to commence empirical antibiotic treatment. ‘Treat first, think later’ is the custom and practice and can lead to a defensive mindset. Yet, the overall incidence of true blood culture-positive early-onset sepsis is low (0.7–1/1000 live births overall); lower still in the term and near-term infants.9 10 The incidence in babies who are admitted to NNUs is 5.6/1000.11 The majority of infants are treated unnecessarily with antibiotics, and the number needed to prevent one true sepsis is very large. A large retrospective cohort study in 127 NNUs in the USA reported wide variation in AUR. There were no differences in rates of proven sepsis, necrotising enterocolitis (NEC), surgical case volume and mortality between the high and the low prescribing units. The only difference between the units was the rate of suspected clinical sepsis, suggesting an avoidable inappropriate use of antibiotics.12
Of greater concern are reports from many other studies where early use of antibiotics without proven morbidities, especially in the first week of life, is associated with increased risk of subsequent mortality and diseases such as late-onset sepsis, NEC and severe retinopathy of prematurity.13–17 The effect size of these adverse events increased with the duration of early antibiotic use.
There is emerging evidence that administration of antibiotics in early life has profound and lifelong adverse effects. The perinatal period is critical for the establishment of the intestinal microbiome. The ‘sterile womb’ theory, whereby the ‘sterile fetus’ first acquires bacteria by passing through the birth canal, has been recently challenged. Studies suggest that the colonisation of the fetal gut may in fact commence prior to birth by bacterial translocation from the maternal oral cavity and gut via the circulation or ascension from the vagina.18 The infant microbiome modulates the immune system development and produces metabolites, important in ‘cross-talk’ between the two. Antibiotic use in pregnancy and the neonatal period results in altered composition of the microbiome (bacterial dysbiosis). This can potentially disrupt the complex immunological development at a critical stage, leading to chronic inflammation with lifelong sequelae.19 20 Bacterial dysbiosis in early life may thus be linked to disease processes such as inflammatory bowel disease, diabetes mellitus, allergic disease and obesity.21–25
Measurement
Our primary outcome measure was the AUR calculated as the number of days of antibiotic use per 1000 patient-days. We collected these data separately for blood culture-positive and blood culture-negative patients, as well as by antibiotic class. Moreover, we agreed on three process measures:
The proportion of culture-negative septic screens where antibiotics were stopped appropriately at 36–48 hours=number of culture-negative septic screens where antibiotics were stopped at 36–48 hours × 100/total number of culture-negative septic screens.
The proportion of infants who never received antibiotics during their entire stay on the NNU=number of infants who never received antibiotics during admission × 100/total number of babies admitted to the NNU.
Antibiotic usage days per patient at discharge.
The department submitted and analysed outcome data on mortality and common morbidities through VON Nightingale system and Badgernet, a live internet-based electronic database widely used in the NNUs in the UK (Clevermed, Edinburgh, UK). Critical incidents were reported and investigated through the critical incident reporting system (DATIX, London).
In the absence of existing reporting system on antibiotic usage, we agreed and adhered to a written data collection methodology before embarking on the QIP. To ensure reliability of the data source, we triangulated data on antibiotic usage from three independent sources between November 2015 and January 2016:
Pharmacist-led prescription chart audit.
Medical review of clinical notes.
Badgernet electronic portal—daily entry of medications by nurses including antibiotics.
Following a high degree of conformity, Badgernet was the agreed data source for prospective monitoring. Data from November 2015 until January 2016 served as baseline. We excluded routine fluconazole prophylaxis in high-risk preterm infants and trimethoprim for renal conditions from analysis as clinicians were reluctant to change this practice. We used two rotating teams of nurses, doctors and nurse practitioners every three months for data collection and analysis to avoid data fatigue and monotony. We reviewed data every 15 days and reported to the wider team every month, earlier if a trigger threshold was reached. Sequential data over time were presented as run charts and quantitative data at the beginning and end of the QIP analysed using non-parametric statistical tests.
Our baseline measurements showed the following:
The overall median AUR was 347/1000 patient-days and 268/1000 patient-days in culture-negative sepsis.
The proportion of culture-negative sepsis screens where antibiotics were stopped within 36–48 hours was 32.5%.
The proportion of admitted infants who had no exposure to antibiotics at discharge was 21.9%.
The median antibiotic days per patient at discharge were 3.
In early February 2016, we participated in a VON day spot audit that benchmarked our NNU’s AUR on the 50th–75th centile when compared with other participating centres across the world.
Design
A multidisciplinary team of professionals (medical and nursing staff, advanced nurse practitioners, pharmacists and administrative staff) and parents joined the QIP collaborative ‘Choosing Antibiotics Wisely’ in December 2015. The programme was officially launched in January 2016. Funding was obtained from the unit’s ‘Training and education charitable fund’ with support and encouragement from senior clinicians, managers and executives. The project was reviewed by the institution’s ‘NHS Research and Development’ department and classed as ‘Quality Improvement’ rather than ‘Research’. The project was therefore exempt from ethical approval and consent process.
The team joined in a series of live webinars organised by VON where world experts presented a balanced analysis of the benefits of antibiotic use in the at-risk neonatal population with the potential harm that inappropriate usage may have on short-term and long-term outcomes. They offered judicious improvement strategies and shared success stories. The webinars included robust sessions on quality improvement methodology. A learning management system offered access to handouts, video recordings of lectures, toolkits and discussion forums. The webinars were followed by local deliberations in academic meetings to agree and implement good practices that suited our own clinical setting. Our primary drivers were enshrined in four basic pillars—to establish a culture of antibiotic stewardship, maintain partnership with staff and families, avoid inappropriate prolongation of antibiotics and introduce consensus guidance to safely reduce initiation of antibiotics in selected low-risk infants. The guidance for non-initiation was balanced by a safety net of enhanced clinical review through repeated physical examinations and laboratory tests undertaken by senior clinicians.
Strategy
Multiple initiatives were undertaken to ensure staff and families were aware and actively involved in the programme (Plan–Do–Study–Act (PDSA) 1). Information about infection and the pros and cons of antibiotic use was disseminated through posters displayed on the unit. Leaflets in the admission pack for parents encouraged them to be present on ward rounds and ask questions about their baby, and specifically about antibiotic use. Such information was mixed with other health promotion messages such as breastfeeding and infection control measures to reduce unnecessary anxiety. Weekly parent education classes (as part of our developing family integrated care programme) further reinforced these messages. Noise-reducing headphones ensured that parents could stay at their baby’s cot side during lengthy ward rounds, while maintaining confidentiality rights of other families on the unit. Signed and dated stickers on prescription charts confirmed that nurses/doctors had communicated information on any new antibiotic prescription to the parents. One highly motivated parent even attended the initial VON webinar. Parents and staff were also reassured by the availability of enhanced early warning systems on the unit such as predictive Heart Rate Characteristics (HRC) monitoring system. Staff and parent awareness audits were built in the programme at different times to assess and heighten awareness.
Once these processes were established, we sequentially introduced a series of further clinical PDSA cycles to reduce antibiotic use:
PDSA 2 (March 2016): Introduction of stickers on prescription charts to trigger mandatory review of antibiotics at 36 hours, backed up by additional scrutiny on daily pharmacist-led ward rounds.
PDSA 3 (April 2016): Introduction of non-initiation of antibiotic guideline in low-risk admitted infants>34 weeks (online supplementary appendix 1). This was agreed through a review of risk factors in all cases of culture-positive early-onset sepsis over a 10-year period in our institution. Although the process was tested, the number of babies eligible was too small to make a difference and this led to PDSA 4.
PDSA 4 (June 2016): Lowering of the gestation limit to >30 weeks for non-initiation of antibiotics supported by biweekly PDSA review. The intervention risk was balanced by repeated clinical reviews, additional laboratory tests and HRC monitoring (online supplementary appendix 1). Data on adverse effects such as delayed treatment leading to harm, death, NEC, late-onset sepsis and mortality were collected through routine incident reporting and data collection tools.
PDSA 5 (July 2016): Stopping antibiotics earlier than initial predicted course in culture negative well infants, if C-reactive protein (CRP) <10 (online supplementary appendix 2).
Supplemental material
Supplemental material
Many other initiatives also took place concurrently including specifying the minimum blood volume of 1 mL for blood cultures, expediting transit time to the laboratory, facilitation of 36 hours blood culture reporting, introduction of central line care bundles and family integrated care programme.
Results
Over the 14-month period of the QIP (November 2015–December 2016), 523 infants were admitted to the NNU and 526 were discharged. During the QIP we reduced our AUR from a baseline median of 347/1000 patient-days to 198/1000 patient-days, a reduction of 43% and twice that of our original SMART aim of 20% reduction, that is, 277/1000 patient-days. This reduction was evident across all antibiotic classes. The AUR in blood culture-negative episodes reduced from a baseline median of 268/1000 to 153/1000 patient-days, a reduction of 43%.
Figure 1 shows an annotated run chart of monthly AUR with PDSAs and VON webinars plotted along the timeline. The green line indicates the SMART AUR reduction goal, while the red line represents the median over the entire QI period. As the PDSA cycles were introduced and awareness heightened through VON webinars, there was a definite trend towards reduction in AUR. The readers will note a deviation in early September 2016, where a peak in AUR coincided with the arrival of new trainees on rotational clinical placement.
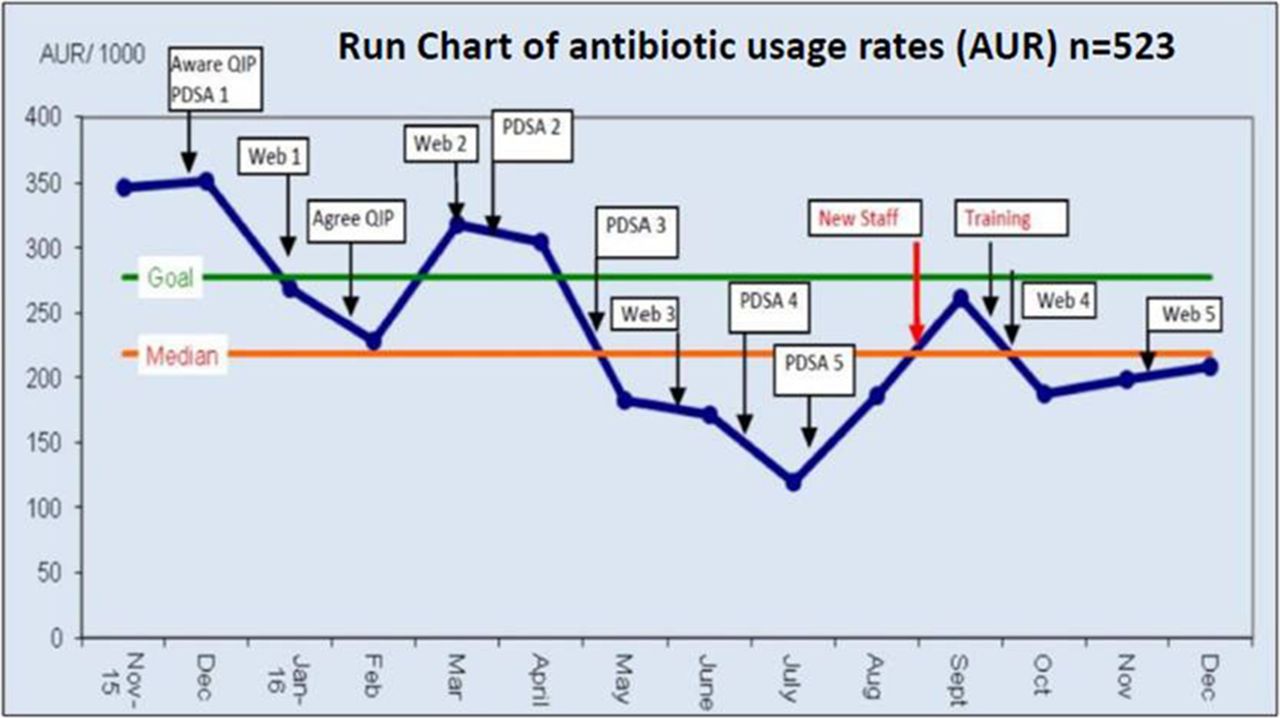
Run chart of monthly antibiotic usage rate (AUR) during the quality improvement programme (QIP). PDSA, Plan–Do–Study–Act.
Figure 2 shows the same monthly AUR superimposed on bar charts representing frequency of blood culture-positive sepsis. The turquoise line represents the total AUR and the red line AUR in culture-negative episodes only. As one would expect from a safe QIP, when there was an increase in the number of positive blood cultures in March 2016, there was also a corresponding rise in total AUR, but the AUR in culture-negative episodes remained stable. In contrast, in September 2016, despite the observed low incidence of positive blood cultures, there was a rise in both the total and culture-negative AUR, suggesting inappropriate antibiotic use, which coincided with new rotational medical trainees joining our team.

Line chart of monthly antibiotic usage rate (AUR) (overall and that in infants with negative blood culture) in relation to the frequency of blood culture-positive sepsis.
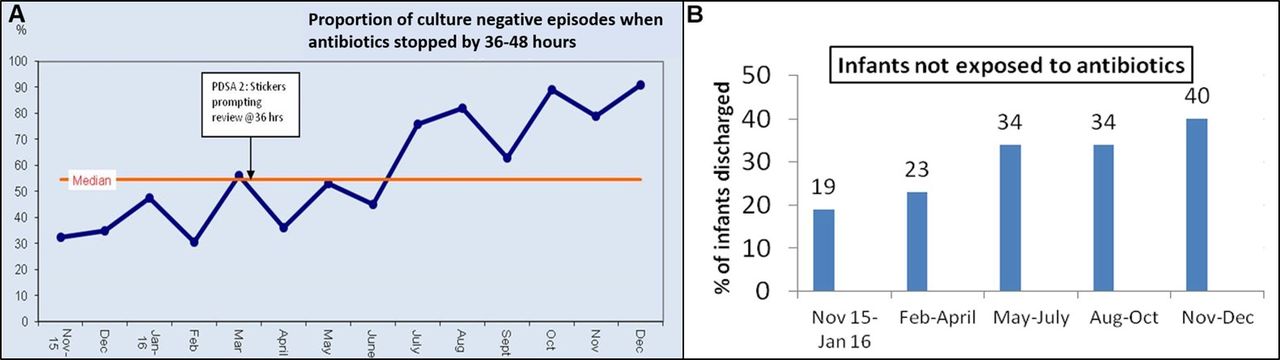
Figure 3A is a run chart showing the proportion of culture-negative sepsis screens where antibiotics were stopped at 36–48 hours. The median is indicated by the red line. The specific PDSA related to ‘STOP and Review’ of antibiotic prescription at 36 hours is annotated along the timeline. There is a definite and sustained increase in early discontinuation of antibiotics in infants with negative sepsis screens throughout the duration of the QIP from a baseline of 32.5% to 91%. figure 3B shows, in three monthly epochs, the proportion of admitted infants who had no exposure to any antibiotics at discharge; this nearly doubled from 21.9% to 41.2%.
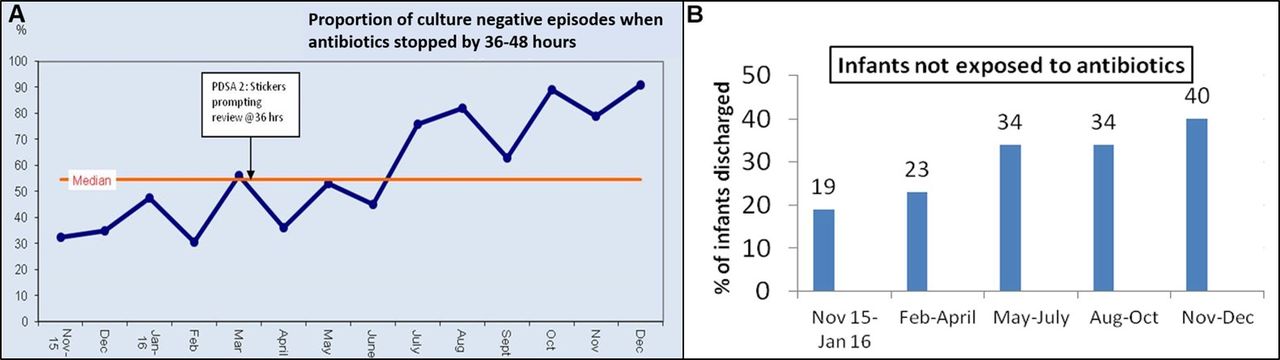
(A) Run chart of proportion of infants where antibiotics were discontinued at 36–48 hours in infants with negative sepsis screens. (B) Bar chart showing the proportion of infants discharged without any exposure to antibiotics at discharge from the neonatal unit during the quality improvement programme. PDSA, Plan–Do–Study–Act.
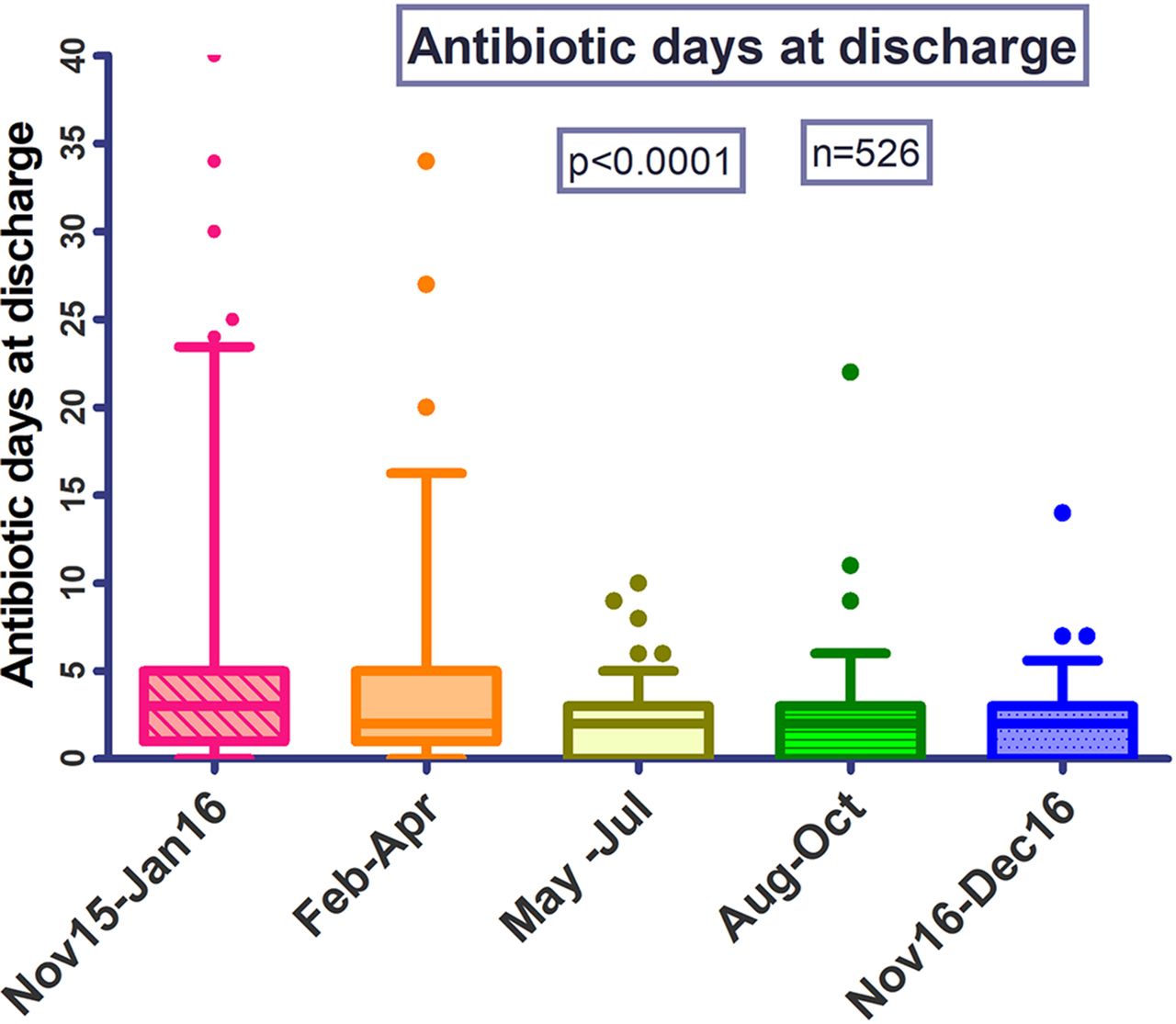
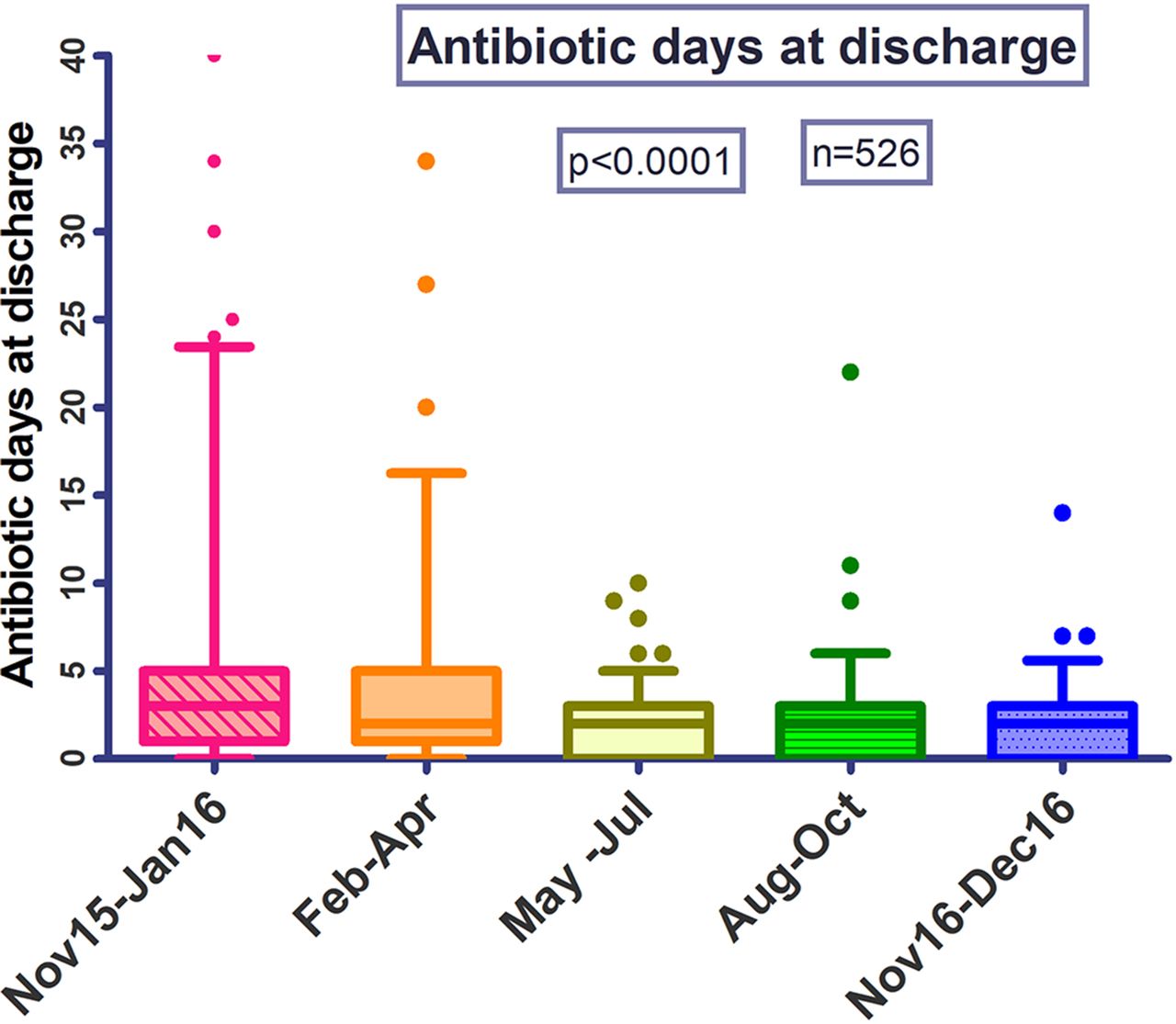
Figure 4 is a box-and-whisker plot of days of antibiotic exposure at discharge per patient, displayed in three monthly epochs. The median antibiotic days per patient at discharge reduced from three to two, and this drop was highly statistically significant (p<0.0001). There was also a reduction in practice variation as evident from reduction in the length of the whiskers over the QIP period.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box-and-whisker plot of antibiotic days at discharge in three monthly epochs during the Quality Improvement Programme.
Our staff audit showed nearly 100% awareness of the QIP; >85% of the staff knew when to stop antibiotics in well babies if their blood cultures were negative. They were also aware of the magnitude of AUR reduction achieved through the QIP.
A random sample of the families participated in an audit of antibiotic usage in their babies. All except two received the information leaflet; 88% of responders knew why their baby was on antibiotics and the projected duration of treatment.
During the QIP, no critical incidents related to missed or delayed identification and treatment of sepsis were reported. We noted a slight increase in the rate of culture-positive sepsis (19.4%) compared with the previous years (14.3% in 2015, 16.9% in 2014). Despite that, we recorded our lowest ever case-mix-adjusted mortality and NEC rates in 2016. In the high-risk VON cohort, mortality rates were 5.5% in 2016, 12.3% in 2015% and 14% in 2014, while for NEC, the rates were 1.4% in 2016, 4.9% in 2015 and 7.6% in 2014.
Lessons and limitations
The strength of our QIP was the enthusiasm and cohesiveness of the team members and their willingness to make a difference. The QIP was highly visible with posters on display, information leaflet for parents, frequent team meetings and staff newsletters. Surveys confirmed high level of parent awareness and support. Staff and sometimes parents sacrificed their personal time to join out-of-hours international webinars. PDSAs were debated, refined and implemented by different subteams to ensure wider engagement.
Our QIP was not without its challenges. The initial challenge was to mitigate risks of deviating from custom and practice, handle small pockets of scepticism and support clinicians out of their comfort zone in fear of adverse clinical incidents. These were managed by small graded steps of positive changes, enhanced monitoring to prevent major setback and loss of confidence and frequent dissemination of measures of progress. To motivate, sustain and educate a team during a period of unprecedented staffing crisis in the National Health Service was challenging and educational for future programmes. However, on our unit this resulted in a number of consultant staff undertaking resident duties to maintain service and thereby offering a wealth of experience and wise professional judgement that may otherwise not have been immediately available on the floor.
As shown in figure 2, there was a steep rise in AUR in September 2016, coinciding with the arrival of new rotational staff. This was identified and managed with additional teaching sessions reinforcing changes in our practice and the results achieved through the QIP. This highlights the importance of including the QIP in induction programme for new staff members.
Conclusion
The results of our QIP showed a definite change in the culture of antibiotic stewardship on our unit leading to a sustained reduction of antibiotic use. There are many underlying reasons for this initial success. A clear rationale and evidence base for the intervention was available. Prior to the QIP, we were mindful that the neonatal intensive care environment caters for high-risk vulnerable infants and major deviations from a generally risk-averse practice would need to be well balanced, evidence-based and implemented in collaboration with reputable partners such as VON and CDC to provide confidence to the local team. The QIP was supported by senior Health Board executives and led by a nominated Consultant Neonatologist. While the generic principles of the collaborative approach were useful, we ensured that the interventions in our PDSA cycles were pragmatic and appropriate for our patient profile, staffing patterns and infrastructure including methods of data collection, monitoring and reporting. The use of two teams for data collection and reporting in three monthly rotation was particularly effective in reducing data fatigue and monotony. Our staff and parent awareness audits showed high level of engagement, and this partnership was perhaps the most important factor in our success and sustainability. We launched this programme at a time when the unit was also developing its family integrated care programme; antibiotic stewardship was an ideal project where transparency and shared decision-making could be put to the test and implemented.
After multiple deliberations, the team agreed a SMART aim of a 20% reduction in AUR over a 12-month period. Although a sustained reduction of AUR by 43% of baseline may portray our initial aim as modest, at the time we felt that this goal was ambitious, realistic and unlikely to curb our initial enthusiasm through disappointment. It is well recognised that the approach to setting targets will vary depending on the organisation’s current performance on an indicator, whether current benchmarks are available, careful assessment of what is feasible in the local healthcare environment and based on ‘best known’ similar processes.26 Most units participating in the VON collaborative had set a target of 10%–20% reduction in AUR. In our situation, the baseline AUR had to be determined, robust benchmarking data was being collected through the programme and the perception of risk related to a missed or delayed treatment of sepsis was very high.
The reduction in AUR was primarily achieved by limiting the duration of antibiotics in culture-negative sepsis screens and non-initiation of antibiotics in low-risk clinically well babies. Most importantly, this reduction has been sustained without any adverse events. While planning our PDSA cycles on non-initiation of antibiotics we were mindful of the effect that missed sepsis may have on the infant and their family and on team confidence. We were stringent on the need for frequent clinical review and documentation and would reverse the initial decision of non-initiation promptly if the situation changed. An interim guideline was agreed after reviewing risk factors in all cases of culture-proven sepsis over a 10-year period and this offered reassurance to junior medical and nursing staff. Non-initiation of antibiotics was introduced in low-risk, more mature babies initially, lowering the gestation in small steps to allow staff to get familiar and confident with new guidance and safety reviews (online supplementary appendix 1). The availability of predictive heart rate characteristics monitoring system on our unit provided added confidence.
During the QIP, we recorded our lowest annual incidence of all-cause mortality and NEC for over a decade. We believe this was due to a combination of direct beneficial effect of reduced antibiotics use on microbial flora as well as the increased vigilance and safeguards put in place to manage the perceived risks of the programme. The slight increase in the rate of culture-positive sepsis during the QIP could be due to a change in practice of ensuring that a minimum of 1 mL of blood is used in blood culture, thereby increasing its sensitivity.27 Similar reports of reduction in morbidity and mortality associated with antibiotic stewardship have been reported in recent publications. Analysis of prospectively collected antibiotic usage data between 1990 and 2014 in a tertiary NNU in Sydney, Australia, showed that it is safe to stop antibiotics within 2–3 days in culture-negative, clinically well babies. No infants with negative cultures relapsed with sepsis when antibiotics were stopped after 48–72 hours. Since the AUR reduced over the study period as a result of antibiotic stewardship, there was a gradual decrease in rates of late-onset sepsis, particularly in the very low birthweight infants.28
In conclusion, to our knowledge, we are the only neonatal centre in the UK to have run such a systematic and bold campaign with international collaborators to reduce antibiotic use. We have demonstrated that reduction in antibiotic usage is possible through introduction of prudent and evidence-based practices without compromising patient safety. Most importantly, this QIP was implemented in partnership with staff and family and the culture of change is palpable and evident in every dataset we have presented. The confidence of sustained improvements has led to successful PDSAs being adopted formally into clinical guidelines. Our methods are generalisable and have enthused other clinical teams to consider similar initiatives. The challenge is to sustain this positive change over a longer period of time and a second year of the programme will ensure improvements are embedded in practice and focus on scope for improvement on the postnatal ward. While there were cost savings from reduced antibiotic use, the greatest impact was the indirect savings and health benefits related to reduced mortality and morbidity.
Acknowledgments
The authors thank all the staff and families on the neonatal unit for working together, the managers and executives for supporting this programme and the VON/CDC collaborative for their excellent support and guidance. A special thanks to Mrs Kerri Kelleher for being the lead parent representative for the programme.
References
Footnotes
Contributors SB and JM conceived the idea of this Quality Improvement Programme and collaborated with Vermont Oxford Network. VM, GD, SC, KW, LW and SB collected and analysed the data. JW, GM, AK, MM, LW, JT and SB designed and led the various PDSA cycles. VM and SB drafted the initial version of the manuscript, and all other authors contributed in reviewing and editing the manuscript to its submitted version.
Funding The quality improvement programme did not have any specific funding but a single annual payment of $3900 was paid to Vermont Oxford Network to join the iNICQ curriculum.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.