Article Text

Abstract
Community rapid response and rehabilitation teams are used to prevent avoidable hospital admissions for adults living with multiple long-term conditions and to support early hospital discharge by providing short-term intensive multidisciplinary support. Supporting self-management is an important service intervention if desired outcomes are to be achieved. A Care Quality Commission inspection of the Richmond Response and Rehabilitation Team in 2014 identified that self-management plans were not routinely developed with service users and reported this as requiring improvement. This quality improvement project aimed to develop and implement a self-management strategy for service users and for 90% of service users to have a personalised self-management plan within 3 months. The quality improvement intervention used the Plan-Do-Study-Act model comprising: (1) the development of a self-management plan, (2) staff education to support service users to self-manage using motivational interviewing techniques, (3) piloting the self-management plan with service users, (4) implementation of the self-management plan and (5) monthly audit and feedback. Evaluation involved an audit of the number and quality of self-management plans developed with service users and a survey of staff knowledge and confidence to support service users to self-manage. Following implementation of the intervention, the number of self-management plans developed in collaboration with service users increased from 0 to 187 over a 4-week period. Monthly audit data confirmed that this improvement has been sustained. Results indicated that staff knowledge and confidence improved after an education intervention. Quality improvement methods facilitated development and operationalisation of a self-management strategy by a community rapid response and rehabilitation team. The next phase of the project is to evaluate the impact of the self-management strategy on key service outcomes including self-efficacy, unplanned and emergency hospital admissions and early discharges.
- older people
- self-management
- quality improvement
- rapid response and rehabilitation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Problem
The Richmond Response and Rehabilitation Team (RRRT) is a multidisciplinary, integrated health and social care team within the London Borough of Richmond. At the time of this quality improvement project, the team comprised 54 staff members (nurses, physiotherapists, occupational therapists, social workers, therapy assistants and rehabilitation assistants) and had three key areas of responsibility for adult services: hospital discharge, rapid response and community rehabilitation. Approximately 40% of referrals to the team are received from the community and 60% from hospitals. The RRRT provides assessment and support plans for discharge from hospital to home or social care placement. A rapid response service is provided to manage crises and support people to stay at home, preventing unnecessary admission to an acute hospital or care home. The RRRT puts in place individualised care support, equipment and multidisciplinary team interventions to prevent unnecessary admissions. If the person would benefit from community rehabilitation, the team will continue to support them for up to 6 weeks.
The typical service user of the RRRT is an older person (aged 65 years and over) with one or more long-term conditions, living in the Borough of Richmond or registered with a Richmond general practitioner (GP). Approximately 198 500 people are registered with a Richmond GP. One in three of those registered has one or more long-term conditions and 1 in 10 has three or more.1 Overall, the emergency hospital admission rate in Richmond is among the lowest in the country.2 However, around 2073 (15%) emergency admissions (costing £4.2 million per year) are for potentially preventable conditions.1
The development of self-management plans with service users is an organisational key performance indicator (KPI) for the RRRT. However, the monthly KPI RAG rating (a traffic light rating system) for self-management plans had been consistently in the red. Furthermore, a Care Quality Commission inspection in 2014 identified that self-management plans were not routinely developed with service users and reported this as requiring improvement. The aim of this quality improvement project was to develop and implement a self-management strategy for service users and for 90% of service users to have a personalised self-management plan within 3 months.
Background
More than 15 million people in the UK have a long-term condition such as hypertension, depression, asthma, diabetes, coronary heart disease, chronic kidney disease or other health problem or disability for which there is no cure.3 The number of people with multiple long-term conditions is expected to rise to 2.9 million in 2018.4 Nationally, the care of adults with long-term conditions uses around 70% of the healthcare budget.4 Addressing the rising costs of care associated with long-term conditions, especially those generated by unplanned and emergency hospital admissions, is a key area of policy focus for the UK government. A study by Nesta estimated that £4.4 billion could be saved in the UK National Health Service (NHS) through greater patient participation and self-management of long-term conditions,5 and a King’s Fund6 policy paper recommended active self-management support as the number one priority for commissioners to deliver financial sustainability of the NHS. Despite the increasing policy focus of supported self-management,4 7–11 its implementation in the UK remains patchy and disjointed.12
Self-management is defined as: ‘The actions individuals and carers take for themselves, their children, their families and others to stay fit and maintain good physical and mental health, meet social and psychological need, prevent illness or accidents, care for minor conditions and maintain health and well being after an acute illness of discharge from hospital’ (Phillips 201213, p.33). The response of health and social care organisations comprises services that enable people to self-manage13 through: ‘The systematic provision of education and supportive interventions by healthcare staff to increase patients’ skills and confidence in managing their health problems, including regular assessment of progress and problems, goal setting and problem solving support’14 (p. 59).
Despite the growing policy focus on supported self-management, we know that older people experiencing some of the conditions common to ageing are less likely to receive this support.15 16 UK health services perform badly compared with other countries in involving patients of all ages in shared decision making and supported self-management17; for example, older people report less education and support in self-management of diabetes.16 There is evidence that care and support for older people with long-term conditions is unjustifiably inequitable.18–20 With this in mind, localities should examine local performance to ensure that older people are not disadvantaged.21
Guidance on implementing self-management locally is provided by the House of Care Model.3 22 The House of Care Model has been adopted as a central metaphor in NHS England’s plans for improving care for people with long-term conditions.23 It is based on Wagner’s24 chronic care model that has influenced global health policy and emphasises a proactive healthcare approach to supporting patients to self-manage rather than a reactive approach when a person is sick.
Aim
The aim of this quality improvement project in the RRRT was to develop and implement a self-management strategy for service users, drawing on the House of Care Model, and for 90% of service users to have a personalised self-management plan within 3 months.
Project objectives were:
Development of a self-management care plan by June 2015.
RRRT staff to be trained in collaborative goal setting and problem solving using the principles of motivational interviewing (MI) by August 2015.
90% of RRRT service users to have a personalised self-management plan at initial assessment by November 2015.
RRRT staff to incorporate self-management support into routine care by December 2015.
Measurement
Baseline measurement comprised an audit of self-management plans and a questionnaire survey of RRRT staff to determine baseline attitudes, beliefs and knowledge about self-management. These data indicated that self-management support was not integrated or standardised throughout the RRRT.
Audit data provided by the Service Information System showed that no self-management plans were developed over a 6-month audit period (January–June 2015). Informal conversations between the project lead and six members of the RRRT over a 1-week period in June 2015 identified that, while staff reported that some self-management support takes place, it is often unrecorded and is reliant on the beliefs, knowledge and confidence of individual staff.
Staff knowledge and confidence to support service users to self-manage was measured using a 12-item questionnaire.17 The questionnaire has been used in previous quality improvement projects focusing on self-management support for service users.25 Three items address staff beliefs, one item addresses knowledge and eight items address confidence to support service users to self-manage, with a 10-item visual analogue Likert scale for responses. Baseline questionnaire data from 21 members of the RRRT (out of 35, 60% response rate) collected in June 2015 showed that, while some staff reported high levels of knowledge and confidence to support self-management, some reported low levels and on occasions no knowledge. It is possible that those reporting high levels of confidence and knowledge for supporting self-management believe that they offer self-management support to a high standard; however, this may not be the case, and investigation is warranted.
Design
A driver diagram was developed in collaboration with team members to identify factors that may influence self-management support within the RRRT and to identify key priorities for change. A self-management strategy was developed to facilitate evidence-based self-management support becoming a part of usual care delivered by the RRRT. The driver diagram identified staff behavioural change as a key factor to enabling service improvement.
The behavioural model COM-B26 guided the exploration of staff’s motivation for behavioural change. This model focuses on the capacity, opportunity and motivation of staff to make the behavioural changes needed.26 Baseline questionnaire findings indicated that the majority of staff were motivated to support service users to self-manage (80%, n=17 rated this as extremely important). The main components lacking for effective self-management support were capacity and opportunity. Deficits in knowledge and confidence were identified as a capacity barrier. The absence of standardised processes, guidance and materials designed to reduce barriers and increase the means to support self-management constituted an improvement opportunity. The intervention therefore focused on capacity and opportunity and sought to stimulate staff behavioural change so that the collaborative development of service user self-management plans and self-management support would become usual care. The intervention was multifaceted, comprising the development of a new document, staff education, audit and feedback.
Strategy
The Plan, Do, Study, Act (PDSA) model for quality improvement was used.
PDSA cycle 1 in June 2015 aimed to develop the self-management plan as part of personalised care planning, which is at the centre of the House of Care model.27 The self-management plan should reflect collaboration between staff and service users at the initial assessment meeting, with review at subsequent consultations for the duration of service users’ engagement with the team. The project manager invited all staff members and five service users to join the project group to develop the self-management plan document. The final project group comprised two service users, the project manager, the executive sponsor, the team manager, the assistant team manager, one Band 7 physiotherapist, one Band 7 and two Band 6 occupational therapists, one Band 6 registered nurse, two therapy assistants and one business support administrator.
The self-management plan document was developed drawing on the principles for personalised care planning set out by National Voices, a leading coalition of more than 150 health and social care charities28:
Plans to be developed in partnership with service users, informal carers and health and social care professionals.
People to have the right information and support to be able to manage their conditions in ways that work for them.
Plans to be holistic and consider health, well-being and life more widely than the symptoms or conditions that a person has.
Plans to be agreed by both parties and owned by the service user.
Plans to be focused on agreed goals and outcomes that are relevant to the person with an agreed action plan for achieving these and, where relevant, contingency planning for crisis episodes.
Plans to be reviewed regularly, at intervals that make sense to the individual.
The self-management plan document was developed over three 1-hour project group meetings. The service users were unable to attend the meetings due to restricted mobility so the project manager met with them in their own homes weekly on three occasions to discuss the self-management plan document content. The first version of the self-management plan document was agreed by week 3.
PDSA 2 aimed to enhance staff capacity to support self-management and to develop the two side walls of the House of Care, that is, engaged, informed patients, and healthcare professionals committed to partnership working. Two staff workshops were developed and delivered in July and August 2015:
Workshop 1 (1 day of 7 hours) focused on supporting self-management through collaborative goal setting and problem solving using an MI approach. This workshop was delivered on two occasions by a qualified MI and cognitive–behavioural therapy practitioner. All staff were invited (n=56; 25 undertook the training, 44%).
Workshop 2 (2 hours) focused on enabling staff to set and review collaborative short-term and long-term SMART goals with service users. It was delivered by a community neurorehabilitation team who had implemented a successful stroke focused self-management strategy. This workshop was attended by 36 staff (64%).
Both workshops were interactive and involved role play. Evidence shows that smaller group interactions involving role play are more likely to have a positive impact on changing behaviour29 in comparison with meetings and didactic lectures.30
The questionnaire survey was repeated after the workshops.
PDSA 3 aimed to pilot the self-management plan document with three RRRT service users at the point of initial assessment.
Pilot 1
A self-management plan was developed in collaboration with an 84-year-old service user who had recently been discharged from hospital following a fall at home. The client had bilateral leg ulcers and was below their baseline mobility. The client was receiving support three times daily from the team’s reablement care provider. During discussion, it became clear that this client’s most important goal was to regain mobility so that they could return to feeding the birds in their garden as they had done daily prior to the fall. An action plan was developed by the client, facilitated by the team worker. The client planned to mobilise the length of their lounge every day when the carers were visiting to increase their confidence and progress their mobility. A physiotherapy referral was agreed to assess if additional support was required. The self-management plan was completed, and an action plan using SMART goals was documented. An arrangement was made for a 1-week follow-up. At review, the client reported that they had found the self-management plan document useful as it contained all the important contact telephone numbers that they may need. The client reported that they had reread the goals several times during the first week and felt that this helped motivation to mobilise each day. The client also reported that they were using the self-management plan document to keep their health and social care documents all in one place, including hospital appointment letters. In response to this pilot, changes were made to improve the self-management plan document that included increasing the number of clear document pockets within the document folder to allow for the inclusion of other health and social care documents. A diary sheet was also developed to allow the service user to record and keep track of all appointments and home visits.
Pilot 2
A revised self-management plan document was taken to an initial assessment home visit with an 80-year-old service user who had recently had a total hip replacement. This client had macular degeneration and was unable to read the self-management plan. Although we were able to discuss goals and collaboratively develop an action plan, the client was unable to read any of the documentation. A large print version of the self-management plan document was therefore needed for those with a sight impairment such as macular degeneration; this is being developed.
Pilot 3
A self-management plan was developed collaboratively with a 92-year-old service user at the initial assessment following a recent discharge from hospital subsequent to a fall in which the client sustained a laceration to their arm. Prior to this hospitalisation, the client was independent. At the point of assessment, the client was receiving support twice daily from carers. The client’s long-term goal was to return to being independent with all activities of daily living. The client’s short-term goals were to make their bed daily and participate in meal preparation with support from the carers. A 1-week review was arranged. At review, the client reported that they had used the self-management plan document to contact the out-of-hours district nursing team over the weekend when their wound had started to bleed ‘quite heavily’. The client also reported that they had been unable to meet their short-term goals every day for several reasons, which they could not recall. Following this pilot, an additional page was added to the goal setting and action planning sections of the self-management plan document to allow clients to record problems and/or barriers that they had experienced in achieving their goals and to facilitate action planning and problem solving at the next review.
PDSA 4 aimed to disseminate the self-management plan document to the whole RRRT. In November 2015, the self-management plan document was available for use by all RRRT staff. Staff were advised to identify any problems encountered using the document with service users and to feedback any improvements to inform ongoing refinement. Consideration was given to the sustainability of self-management within the service. For staff members who had not attended the training, further training was organised. For those who required a refresher session, further in service training was led by members of the project group.
Results
Outcome measure
Following development of the self-management plan document and staff training, the number of self-management plans developed rose from 0 to 187 over a 4-week period (June 2015). This represented approximately 50% of referrals for that period and indicated that the aim for 90% of service users to have a personalised self-management plan within a 3-month period was achievable.
The self-management plan document was made available to all RRRT staff in November 2015, and monthly audit data of self-management plans indicate that the improvement reported in June 2015 has been sustained (November 2015: 416, 92%; December 2015: 404, 87%; January 2016: 486, 84%; February 2016: 456, 96% (figure 1).

Number of self-management plans developed with service users November 2015–February 2016.
Outcome measure
Staff knowledge about supporting service users to self-manage was scored on a scale of 1–5 (1=no knowledge to 5=expert knowledge). Pretraining, 14% (n=3) reported having no knowledge, and 29% (n=6) scored their knowledge as 2. Post-training, no one scored 1% and 8% (n=2) scored 2. Pretraining, 24% (n=5) scored their knowledge at 4 or above compared with 62% (n=15) post-training, indicating an increase in staff knowledge about self-management support following the education intervention (figure 2).
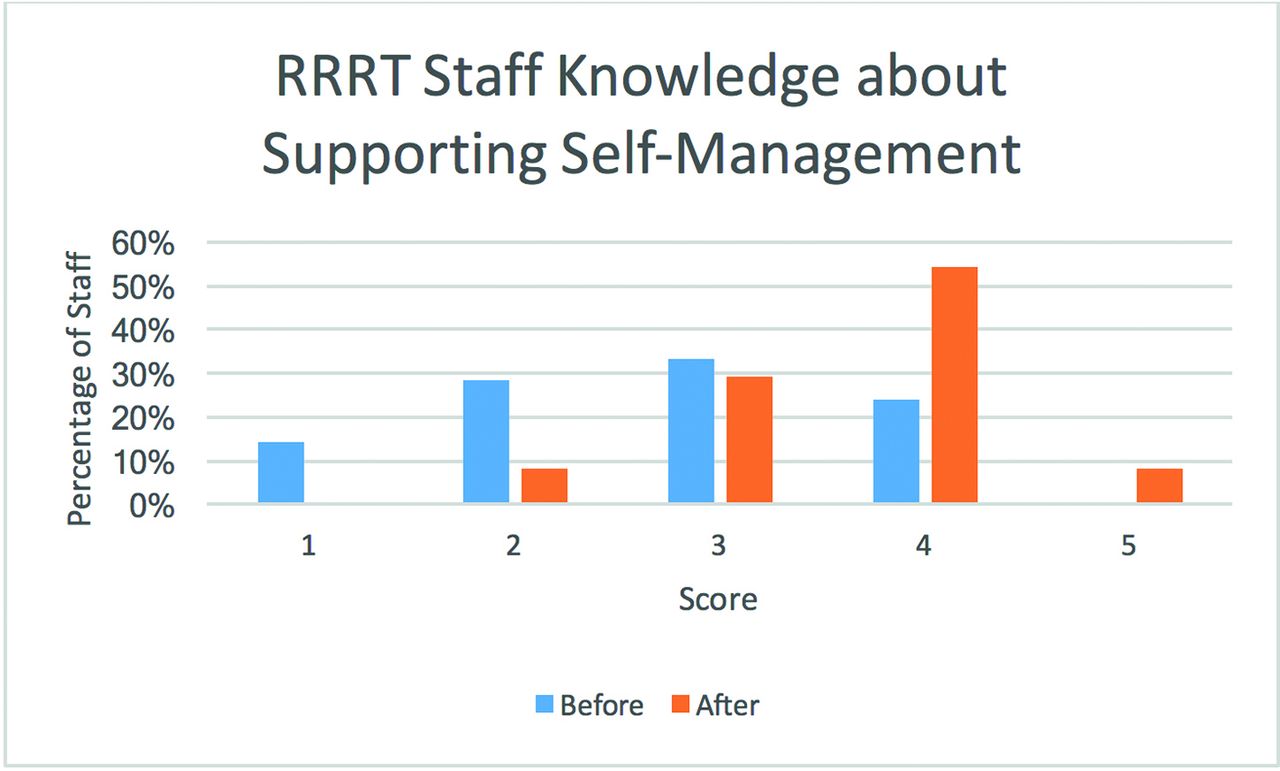
Staff knowledge about self-management pre-education and post education intervention. RRRT, Richmond Response and Rehabilitation Team.
Outcome measure
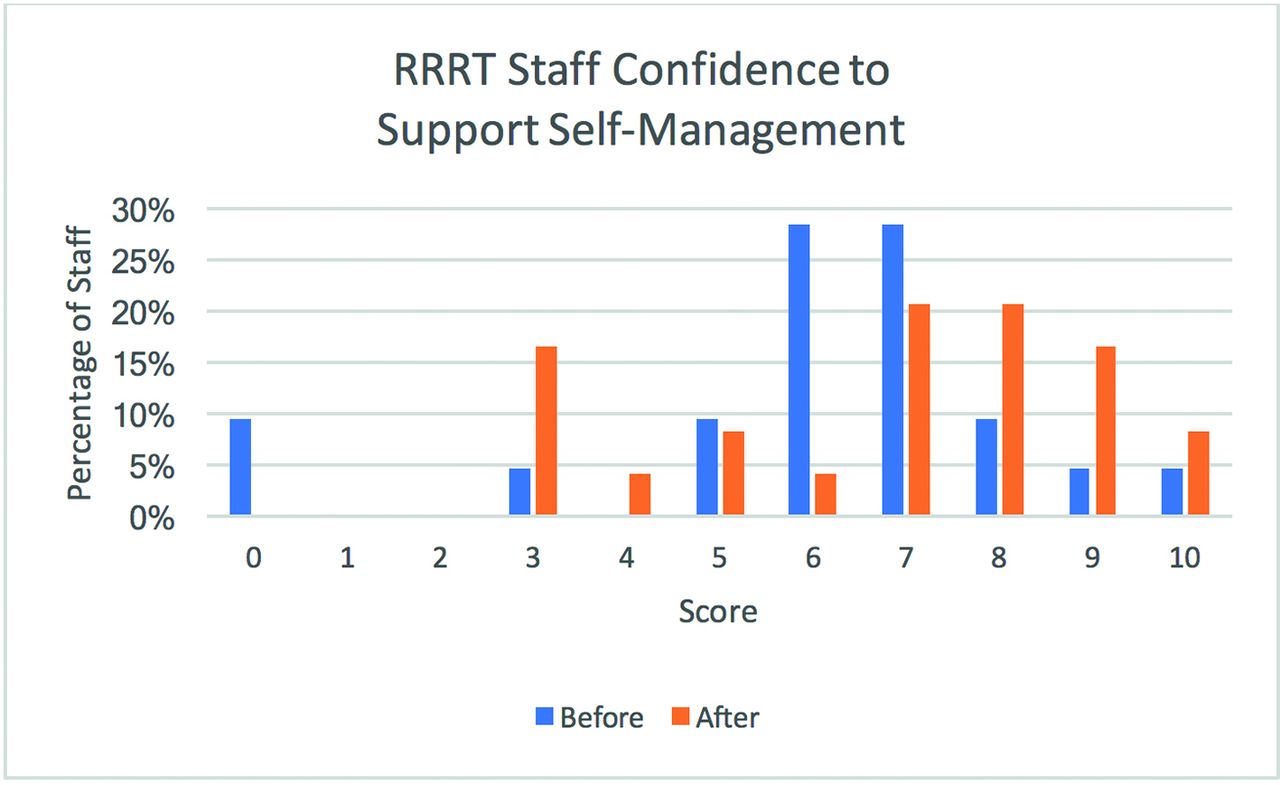
Staff confidence about supporting service users to self-manage was rated on a scale of 0–10 (0=no confidence to 10=very confident). Pretraining, two staff (10%) scored their confidence as zero. Post-training, confidence levels increased, and the lowest score was 3 (n=4, 17%). Pretraining, 49% (n=10) scored their confidence as 7 and above, which increased to 67% (n=16) as 7 and above post-training (figure 3).
{kind=link}
{kind=link}
{kind=link}
Staff confidence to support self-management pre-education and posteducation intervention. RRRT, Richmond Response and Rehabilitation Team.
Lessons, strengths and limitations
Several lessons were learnt during this project. Not all professionals engaged with the education intervention, although this does not mean that they did not support the new way of working. Some staff reported being too busy to take time out for training. A lack of engagement by some senior staff to attend training, to change their own practice and to support the new system may have undermined implementation of the self-management strategy. The project lead initially was not in a position of leadership within the RRRT when introducing a new way of working. This challenge was overcome in part by keeping the team involved throughout the project, providing regular communications about the importance and benefits of self-management and providing progress updates. Another key lesson learnt by the project lead was the importance of measuring and communicating the progress of the project and its impact for ongoing support, commissioning and sustainability. Limitations of this quality improvement project were that it had to be completed within a 6-month period and that data were not accessible beyond February 2016 due to the project lead taking up a new post in a different healthcare organisation. An attempt was also made to obtain data retrospectively for the months of September and October 2015; however, a change to how the Trust now calculates this KPI meant that a count of self-management plans developed with service users was not accessible. All data presented in this report were collected throughout the duration of the project. Strengths of this project included a committed project team with multidisciplinary representation and service users and a rigorous approach to the development and implementation of an evidence-informed self-management strategy that has the potential to be implemented by other rapid response and rehabilitation teams.
Conclusions
This quality improvement project facilitated a shared approach to self-management support through the development of a multidisciplinary project group to monitor, disseminate and share good practice; the development of a self-management plan; the implementation of an education strategy; and dissemination of the self-management plan to the RRRT. The project has generated evidence to support the feasibility of integrating self-management support into rapid response and rehabilitation models. Audit data identified an increase in the number of self-management plans being developed in collaboration with service users, rising from 0 to 187 over a 4-week period. A staff survey pretraining and post-training demonstrated an increase in staff knowledge and confidence to support service users to self-manage.
This is an ongoing quality improvement project. Measurement continues, including the number of self-management plans developed, and an audit of the quality of the self-management plan documentation including the extent of goal setting and follow-up. Service user satisfaction and hospital admission data will be accessed retrospectively and at monthly intervals to evaluate the impact of self-management plans. The staff survey will continue as a training needs analysis to inform continuing staff development. Staff training attendance data will be collected together with data on its impact. To date, 34 of the 56 staff have undertaken the training and staff numbers have recently increased from 56 to 71 so that further training is needed if self-management is to be integrated successfully into the whole team’s activities and processes. The whole team need to be trained in order to reach a shared understanding of self-management and how best it can be operationalised and sustained over time. It is recommended that self-management training is included within the induction of all new staff. A whole systems approach is needed to implement successfully self-management support, with policies and procedures including workforce planning, job plans, staff induction, appraisal and governance aligned accordingly.
The next phase of the project will include an analysis of service users’ reported barriers to self-management and will include the introduction of the Patient Activation Measure (PAM),31 which has been shown to be valid and reliable and has been used extensively globally.32 33 Patient activation is defined as: ‘an individual’s knowledge, skill and confidence for managing their health and healthcare’ (Hibbard et al, 200531, p. 332). The PAM measures a service user’s activation levels using 13 items. Service users who have a high activation level are more likely to engage in more positive health behaviours and self-manage their health conditions more effectively.34 Studies have shown that when the right service and support are in place, service user activation and health improve.34 PAM has the potential to enable tailored self-management support reflecting an individual’s activation levels, and it allows measurement of the effectiveness of interventions.
Acknowledgments
We would like to thank Professor Siobhan Gregory and Hounslow and Richmond Community Healthcare Trust for encouraging JS’s application to the Older Persons Nurse Fellowship and for their support throughout. We would also like to thank King’s College London, particularly, my supervisor Dr Jo Fitzpatrick and fellowship leads, Dr Corina Naughton and Nicky Hayes. Thanks also to Health Education England for funding the Older Persons Nurse Fellowship.
References
Footnotes
Contributors JS conceived and designed the study, with JMF contributing. JS led on data collection, analysis and interpretation of data. Both authors developed the paper and have approved the final version for publication. Both authors agree to be accountable for all aspects of the work in ensuring that questions related to accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Ethics approval This project met criteria for service evaluation and was exempt from requiring ethical approval as per the guidance for ethical clearance at King’s College London.
Provenance and peer review Not commissioned; externally peer reviewed.