Article Text

Abstract
Background Best possible medication history (BPMH) enhances the care of safety net patients, especially those with limited English proficiency and limited health literacy who are most vulnerable to medication error during the hospital admission process. Our large urban academic safety net centre faced numerous barriers to achieve BPMH among hospitalised patients including communication barriers that increase the time and complexity of eliciting BPMH, frequent provider turnover at our training institution and lack of an electronic health record (EHR) medication reconciliation tool to facilitate BPMH collection and monitoring.
Design Leveraging opportunities afforded by the US federal incentive EHR programme, our multidisciplinary team designed an EHR-facilitated medication reconciliation programme by which pharmacy technicians engaged newly admitted patients and their caregivers at the bedside to develop and electronically document the BPMH.
Strategy Prior to this intervention, pharmacy technicians had no role in BPMH. Providers collected home medications documented on paper notes without a consistent methodology. With each plan–do–study–act (PDSA) cycle since the programme began, the goal was to increase the per cent of BPMH completed by a pharmacy technician. Individual PDSA cycles targeted either the pharmacy technicians by expanding their pool of eligible patients or provider engagement with the pharmacy technician workflow.
Results By optimising not only the health information technology platform but also the operational processes, the programme achieved a nearly 80% generation of BPMH completed by a highly trained pharmacy technician, surpassing its intended goal of 50% BPMH completion by a pharmacy technician on admission.
Conclusion An EHR-facilitated tool improved BPMH at an urban academic safety net hospital using pharmacy technicians.
- medication reconciliation
- vulnerable populations
- safety net hospitals
- pharmacy technicians
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Problem
Medication reconciliation—the comparison of prescribed or recommended medication regimens with the patients’ actual medication-taking behaviour—is a challenging yet very necessary component of admission to and discharge from a hospital and crucial to patient safety. In the USA, the National Patient Safety Goals programme of the Joint Commission added medication reconciliation in 2005, and the 2009 Health Information Technology for Economic and Clinical Health Act made achieving medication reconciliation a core metric for receiving financial incentives for hospitals implementing electronic health record systems (EHRs).
Our urban academic safety net hospital recognised the challenges of implementing effective medication reconciliation with our patient population and institution (table 1). Our hospital serves a high proportion of low health literacy patients, patient populations who often have a worse understanding of their home medication regimen compared with higher health literacy patients.1 High-quality medication reconciliation with this population also requires time for appropriate patient education and teach-back and resources for language interpretation. In addition, as a training institution we have frequent turnover each month of physicians, pharmacists and nurses. Finally, our hospital is embedded within a safety net health system without a unified EHR, requiring medication reconciliation across multiple disparate EHRs and paper records.
Patient and institutional factors which make medication reconciliation more challenging
This medication reconciliation project focused on generating high-quality preadmission medication histories as this step is the foundation of the medication reconciliation process. Our goal was to generate accurate preadmission medication histories in the EHR via bedside patient engagement at the time of admission for at least 50% of patients admitted to a medical or surgical unit by incorporating highly trained pharmacy technicians as central experts in this workflow.
In the preimplementation phase, our informatics team began by optimising the existing EHR to develop a specific area to document the home medication list on admission and discharge medication list. Previously this information could only be found embedded within clinical notes. As such, before these technical changes were made, the EHR offered no specific system for monitoring compliance or quality of medication reconciliation. We then formed an interdisciplinary team including pharmacy leadership, hospital administration, clinical champions and clinical informaticists to construct a business plan that deployed pharmacy technicians to generate and enter a home medication list into the optimised EHR. To justify the resource investment, pharmacy leadership collected preliminary data that demonstrated that if providers alone were to develop medication histories, it would add significant time to existing workflows, risking delays in patient flow during the admission process or inducing providers to develop workarounds that may compromise quality. After careful review, hospital administration agreed to support this important safety work by hiring four full-time equivalents (FTEs) of experienced, multilingual pharmacy technicians to staff this programme 7 days per week for 16 hours per day.
Background
Evidence demonstrates that potential adverse drug events in hospitalised patients can be largely attributed to problems with inaccurate medication histories,2 which may be the cause of up to 85% of medication errors on admission.3 Older patients or patients on multiple medications have a higher risk of errors in preadmission medication histories, while patients who have prior recent electronic medication lists are at lower risk for error.4
The foundation of medication reconciliation during transitions through an acute care setting is the best possible medication history (BPMH), a medication history which includes a standard interview process with patients plus evaluation of one additional source of information.5 This BPMH serves as a reference for inpatient prescribing practices and the basis of any home medication modifications based on the inpatient hospitalisation at the time of discharge. The BPMH is difficult to obtain for multiple reasons6 7 :
poor patient understanding of the home medication regimen (worse in low literacy or vulnerable populations)
lack of experience or expertise by junior providers in eliciting a medication history
inadequate or fragmented health information systems
errors in history taking
time-consuming nature of the process
competing clinical responsibilities.
While quality data showing clear improvement in patient safety or clinical outcomes as a result of medication reconciliation interventions are lacking,8 9 some evidence suggests that medication reconciliation interventions may be worthwhile, especially those involving pharmacy or targeting high-risk groups.10 Recent data suggest that pharmacy-driven medication reconciliation programmes may improve rates of readmissions and emergency department visits.11 Therefore, we felt that the generation of an electronic BPMH as part of medication reconciliation could be a particularly meaningful target for quality improvement work.
Measurement
The rate of BPMH generation by pharmacy technicians across hospitalised patients was the primary outcome for this intervention. Prior to this intervention, pharmacy technicians did not participate in developing the BPMH on admission as this task was assumed to be the responsibility of the admitting provider. Provider compliance with BPMH generation using standard practices was estimated to be greater than zero but likely substantially less than the target 50% we hoped to achieve using pharmacy technicians. Baseline compliance could not be systematically measured as medication histories prior to this intervention were only found embedded into handwritten clinical notes and did not typically cite the process or sources by which such information was gathered by the provider.
Baseline data prior to launch of the programme showed that a user trained in the optimised EHR medication reconciliation pathway needed 1–2 min per medication to enter the home medication list in the EHR, not including the time to verify and actually develop the list. Estimates using an average of 8 medications for a patient admitted to a medical or surgical unit and 40 admissions per day meant 11 additional hours per day of work on data entry alone. These data informed the number of pharmacy technician FTE that would be required to achieve the goal of 50% BPMH generation on admission.
Our main outcome of interest was percentage of total admissions for which a BPMH was generated by a pharmacy technician; each plan–do–study–act (PDSA) cycle aimed to improve this specific outcome only.
We also collected process outcomes and descriptive characteristics of patient sociodemographic and medication profile characteristics to further explore the resources needed and benefits of this intervention. These measures included total amount of time to generate and enter BPMH in the EHR; percentage of BPMH completed by a pharmacy technician prior to a provider entering admission orders; number of medications taken by each patient; number of discrepancies between a patient’s prescribed list or pharmacy profile and patient-reported medication-taking behaviours and number of patients on high-alert medications (anticoagulants, insulin, methadone and chronic opiates of 50 mg morphine equivalents or more).
Each time a pharmacy technician began a BPMH, she/he entered the patient information and the data described above into a secure database. This method allowed pharmacy technicians to better track these specific measures.
Design
Our team designed this intervention to focus on developing a multidisciplinary approach to generating the BPMH, centred on pharmacy technicians collaborating with staff pharmacists, patients and caregivers, inpatient and outpatient providers, community pharmacies, skilled nursing facilities, jails and other partners. We chose pharmacy technicians as the central resource because they are licensed specialists with in-depth knowledge of medications and training in customer service and interdisciplinary collaboration. They serve as a cost-effective, natural link between patients and providers.
Our final protocol for developing the BPMH by the pharmacy technician followed four key steps (figure 1): patient identification, patient interview, list generation and communication with the healthcare team.

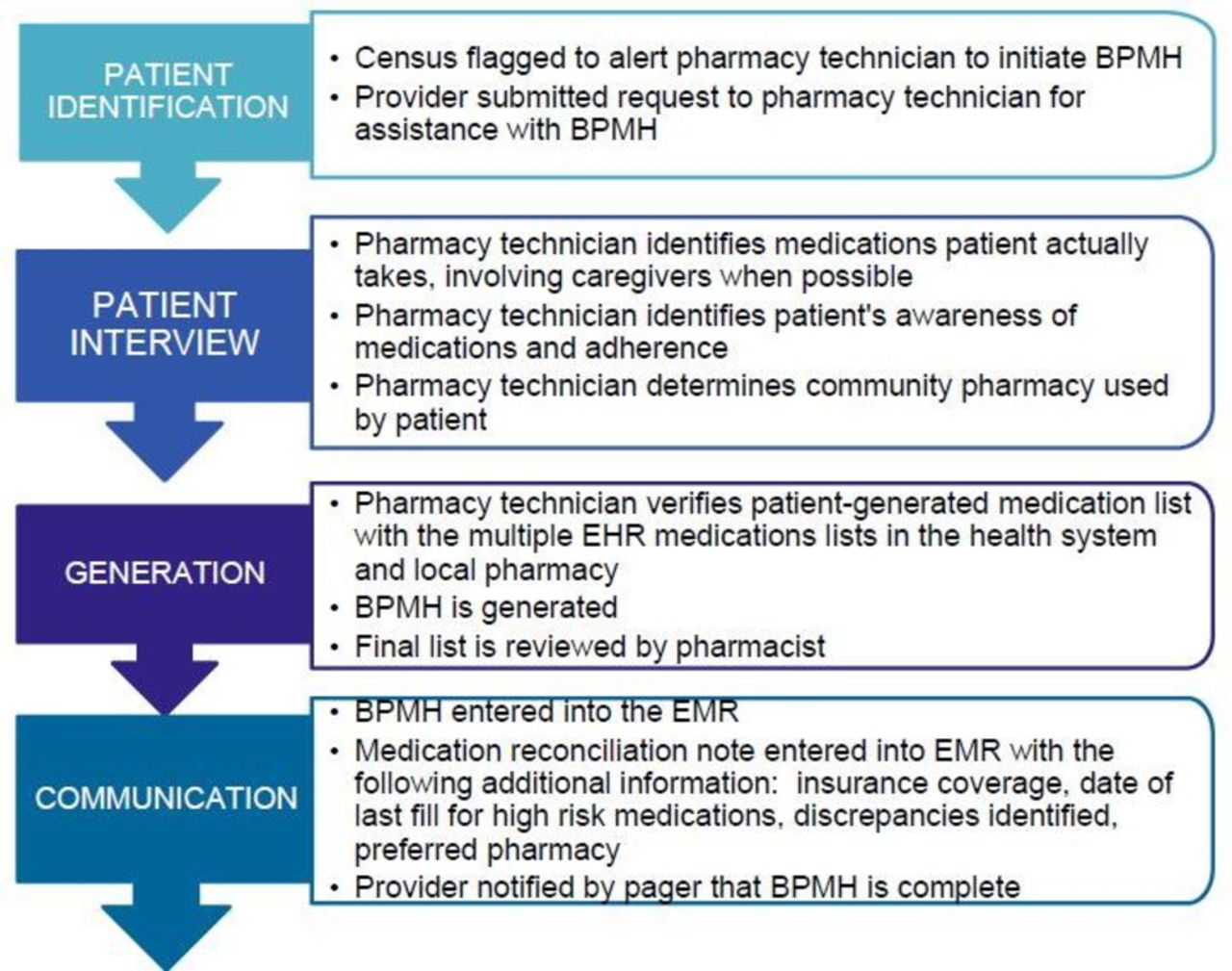{kind=link}
Final best possible medication history (BPMH) protocol design after multiple plan–do–study–act at an academic urban safety net hospital. EHR, electronic health record.
Strategy
PDSA cycle 0: educational intervention around medication reconciliation
We aimed to generate a safety culture supportive of medication reconciliation by raising awareness of the institutional commitment to medication reconciliation and prepare clinicians for workflow and technical changes. Pharmacy and clinical champions provided training to clinical divisional informatics leaders and trainees that consisted of two parts: (1) education regarding general principles behind medication reconciliation and (2) technical training around the new electronic medication reconciliation tool and pharmacy technician programme.
PDSA cycle 1: piloting BPMH generation on patients admitted through the emergency department
Pharmacy technicians generated BPMH for patients who were admitted through the emergency department and documented their findings in a paper note, reviewed by a staff pharmacist and placed in the bedside chart. Pharmacy technicians identified patients appropriate for BPMH by monitoring the emergency department admissions list.
(This initial paper version of the note included a list of medications that the patient was actually taking, the sources of information (eg, community pharmacy, patient, family/caregiver, clinical notes, outpatient EHR) and discrepancies describing how patients were taking medications differently from prescriber instructions or not at all.)
PDSA cycle 2: expansion of BPMH programme to include non-emergency department admissions
Since up to 30% of hospital admissions may be directly admitted from areas outside the emergency department, we expanded the programme to include direct admissions from outpatient providers, transfers from other hospitals and admissions from the Post Anesthesia Care Unit after surgery. Pharmacy technicians in this cycle were given access to other work lists to identify all patients admitted outside the emergency department pathway.
PDSA cycle 3: prioritising the limited resource of pharmacy technicians performing medication reconciliation
Because of staffing fluctuations, BPMH by pharmacy technicians was not available for all eligible admissions in cycle 2, and so we needed a mechanism for providers to identify high-risk patients for whom home medication reviews would be most beneficial. We hypothesised that if providers were more engaged with the pharmacy technicians in the workflow process that a greater percentage of BPMH could be completed by a pharmacy technician. Thus, the informatics team developed a feature within the EHR tool for any clinician to provide clinical information prioritising patients for medication review. This information was transmitted via pager to the pharmacy technician on duty who added this patient’s information to the top of the work queue.
PDSA cycle 4: conversion to electronic documentation in order to increase visibility of information captured
Clinical care teams provided positive feedback about the value of the information gathered by pharmacy technicians but lamented its lack of accessibility due to location in the physical chart. Given the frequent turnover of trainee providers, we needed an additional mechanism to remind trainees about the pharmacy technician BPMH programme and felt that an electronic note would increase programme visibility and encourage use of the prioritisation tool described in cycle 3, ultimately increasing per cent BPMH performed by pharmacy technicians. Therefore, we changed the BMPH note to an electronic form that coexists with inpatient and outpatient clinician notes.
(In this EHR BMPH note, pharmacy technicians noted additional information, including dates of last prescription fills, the patient’s preferred community pharmacy, prescription drug coverage and patient’s reported medication knowledge and adherence.)
Results
PDSA cycle 0 spanned approximately 3 months. PDSA cycles 1–4 spanned a total of 15-month period, with 3–5 months for each cycle. During the 15-month period, there were a total of 13 116 admissions, of which 77% had a BPMH documented in the EHR by a pharmacy technician during the hospitalisation. With each PDSA cycle, enhancements broadened the programme’s reach and increased clinician engagement by making information more accessible. The percentage of BPMH completed by a pharmacy technician increased from 64% in PDSA cycle 1% to 79% by PDSA cycle 4. The time required to complete each BPMH did not change significantly between cycles (average 23 min).
On average, patients reported taking 5.1 medications. Pharmacy technicians elicited an average of 1.4 discrepancies between a patient’s prescribed list or pharmacy profile and their reported medication-taking behaviours, including non-adherence. Seventeen per cent of patients were documented as taking a high-alert medication. These patient characteristics did not vary substantially between PDSA cycles.
Lessons and limitations
Although we reached high rates of BPMH completion overall, pharmacy technicians could complete BPMH prior to provider placement of admission orders for 21% of admissions (monthly range 10%–40%). Although we intended BPMH to enhance medication safety and accuracy during the admission prescribing process, pharmacy technician staffing fluctuations in combination with a consistently high number of admissions during the narrow window between the decision to admit and the placement of admission orders compromised this goal.
Since medication reconciliation is a required part of all hospitalisations to a medical or surgical unit, providers developed BPMH when pharmacy technicians were not available, including when patients were discharged prior to BPMH generation by a pharmacy technician, when volume of admissions was high during a technician’s shift or if patients or caregivers declined to talk with the pharmacy technicians. If patients were unable to participate in BPMH due to cognitive impairment or severity of their medical condition, pharmacy technicians evaluated these patients and documented as such, thereby signalling providers to complete this assessment once the patient’s condition improved. As described in PDSA cycle 3, providers could also contact a pharmacy technician on duty to re-evaluate patients once they were able to participate in an interview later in the hospitalisation.
Future studies should assess the quality of BPMH performed by a pharmacy technician versus a provider; the impact of pharmacy technician BPMH on medication errors post-hospitalisation and hospital readmission; and the cost-effectiveness of pharmacy technician BPMH programmes.
Conclusion
Medication reconciliation tools are common features of modern EHRs. However, due to the provider and patient challenges posed at our institution, simply implementing an EHR tool might not lead to meaningful execution of medication reconciliation. Thus, we worked to optimise both our EHR tools and operationalise a programme to embed BPMH into the admission workflow using pharmacy technicians. We also provided education to clinicians not only on the EHR tool but on the rationale and strategies for effective medication reconciliation, emphasising the culture of medication safety as an institutional priority. With each performance cycle, enhancements were associated with increases in the percentage of patients with BPMH performed by a pharmacy technician during the hospitalisation. Early cycles expanded the reach of the pharmacy technicians to the appropriate admitted patients, and later cycles aimed to expand provider knowledge and engagement with pharmacy technicians to prioritise specific BPMH. All cycles aimed to and successfully increased the percentage of BPMH completed by a pharmacy technician. Programme successes are due to: early engagement of stakeholders for fiscal support; a critical evaluation of admissions processes aiming to optimise each team member’s workflow to enhance patient flow; consistent engagement of both patients and their community caregivers to improve the accuracy of medication reconciliation and matching clinical responsibilities to team members’ training to improve patient care. Because of these factors, we were able to greatly surpass our goal of 50% BPMH performed by a highly trained pharmacy technician.
Acknowledgments
The authors thank the Zuckerberg San Francisco General Hospital/San Francisco Health Network Executive Leadership, Zuckerberg San Francisco General Informatics and Zuckerberg San Francisco General Pharmacy Department for all their important contributions to the successful launch of this project. The authors would especially like to thank the team of dedicated pharmacy technicians who carry out this work each day, specifically Katrina Alban, Joel Hallare, Antonio Hoy, Dang Lam, Kimberly Lin, Melisa Palacios, Chaune Pierre-Harris, Loida Roguel, Renee Sandoval, Jason Sison and Tracy Zhou. They also thank the Open Access Publishing Fund at the University of California San Francisco for their support.
Footnotes
Contributors SS was responsible for the literature review, data analysis and manuscript writing. DES was responsible for the literature review, project design, project implementation, data monitoring and analysis, and manuscript writing. SG was responsible for the project design, project implementation and manuscript writing. NR was responsible for the data analysis and manuscript writing.
Funding Research reported in this publication was supported by AHRQ Grants 1K08HS022561 and P30HS023558 and the National Center for Advancing Translational Sciences of the NIH under Award Number KL2TR000143.
Disclaimer The funding sources had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript; and decision to submit the manuscript for publication. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of AHRQ or the NIH.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.