Article Text

Abstract
Summoning is a key component of communication between obstetrics and neonatal resuscitation team (NRT) in advance of deliveries. A paging system is a commonly used summoning tool. The timeliness and information contained in the page help NRT to optimally prepare for postdelivery infant care. Our aim was to increase the frequency that summoning pages contained gestational age and reason for NRT attendance to >90%. At baseline, 8% of pages contained gestational age and 33% of pages contained a reason for NRT attendance. Sequential Plan-Do-Study-Act cycles were used as our model for quality improvement. During the 8-month improvement period, the per cent of pages increased to 97% for gestational age and 97% for reason for NRT attendance. Measures of page timeliness, our balancing measure, did not change. Summoning communication between obstetric and NRT is crucial for optimal perinatal outcomes. The active involvement of all stakeholders throughout the project resulted in the development of a standardised paging tool and a more informative paging process, which is a key communication tool used in many centres.
- communication
- paging
- neonatal
- obstetrics
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Problem
In March of 2012, obstetric practice at our institution moved to the newly opened Texas Children’s Hospital Pavilion for Women (PFW) Houston, Texas, from an adjacent delivery hospital. Prior to this transition, the labour and delivery (LD) personnel sent a team page to the neonatal resuscitation team (NRT) via a paging operator to summon the team for a delivery. The pages relayed location of the delivery and a predefined set of information items using a paging tool. NRT and LD were generally satisfied with this system and the desired information was usually transmitted.
There were several issues with the system after moving to the new hospital location. The NRT noticed a decline in per cent of pages with gestational age and reason.
NRT worked with our Golden Hour Team, an interprofessional and multidisciplinary group focused on care of babies in the delivery room, to address this concern. Our hypothesis was that newly hired staff unfamiliar with the paging system, which did not change with the transition to PFW, may have reduced the effectiveness of the prior system.
Our aim (key measure) was to increase the frequency that summoning pages contained gestational age and primary reason NRT was needed to >90%. Our balancing measures were per cent of deliveries where the NRT page was received before birth and time interval between NRT page receipt and delivery of baby. These were chosen to ensure that any improvement in information sharing in the pages was not detrimental to timely arrival to deliveries.
Background
Healthcare error is the third leading cause of death in the USA,1 and communication errors are often the root cause.2–4 According to the Joint Commission, ineffective communication contributed to 72% of obstetric sentinel events resulting in perinatal mortality or permanent disability.5 Coordinating activities with other units like the neonatal intensive care unit was the most frequent communication barrier in a study of LD providers.6 Given the increasing complexity of the current healthcare environment, communicating effectively within and between teams has never been more important.
Summoning is a key component of communication between obstetrics and NRT in advance of high risk deliveries, which has unique challenges.7 The Neonatal Resuscitation Program recommends communication of expected gestational age, amniotic fluid colour, number of babies expected and any additional risk factors,8 but does not address the timing or vehicle for delivery of this critically important information. A paging system is a commonly used summoning tool and the primary method used at our institution. The timeliness and information contained in the page (gestational age and reason for NRT attendance) help NRT to optimally prepare for postdelivery infant care.
Little data exist on how to optimally summon NRT to deliveries. In one survey, 44% of individuals reported use pages or text messages to summon NRT to deliveries at their institution.9 In the same survey, individuals in institutions with a standardised script for communication, such as the paging tool described here, were more satisfied with the level of communication.9 Another study reports improvement on frequency of five critical information items communicated from LD to NRT when changing from verbal-based communication to computer-based text/page system.10 Therefore, a paging tool such as the one we describe might improve communication of critical information items and user satisfaction at other institutions.
Baseline measurement
The Golden Hour Team had previously developed a checklist for NRT to use to prepare for every attended delivery and collects data on quality measures of delivery room care. These data are stored in a database for quality improvement and safety monitoring. Prior audits have demonstrated a >90% collection rate and use of the checklist by NRT for attended deliveries.
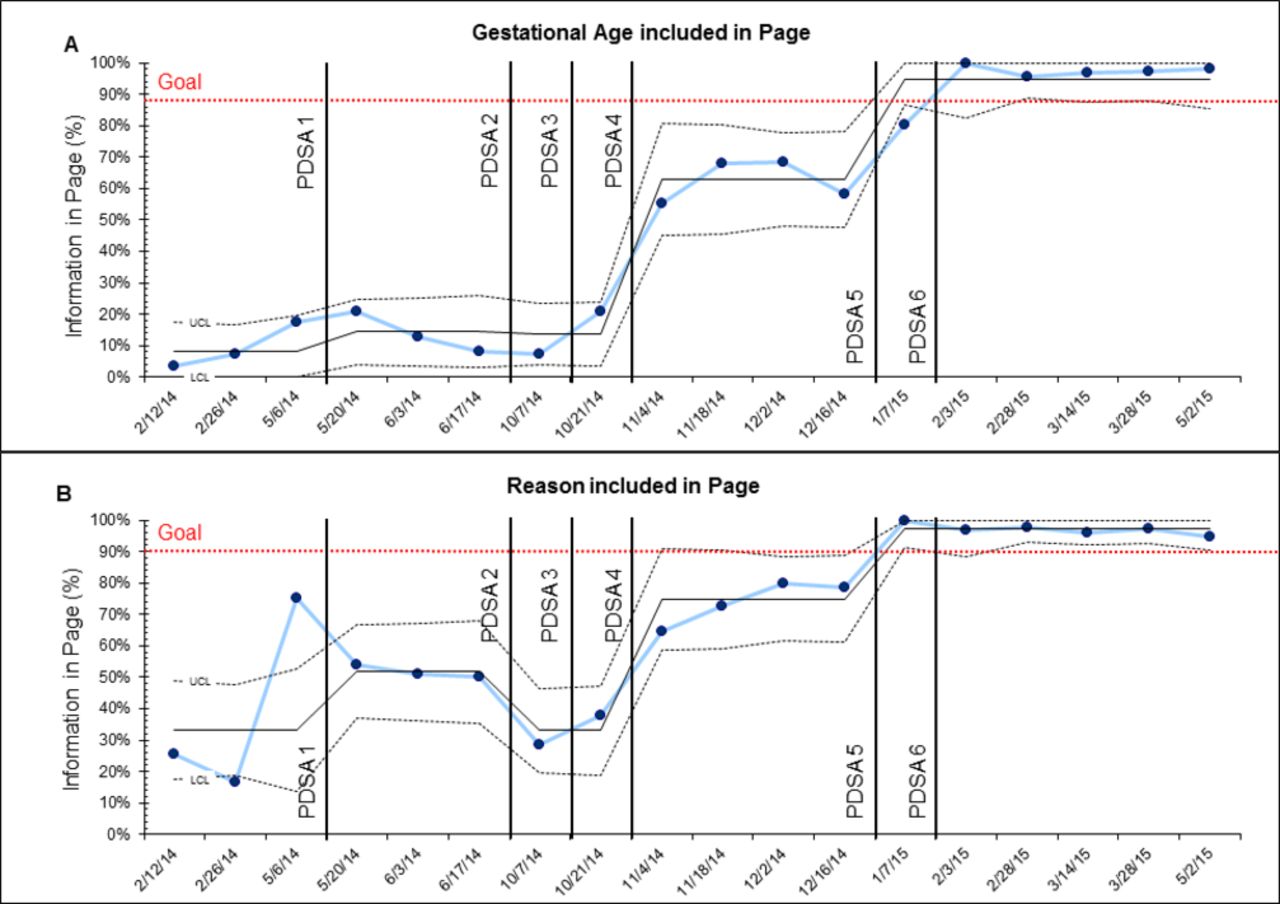
Members of NRT generally agreed that a high percentage of pages included gestational age and reason for NRT attendance, but had slowly declined in frequency since transitioning to PFW. But our database did not record these data and no prior data on these measures were available. In February of 2014, we obtained prospectively all the transcripts for pages to NRT in 2-week blocks. This analysis revealed that 8% contained gestational age and 33% contained the reason NRT was needed at delivery (n=229). Subsequent paging transcripts of 2-week intervals were obtained and analysed periodically. In May 2014, the percentage of pages containing gestational age was 17% and reason for NRT attendance was 75% (figure 1).
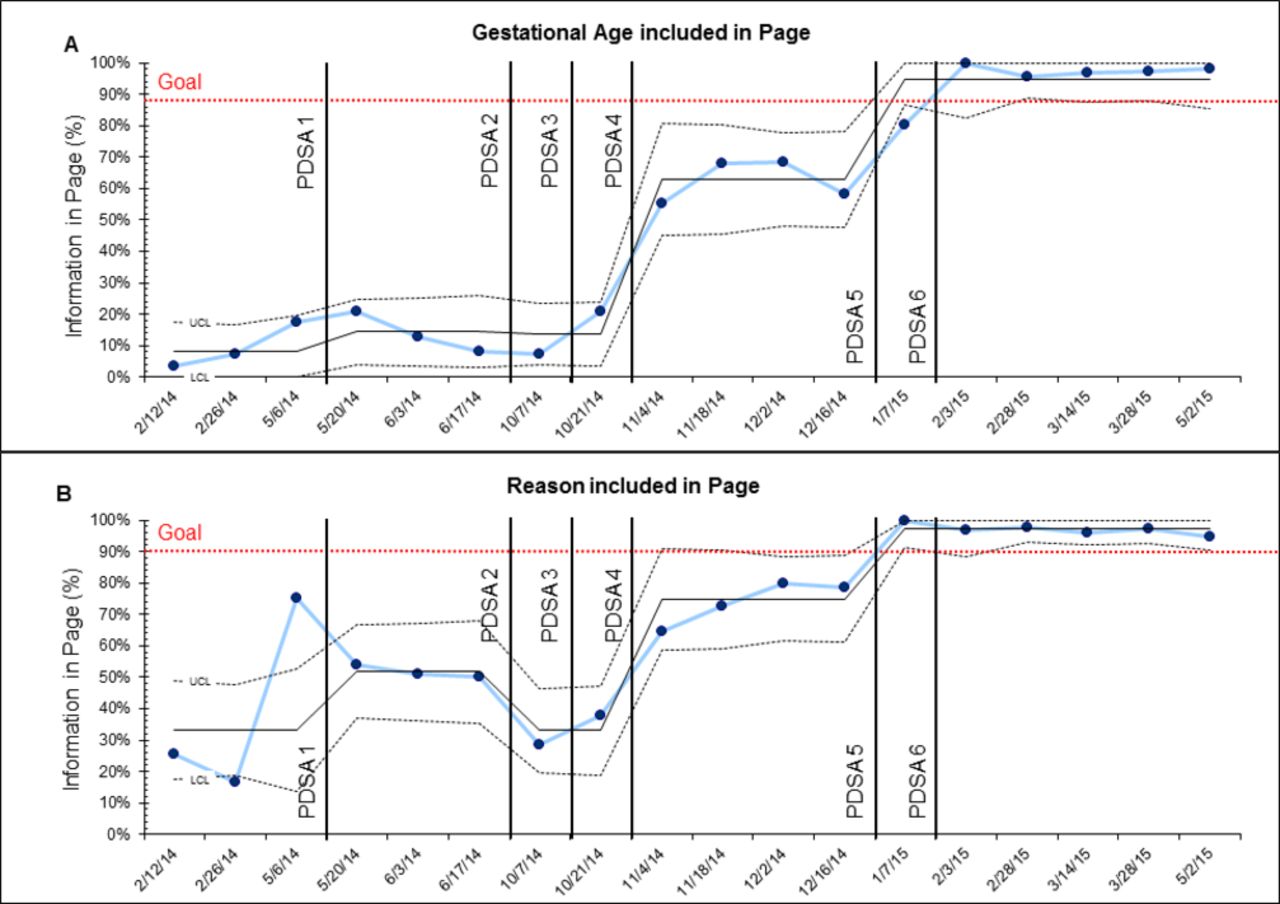
Information received from pages improved to our goal of >90%. All pages for NRT were included in transcripts analysed. Pages were excluded if they were test pages, non-urgent transfer requests or for locations outside the routine delivery areas of the hospital. Data were grouped into 2-week intervals (range of n, 32–135) and displayed in a P chart for (A) gestational age and (B) reason for NRT. The horizontal dashed, red line represents our smart aim goal. Vertical lines represent the start of each PDSA cycle. NRT, neonatal resuscitation team; PDSA, Plan-Do-Study-Act.
The balancing measures were routinely recorded in our database since March of 2012. The data include all deliveries of babies NRT was paged, which would include babies already born and in the newborn nursery. Data were excluded if page time was >10 min after delivery as this was assumed to not be a delivery room issue. Local guidelines (neonatal triggers) define the high-risk deliveries that NRT should be present at, but LD staff are encouraged to page NRT for concerns about delivery even if not listed in the guidelines. The baseline per cent of pages received before birth was 88.6% and the mean time between receiving the page and birth was 11.5 min (n=2640).
Design
The Golden Hour Team made revisions to the existing paging tool (online supplementary figure 1A) in May 2014 to encourage inclusion of gestational age and reason for NRT attendance and updated for use in PFW. The Golden Hour Team met with LD nursing leadership and key clinical stakeholders to gain support and buy-in for reintroduction of the paging tool to LD.
Supplementary file 1
The method for summoning NRT at baseline consisted of the following steps:
The LD primary nurse called the paging operator at a number designated for NRT.
The LD nurse provided the operator with delivery location and any other information felt necessary.
The page operators freely typed the message in no consistent format containing the information they were given and sent the page to NRT.
NRT received the page as text messages on mobile phones and alpha numeric pagers.
The team focused on the second step as a way to standardise what information LD communicates to the paging operator. A later Plan-Do-Study-Act (PDSA) cycle addressed the third step by standardising the message format and information sent by the paging operators to NRT.
Strategy
The Golden Hour Team reintroduced the paging tool and re-educated all parties involved on its use. We used PDSA as our model for quality improvement. Box lists and defines the PDSA cycles sequentially that were used in our quality improvement project.
Plan-Do-Study-Act (PDSA) cycles
Aim: To improve the percentage of pages summoning NRT to a delivery containing the gestational age and the reason for NRT presence.
PDSA 1 intervention: introduced paging tool and changed caller from primary LD nurse to LD unit coordinator (7 May 2014–17 June 2014).
We revised the previous paging tool (online supplementary figure 1A) and reintroduced it to the PFW LD team. The revised paging tool was provided to the paging operators as well. We reminded the LD nursing staff about the tool at morning meetings and through personal contact during the work day. LD nursing leaders also asked that LD unit coordinator become responsible for calling the paging operator using the tool to transmit the information.
PDSA 2 intervention: decreased number of options for reason NRT was needed and changed back to primary LD nurse as caller (19 June 2014–7 October 2014).
LD staff were receptive to the paging algorithm, and feedback indicated the paging tool was easy to use. LD staff recommended the indications be streamlined. We, therefore, decreased the number of reasons to summon NRT from 20 to 9. Indications not eliminated focused on diagnoses requiring a specific resuscitation approach in the delivery room (eg, meconium presence). LD nursing leaders determined the primary LD nurse should summon NRT instead of the unit coordinator as this person was most familiar with the LD patient.
PDSA 3 intervention: paging operators trained and encouraged to prompt LD caller for missing paging tool information (8 October 2014–21 October 2014).
The paging operators were given and trained on the revised paging algorithm. We worked directly with the paging operators and their director to prompt the LD staff for the information on the paging tool, but ultimately they were to include whatever information they received without delaying the summoning page. The director of the PFW paging operator team joined the Golden Hour Team to better understand the problem.
PDSA 4 intervention: LD nurse leader took over education of LD staff about paging tool and decreased number of reasons further (22 October 2014–16 December 2014).
An LD nurse leader (MLM) was invited to join the Golden Hour Team and took over education about the paging tool for LD staff and encouraged its use. The paging algorithm criteria were further reduced from 9 to 5 reasons for summoning the NRT response team to streamline the paging process (online supplementary figure 1B).
PDSA 5 intervention: paging tool developed into a drop-down list in the paging system used by the paging operators (17 December 2014 to end).
We codified the paging algorithm in a computer program developed by the paging operator director. The computer program listed the criteria that the summoning page to NRT should contain. This technological cognitive aid for the paging operators assisted prompting the LD staff for information and reduced the time needed to type in the information provided by LD. It also put the text page into a consistent format and order of location, gestational age and reason NRT was needed.
PDSA 6 intervention: badge tags made of final paging tool and distributed to LD (13 January 2015 to end).
Based on additional LD feedback, a final revision of the paging algorithm reinstated several summoning criteria previously removed as they were the most common reasons NRT was paged to a delivery. This final paging algorithm was made into a badge tag (online supplementary figure 1C), and distributed to the LD team for use as another cognitive aid.
LD, labour and delivery; NRT, neonatology resuscitation team; PFW, Pavilion for Women;.
A P chart was used to display the percentage of pages with gestational age or reason for page tracked in biweekly intervals. A P chart was used to display the monthly percentage of deliveries for which NRT was paged before birth. The χ2 test was used to compare the proportion of deliveries for which NRT was paged before birth. An X-bar chart and an S chart were used to display the monthly mean and SD, respectively, of the time between paging NRT and delivery.
Results
PDSA cycles 1 and 2, although well intentioned, resulted in decreased information shared in the summoning page, reaching a nadir in October 2014 of 7% for gestational age and 29% with a reason for NRT attendance. However, PDSA cycles 3–6 had improved percentage of pages with gestational age and reason for NRT attendance included. By February 2015, >90% of pages contained gestational age and a reason for the page, and improvement was sustained for the next 3 months.
The rate of pages received before birth was tracked and did not change (mean 89.2% compared with baseline mean 88.6%, P=0.86; figure 2). An overall trend to decreased time between receiving the page and birth of the baby was noted but did not reach significance (mean time 10.0 min vs 11.5 min at baseline, P=0.09, figure 3A). An S chart of the data revealed an increase in variability in the interval time from page received to birth after the introduction of the paging tool.

No decrease in timeliness of pages during our quality improvement (QI) work. All deliveries attended by NRT have time page received and birth time recorded in our Golden Hour Team database. Page was counted as received before birth if the page-received time was before birth time. Deliveries were excluded where NRT received a page 10 min or greater after birth time as it was presumed that these did not represent delivery room management related to birth resuscitation. Paging tool refers to the QI work reported here and all data before are baseline data. Data displayed in a P chart. There was no change to this balancing measure (mean 88.6% vs 89.2%, n=2640 vs 1982, baseline vs paging tool, P=0.86). NRT, neonatal resuscitation team.

{kind=link}
{kind=link}
{kind=link}
Trend in decreased amount of time for NRT to prepare. All deliveries attended by NRT have time page received and birth time recorded in our Golden Hour Team database. The difference in these times was the time interval. Pages received shortly after birth had a negative time interval. Deliveries were excluded where NRT received a page 10 min or greater after birth time as it was presumed that these did not represent delivery room management related to birth resuscitation. Paging tool refers to the QI work reported here and all data before are baseline data. Data are displayed as (A) an X-bar chart of the mean time interval and (B) an S chart of the SD of the time interval. There was a trend towards decreased time interval, but it was not significant (mean 11.5 min vs 10 min, n=2640 vs 1965, baseline vs paging tool, P=0.09). NRT, neonatal resuscitation team.
Lessons and limitations
Our primary lesson is that improvements affecting multiple teams and disciplines must involve all parties in the quality improvement process. Initially, the Golden Hour Team was composed of primarily neonatology stakeholders. Our initial efforts to improve the information received in pages (PDSA cycles 1–2) had a negative effect on the per cent of pages with the information we wanted. The first real improvement occurred after an LD nurse manager (MLM) was added to our Golden Hour Team (PDSA cycle 4). Her perspective and relationships within the LD unit strengthened the promotion of the paging tools use to her staff. Additional improvement occurred after the director of the paging operators developed a standardised computer-based method for including the information on the paging tool into the pages sent to NRT (PDSA cycle 5). His contribution was the fruit of him joining our team discussions and understanding the need. We feel that without these additional stakeholders added to our team, we would have never reached our goal.
The second major lesson was on choosing a system within the control of the improvement team. In June of 2015, a hospital-wide standardisation of all summoning pages for all units resulted in the inclusion of only location and no other information. Despite our success, we were unable to use our system to show sustained improvement beyond 3 months past PDSA cycle 6. It should be a consideration when choosing a project if the system you are trying to improve is likely to be in use long enough to be worth the effort.
Our balancing measures were chosen to ensure that use of the paging tool did not increase the time it took to communicate the information from the LD to the operator and subsequently decrease the timely arrival of NRT to deliveries. There was no change in per cent of pages received before delivery. Ideally, NRT would arrive before 100% of deliveries for which they are needed. NRT, however, also responds to deliveries with no fetal or maternal risk factors after which infants are unexpectedly depressed, and to care of infants with respiratory distress or hypoglycaemia appearing after the initial birth stabilisation. A limitation of our study is that indication of attendance of NRT is not included in our database.
We found a decrease in time between page and birth (figure 3A) with our improvement work. This may reflect an increase in the time needed to answer operator questions and for the page to be sent. However, the ideal time of arrival before birth is unknown and may vary by indication for delivery. The NRT team has requested to be present about 10 min before a birth or by the time of the ‘time out’ in cases of surgical delivery. Obviously this is a difficult target to predict and the data reflect some wide variability in that timing. So even though the interval time decreased, it was still with the requested time frame of 10 min. Of more interest to us was the change in SD over the period of our improvement work (S chart, figure 3B). The work to reintroduce the paging tool coincided with an increase in variability. We expect that, if this was indeed caused by our paging tool, this would have decreased again over time as familiarity with the process continued.
Conclusion
Communication between obstetric and neonatal teams around a high-risk delivery is crucial for good outcomes for the mother and the baby. We report here of an improvement project aimed at one component of the communication, summoning. Although initial PDSA cycles did not result in improved information sharing, active involvement of all stakeholders in an improvement team was key to eventual success. LD personnel championed this project, resulting in >90% compliance with the paging tool in subsequent months. The improvement was cut short by an unexpected hospital system change.
Acknowledgments
The authors wish to acknowledge the help of George Miller, whose role as director of paging operators was critical to our work’s success. He designed the computer algorithm using our paging tool that the paging operators used in the final PDSA cycles.
Footnotes
Contributors NCS conceptualised and designed the study, collected data, carried out the initial analyses, drafted the initial manuscript, and reviewed and revised the manuscript. FCK carried out additional analyses, helped draft the initial manuscript, and reviewed and revised the manuscript. EMW, MLM, MCB, JOG and BEL defined the PDSA cycles and were integral to implementation of interventions and collection of the data. JLH helped design the data collection database, made all the statistical analyses of the data and helped draft the manuscript. GG and RMF critically reviewed and revised the manuscript. All authors reviewed and approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.