Article Text

Abstract
Objectives Acute kidney injury (AKI) is common in hospitalised patients, often mandates changes to regular medications and can be unresolved at hospital discharge. General practitioners (GPs) require apposite AKI-related information in electronic discharge letters (EDLs). In 2015 NHS England introduced a care quality standard that all EDLs should include four items of information for patients with AKI. We performed a 12-month quality improvement project (QIP) aimed at achieving above 90% compliance with the quality standard.
Methods Hospital-wide episodes of AKI were detected using the nationally approved electronic AKI alerts system. 25 patient AKI episodes were audited per month for 12 months using the electronic patient record. The target compliance rate was staggered at 35%, 65% and 90% for each subsequent 3-month block. Baseline compliance was 22%. Measures taken to improve compliance included email information, grand rounds, ward-level meetings, computer screensavers, nurse support, clinical governance meetings, and face-to-face rapid education. Annotation of AKI within the computer EDL system was progressively enhanced such that in the final quarter the presence of an AKI-alert mandated the user to complete the AKI annotation before the EDL could be signed off.
Results The completion rate improved to 37% in the second quarter, 51% in the third quarter and 92% in the fourth quarter. This change has been sustained in the 14 months since.
Conclusions By the end of the study, omissions relating to AKI information were reduced from 78% to less than 10%, indicating our QIP was highly effective—meeting the quality standard. The single most important factor in improving documentation was to mandate user review of AKI aftercare in patients with electronic AKI alerts. Our study encompassed hospital-wide inpatients, and our results could be replicated at other acute hospitals that have implemented an EDL system connected to an AKI alert system.
- acute kidney injury
- quality improvement
- electronic discharge letter
- commissioning for quality and innovation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- acute kidney injury
- quality improvement
- electronic discharge letter
- commissioning for quality and innovation
Problem
The hospital discharge letter is critical to ensuring a safe transition from hospital to community care, but the quality of information provided is often found to be inadequate.1–3 Acute kidney injury (AKI) is common in hospitalised patients and requires longitudinal monitoring by general practitioners (GPs), particularly because of the risk of developing chronic kidney disease and its associated morbidity.4 AKI-related aftercare information may be missing from electronic discharge letters (EDLs) because the importance of AKI is not recognised by the clinician writing the EDL, or the AKI resolved earlier during the admission and was later overlooked. To improve the quality of AKI information in EDLs, NHS England introduced a quality standard for AKI reporting as part of the Commissioning for Quality and Innovation (CQUIN) payment reward system.5 As part of the NHS England contract hospitals could negotiate remuneration based on excellence in achieving the CQUIN quality standard. In 2015, the quality standard for AKI mandated the inclusion of four items of information in EDLs for patients with AKI. These items included stage of AKI, evidence of medicines review having been undertaken, type of blood tests required on discharge for monitoring and frequency of blood tests required on discharge for monitoring.
Background
AKI is characterised by a rapid reduction in kidney function with impaired electrolyte, acid-base and water homeostasis. AKI is associated with increased mortality, risk of chronic kidney disease and susceptibility to further episodes of AKI.6 7 The Renal Association UK guidelines divide the severity of AKI into three stages based on the absolute or relative elevation in serum creatinine or the need for dialysis treatment (http://www.renal.org/guidelines/modules/acute-kidney-injury). The incidence of AKI has increased substantially over the last two decades, with an incidence of 3995 per million population in the UK in 2013.8 9 This increase is most notable in the elderly and in patients with multiple comorbidities. In England, the estimated economic burden of inpatient care for AKI is over £1 billion.10 There is also a substantial cost for ongoing care, for patients discharged with AKI, estimated to be 179 million in 2010–2011.10 A review by the National Confidential Enquiry into Patient Outcome and Mortality group in 2009 found substantial deficiencies in the inpatient care of patients with AKI.11 The recognition and management of AKI have become a major healthcare priority in England.
The only formal communication that a GP will receive following an inpatient episode is the EDL. Studies of the accuracy and completeness of EDLs show widespread errors and omissions. In one study 13.3% of EDLs contained medication-related errors.12 Another study examining 637 vascular ward discharge letters found an overall error rate of 10% comprising erroneous information relating to all aspects of care including follow-up arrangements.13 Although studies of the quality of AKI information in hospital discharges have not been published, we anticipated omissions in discharge letters at our large district general hospital.
In 2014 NHS England produced a major planning document—‘the five year forward view’—outlining strategies for simultaneously improving the delivery of healthcare and expenditure by the National Health Service. Two themes of this plan included improving the relationship between primary and secondary care and better prevention of disease. The aims of the AKI CQUIN were to both improve the quality of information given to primary care for patients with AKI and to prevent further AKI by being clear about the follow-up required for an episode of AKI. Four outcome measures were agreed by NHS England to support these aims. The first outcome was the maximum stage of AKI reached during an admission. This is vital since the GP would not be able to easily ascertain that a patient had suffered AKI and the term acute kidney injury avoids the ambiguities of often used text descriptions such as ‘rise in creatinine’, ‘reduced urine output’ or ‘renal impairment’. The stage of AKI is important since more severe AKI portends higher mortality and greater changes to medication dosages. A blood test of creatinine and electrolytes is the most robust way of assessing kidney function. Therefore, the third and fourth outcome measures pertain to informing the GP which blood tests are required and the timing of these. These outcome measures are based on the importance of checking whether the AKI has resolved or persisted and the requirement for ongoing adjustments to the patient’s medication. Patients with non-resolving AKI could then be discussed by their GP with a renal specialist.
Baseline measurement
The quality improvement project (QIP) was approved by the Royal Berkshire Hospital NHS Foundation Trust quality improvement department and was not deemed to require additional ethical approval.
Auditing of EDLs was performed at the end of each month and the results were collated into 3-month blocks to compare against the national CQUIN standard.5 Auditing was performed from April 2015 to April 2016. At the end of each month, all patients with an inpatient episode of AKI that month were ascertained using a national algorithm based on a mathematical analysis of creatinine levels that generated AKI alerts.14 AKI was defined and staged as per the Renal Association Acute Kidney Injury guideline.15 Records were selected randomly by using software on the random.org website to shuffle the list of hospital numbers into a random order and then select records sequentially down the list. Exclusion criteria included death during the admission, interhospital transfer, palliative status, age <18, end-stage renal failure or still being an inpatient. The EDL and blood results were examined, and the records for 25 patients each month with no exclusion criteria were analysed. Each discharge letter was manually checked as to whether the four items of data were present (stage of AKI, medications being reviewed due to AKI, AKI-related blood tests recommended postdischarge and the timing of these blood tests). The auditor used his/her own judgement to determine if the text met the standard of the CQUIN, and if there was doubt a conservative strategy was adopted whereby a second auditor reviewed the record and if only partial documentation was provided the CQUIN aim was regarded as unmet. If a patient had multiple AKI episodes and stages within a single month, only the most severe episode was studied. Results were tabulated using Microsoft Excel spreadsheets and graphs were drawn using the ggplot2 package in the R software environment. We analysed the results monthly and held at least monthly meetings to establish whether additional strategies were required to improve compliance with the quality standard. For reporting to the Clinical Commissioning Group, the data were collated into four quarters (3-month blocks) running from the start of the 2015 fiscal year (April).
During the 1-year project the total number of unique patients with an AKI alert was 3722. When analysed on a per-monthly basis, the total number of patients with an AKI alert was 5434. The overall number of AKI alerts over the year was 12 502.
Prior to the project, several steps had already been taken to assist staff through the introduction of the AKI alert system in March 2015; the AKI alert and stage were available in the blood test reporting system when clinicians clicked to view the biochemistry results (table 1). This built on a year long quality improvement programme to implement a standardized AKI care pathway across the trust, and in primary care.16 Hospital staff were informed of the plans through an AKI launch day, which also included email bulletins of the AKI alert system and the need to report AKI-related information in EDLs. In the first quarter of the study period, a baseline assessment was made of the completion rate of AKI information in EDLs. The completion rate in the first quarter was 22%, indicating that most EDLs lacked AKI follow-up information. No EDL contained the stage of AKI.
A summary of the interventions undertaken during each quarter of the first year
In addition, the content and presentation of a standardised piece of text, regarding AKI aftercare, were developed in collaboration with 20 GPs. The text was designed to ensure the four key pieces of information were presented in a format deemed useful, relevant and easy for GPs to identify and act on as necessary.
Measurement of continued compliance has been continued until present day.
Design
During the baseline assessment period, it became clear after informal discussion with hospital staff that there were several obstacles to clinicians completing EDL AKI information in accordance with the CQUIN. Clinicians were largely unaware of the CQUIN project and consequently were unaware of the four items of information to be recorded. Many clinicians did not feel that stage 1 AKI needed to be reported at all. Staging of AKI had also not fallen into mainstream parlance among clinicians as it was a relatively recently adopted framework. Clinician notes on ward rounds or clerking entries did not usually state the stage of AKI. Clinicians also felt any addition to the EDL would be time-consuming and would compete against the many other requirements that had evolved from other quality improvement initiatives.
We designed our first interventions to educate clinicians about AKI staging and second to make it as easy as possible for them to add the requisite information to the EDL (table 1). We presented the project at the medical and surgical weekly grand round. We attended a ward meeting for every ward/department in the hospital to discuss the project with ward doctors and nurses. New hospital doctors were informed of the CQUIN project at hospital inductions. We sent repeat bulletin emails and displayed information about the project on a large screen television on the medical assessment unit. To make completing the EDL easier, we added an automated AKI annotation of the GP aftercare information accessed by clicking on the ‘AKI annotation’ button. This allowed clinicians to select that an AKI had occurred and the stage. Clicking the button automatically added all four required items of information to the EDL, thereby giving consistent information and facilitating timely EDL completion. This information could be freely edited and added to as clinically appropriate.
Strategy
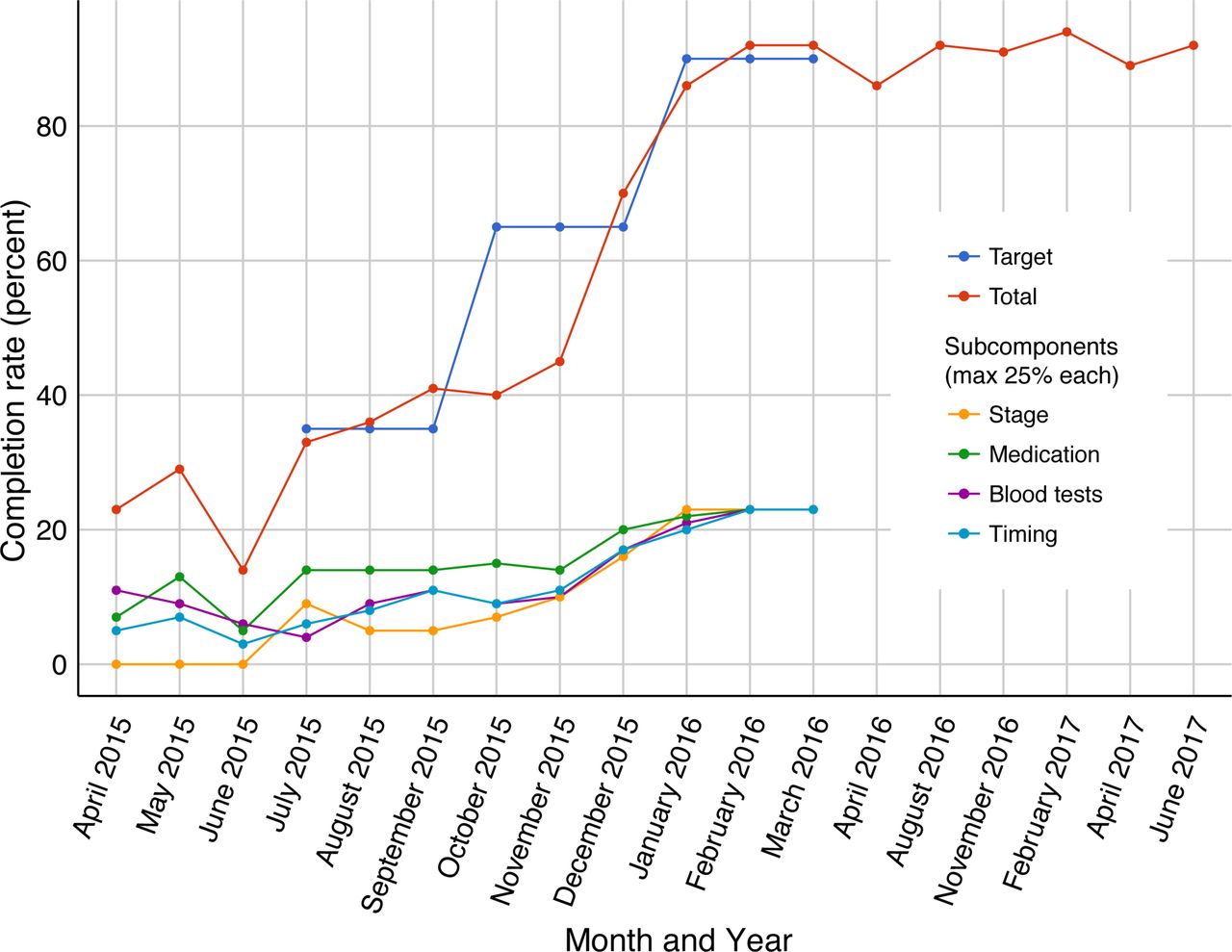
For the second quarter (July–September) following on from the baseline assessment period, the quality standard was set at a 35% completion rate (figure 1). The results for this quarter showed an improvement to 37%. However, there was no continued trend to improvement within the 3-month period, raising a concern that the elevated target of 65% in the next quarter may not be achieved. Several additional strategies were implemented to improve compliance. The QIP was discussed at a further medical grand round. In addition to informal face-to-face education on the wards, targeted reminder emails were sent to staff who had not completed the AKI information for the records audited—the focus was to promote ongoing learning. In addition, a nurse was assigned from elderly care to the project. For 4 hours a week her role was to continue educating junior doctors and nurses about the project and the value to improving patient care. A daily list of AKI alerts was generated for inpatients and reviewed by the project nurse oor nephrologist. The nurse and/or nephrologist then edited the EDLs of these patients so that in the box labelled ’summary list of diagnoses', so that the box stated the presence of an AKI alert. It was hope that when the patient’s usual hospital medical team began to complete the EDL they would notice this alert and the add the full AKI GP aftercare annotation to the EDL themselves. . The EDL was not completed by the project team as it was important the patient’s usual care team completed this with information appropriate to that patient. After noting the presence of the AKI alert within one of the list of diagnosis boxes, the user simply had to click the ‘AKI annotation’ button to automatically add the text ‘Aftercare required by GP’ box and modify it accordingly, particularly with reference to any medication changes made (figure 2).
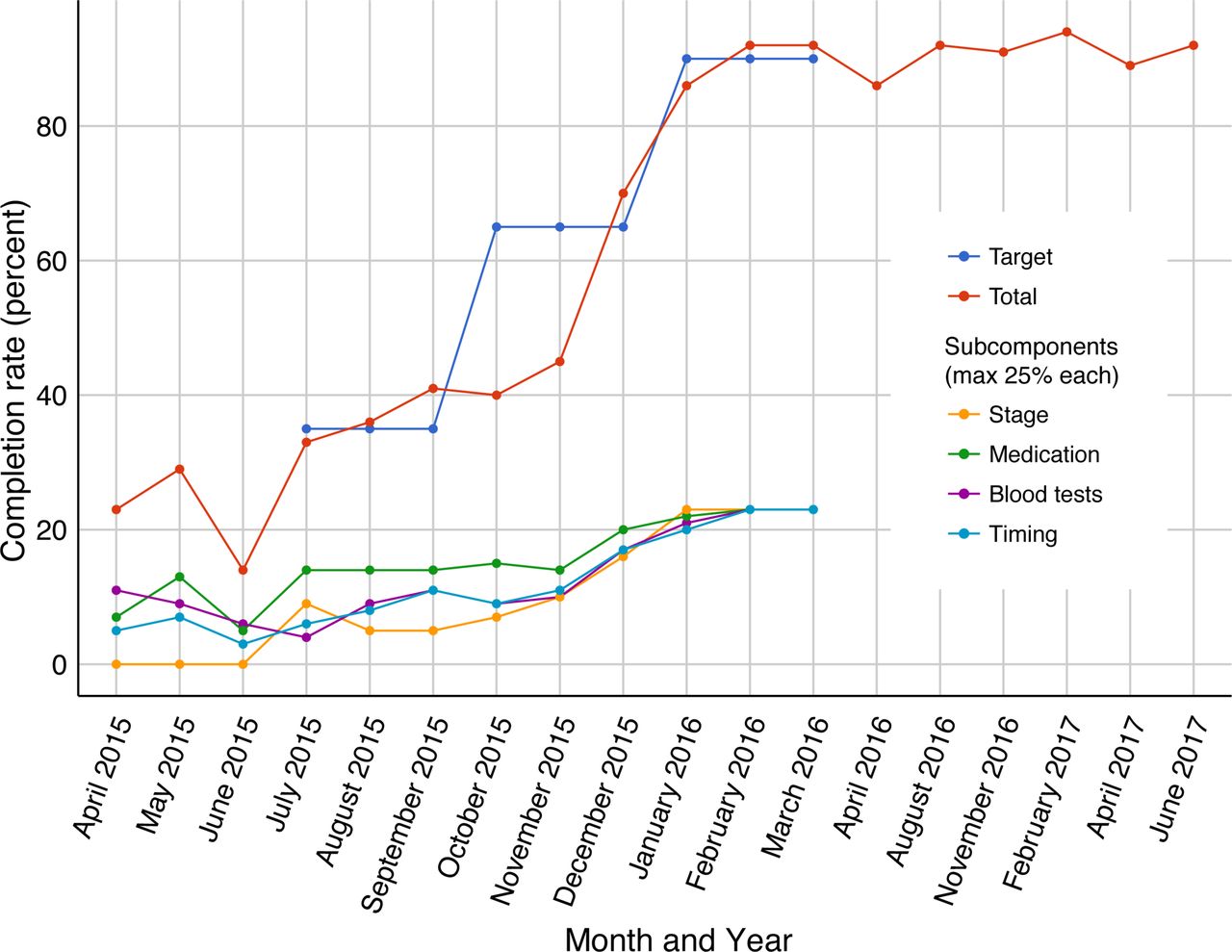
The Commissioning for Quality and Innovation target and actual completion percentages are shown by month and intermittently for the 14 months following completion of the project. The completion percentage of the four individual components is also shown for the first year (maximum percentage 25% each).

{kind=link}
{kind=link}
Screenshots of the AKI alert that appears automatically in the EDL of patients who are considered to have had an episode of AKI during the admission based on changes in serum creatinine. In the third quarter, the button to add ‘acute kidney injury’ annotation information was optional, but in the fourth quarter of the project it was mandatory for progression of the EDL to click this button. AKI, acute kidney injury; CQUIN, Commissioning for Quality and Innovation; EDL, electronic discharge letter; GP, general practitioner.
In the third quarter, the overall completion rate improved substantially to 51% but did not reach the target of 65% (figure 1). It was noted that despite the addition of a diagnosis of AKI to the diagnosis list to prompt staff of an AKI alert, this information was overlooked in some cases and did not result in the clinician accessing the AKI annotation. At the end of this quarter, the AKI alert annotation was added automatically to the summary list of diagnosis boxes (figure 2). In the final month of the third quarter, the completion rate improved to over 65%.
In the first month of the fourth quarter, the electronic AKI annotation was made mandatory by only allowing the EDL to progress if the user had pressed the AKI annotation button for patients with an AKI alert (figure 2, table 1). The user could, however, freely amend or delete the text that was inserted into the ‘Aftercare required by GP’ box. The EDL completion rate improved to 86% for January (figure 1). For the last 2 months of the project, the EDL AKI completion rate improved to 92%, thereby exceeding the target of 90%. Completion did not reach 100% because the AKI alert text was occasionally being inappropriately deleted. Individual feedback was provided to clinicians to assist them with understanding the AKI annotation rationale for those patients.
Results
The quality standard was achieved by the end of 12 months. This change has been sustained in the 14 months since.
Lessons and limitations
At baseline, the presence of the four items of information pertaining to AKI aftercare information for GPs in EDLs was surprisingly low at only 22%. This reinforced the importance of the aim of the national CQUIN project to target an area of AKI care that was recognised as deficient. After 1 year the QIP was successful in achieving >90% completion rate for AKI GP aftercare information. Significant efforts were made to raise awareness of the CQUIN project, including a wide range of education events with medical staff and manually editing EDLs for patients with an AKI alert, until the alert was integrated automatically into the EDL. These measures made some improvements but were labour-intensive. Medical education events alone did not result in sustained behaviour changes. However, where the nurse concentrated on education as part of nurse revalidation, this had a very positive impact. One strategy used for another CQUIN project was to give hospital staff branded water bottles or lanyards. This was noted to achieve success with compliance, but this was not sustained beyond the lifespan of that project. It is possible that such forms of reward improve perception of the project and the sense of being actively involved in the project but does not support sustained changes in behaviour once the reward is removed. Ultimately, the most significant intervention to improve the completion rate was making the AKI annotation a forced function and obligatory to complete for patients with an AKI alert. This electronic intervention is both easily sustainable in the long term and does not require much additional personal input. As one clinician described it, “the new pop up box is very clever because it has identified a patient with an alert so that has streamlined who you need to give aftercare information to.” However, another clinician stated, “the use of a pop up box stating there has been a possible AKI alert adds to the dismissive nature or lack of recognition of any action needed.” The mandated approach was successful in achieving completion of the process, but the perceived tick box approach was felt by many to undermine the intended learning on improving patient outcome in those patients with AKI. As a beneficial side effect of the project, there was an impression among senior staff that the focus on EDL completion for AKI led to a general improvement in the quality of information included in the EDLs.
In terms of limitations to the present QIP, only about 10% of patient records with an AKI alert episode were analysed (in line with the CQUIN methodology). It is possible this sample size did not give representative results. Whether certain patient groups such as elective surgical patients or medical patients had better or worse EDL completion was not assessed. Most interventions were concentrated in the medical departments since the staff for the project were drawn from these departments. The utility of the new information on the perception of EDLs by primary care was not assessed. A completion rate of 100% was not achieved as it was possible to manually over-ride the AKI information that some clinicians did and as a result did not include the appropriate information. In addition, it was also noted that the mandatory inclusion of AKI annotation aftercare information was not being edited where it would have been appropriate to do so, such as for those patients receiving palliative care only. This could lead to confusion in the community when inappropriate AKI follow-up information is received. Patients would also receive a paper copy of their EDLs and could be concerned about the AKI information if it had not been explained to them previously. After the CQUIN standardised information for patients who have experienced an episode of AKI has now been developed.17
The changes implemented during this QIP were made without specific additional investment in staff time and resources. In addition, possible electronic solutions coupled with critical CQUIN time constraints were seen as difficult to incorporate within the pipeline for developing the Trust electronic record. Perseverance, creative solutions and a focus on the fiscal reward resulted in the changes made sufficient to achieve the quality standard. This standard is still being achieved 14 months on. This may, however, largely reflect AKI aftercare information being a forced function, rather than a sustained change in clinician behaviour towards the longer term management of AKI beyond the hospital boundary. Only when this action had to happen was it done, perhaps losing some of its formative value.
Conclusion
A 1-year QIP had a substantial positive impact on the recording of important information about AKI episodes in EDLs at a major district general hospital in England. By the end of the study, omissions relating to AKI information were reduced from 78% to less than 10%, indicating our QIP was highly effective. Although several educational and awareness initiatives were introduced, the single most important factor in improving documentation was to mandate user review of AKI aftercare information for GPs in patients with AKI alerts. The achieved change of >90% completion of GP aftercare information in patients with an AKI alert during their hospital admission has been sustained in the 14 months since. Our study encompassed hospital-wide inpatients, and our results could be replicated at other acute hospitals that have implemented an EDL system connected to an AKI alert system.
References
Footnotes
Handling editor Jessamy Bagenal
Contributors MER and EV designed the project, collected the data, analysed the data and wrote the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.