Article Text

Abstract
Electrocardiograms (ECGs) are performed to determine an individual's cardiac rhythm. Approximately 25,000 ECGs are performed yearly throughout our hospital system. Historically only 68% of all ECGs were performed with the proper order linked to the electronic ECG reading system (MUSE). Failure to link the orders to the electronic reading system leads to problems in patient safety, reporting and hospital revenue.
Our aim was to increase the percentage of linked ECG orders in MUSE compared to total ECGs performed from 68% to 95%.
We created a detailed process map of ECG order linking to the MUSE electronic system. FMEA and Pareto chart creation were used to determine etiology of process failures. Multiple interventions (LOR1 to LOR3) were implemented utilizing the PDSA technique. Process control charts were used to evaluate change.
FMEA and Pareto chart determined most common failures were related to: 1) ECG order not electronically acquired properly, 2) duplicate ECGs and 3) ECG order was not electronically placed. We performed multiple interventions including: 1) ECG performance education, 2) created reminders on the ECG machines, 3) specialized electronic linking system for physician readers and 4) bar-code scanners for all ECG machines. These changes improved ECG order linking to MUSE from 68% to 95% over 6-months. In direct comparison between fiscal year (FY) FY2014 to FY2015, the number of ECGs performed increased 2% while billing increased by 23%.
Utilization of quality improvement methodology allowed us to identify failures for ECG order linking. We established multiple successful interventions amongst different hospital locations and improved our compliance, billing and reporting of ECGs.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Cincinnati Children's Hospital is a large children's hospital with 598 beds, over 35,000 admission and 1.3 million patient encounters a year. The electrophysiology group along with the business team at the Heart Institute at Cincinnati Children's Hospital noted a long-standing problem with electrocardiograms (ECG) being performed without a linked order in the electronic medical record, in this case Epic. This lack of linking orders to ECG performance created two important problems, one clinical and related to patient safety and one financial. The clinic problem was that in order to view the ECG with the interpretation from the electrophysiologist directly reported in Epic (the electronic medical record) the ECG had to be linked to an order. Also, an ECG may have been performed without the physician being aware and or not indicated. Therefore, there were an unacceptable number of ECGs that could not be read and posted to Epic for the ordering physician to have the final results directly reported. Financially, this created a problem because no study can be billed to the payer without first having an order. Therefore all ECGs performed without first being linked to an order were resulting in no charges. Our SMART Aim was to increase the percentage of linked ECG orders in the ECG electronic reading system MUSE from 68% to 95% from February 2015 to May 2015.
Background
Currently we perform and read approximately 25,000 ECGs a year. The percentage of ECG performed with orders was approximately 68%. Performing and reading ECGs utilize resources including ECG technicians and physicians. There are also costs of the ECG machine and yearly maintenance. If 30% of all ECGs are performed without a linked order there are issues with compliance, reporting and loss of revenue.
Baseline measurement
Our measurement was percentage of ECGs linked to an order in MUSE, an electronic ECG reading system. The rationale for the project was that unlinked ECG orders in MUSE create issues in patient compliance, reporting and revenue. This measure will determine the number of ECGs linked to the EPIC order in MUSE. The ‘gold standard’ value is having a proper EPIC order placed for each individual ECG performed, and the order utilized to perform the ECG. The population was all ECGs performed at our institution and satellite locations. Data sources included: Epic, MUSE, and creating of Excel spreadsheets with data from all locations where ECGs were performed. We collected daily data and reported the data weekly. The total ECGs were subdivided by location performed. The calculation of ECG linked to MUSE was: (ECG linked MUSE)/(ECG total) × 100 = % ECG linked. We gathered clinical information from Epic as well as our ECG system (MUSE) and billing data from our finance team. We examined baseline data from January 2015. During this month there were >2,300 ECGs performed and only 68% of the ECGs were performed with the proper linkage of an order in Epic to our ECG reading system MUSE.
Design
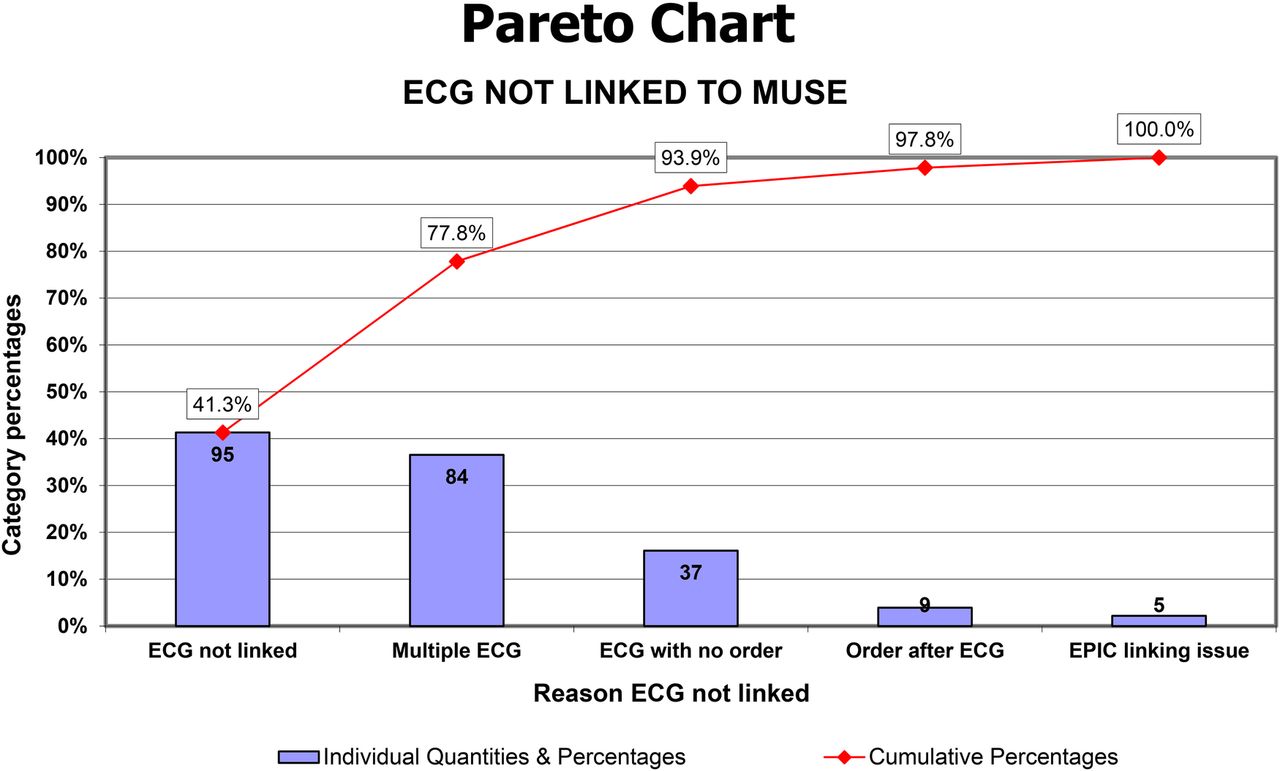
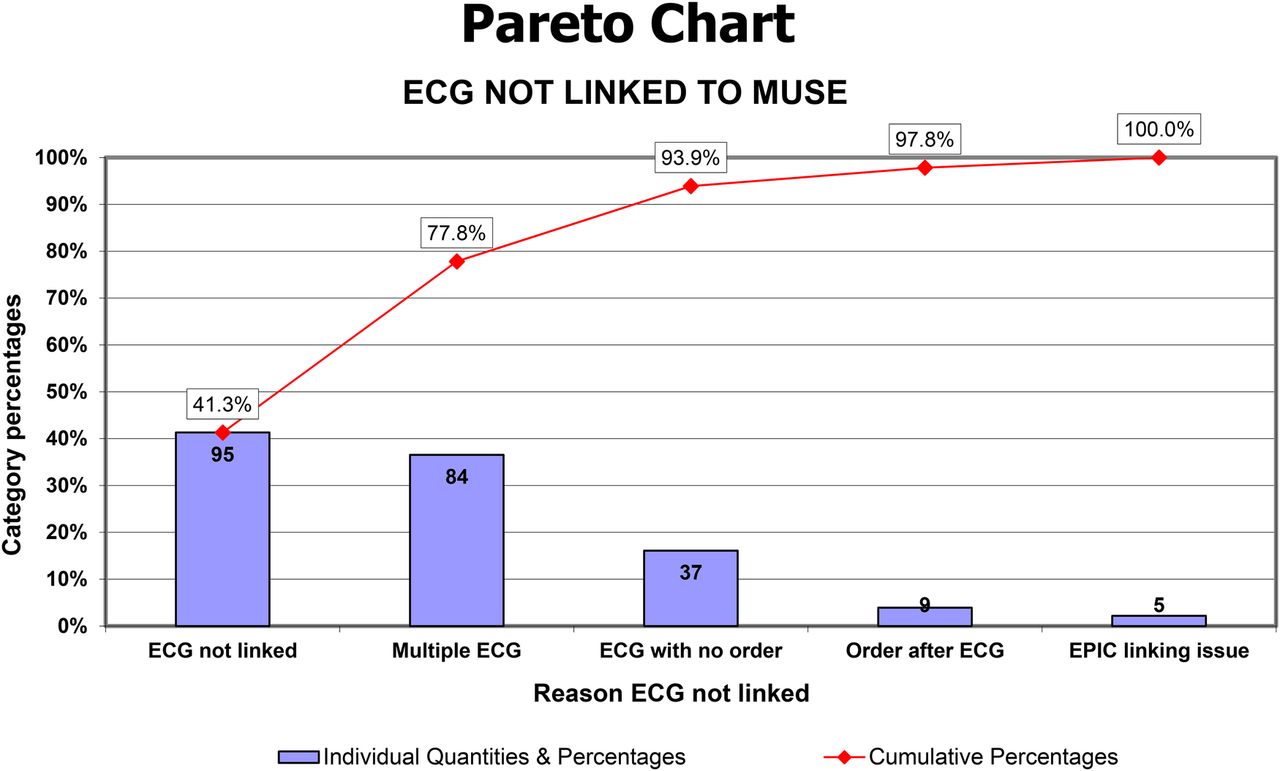
We utilized the Model for Improvement for this project. Initially we observed and walked through the process of ECG ordering in Epic and linking to the MUSE system. We identified problems with registration, ECGs performed without orders (often occur weekends and evenings, and occur when ECGs are performed by untrained staff), ECGs performed with an order but not properly linked to MUSE system, and finally ECGs performed in multiple. A Process Map was created documenting the ECG ordering and linking system. FMEA and Pareto charts determined most common failures were related to: 1) ECG orders in Epic not electronically linked to the MUSE system properly, 2) multiple (or duplicate) ECGs performed at the same time and 3) ECG orders not electronically being placed in Epic (figure 1).
Strategy
We created a SMART Aim with a goal to increase the percentage of linked ECG orders in MUSE compared to total ECGs performed at our institution and satellite clinics from 68% to 95% by May 2015.
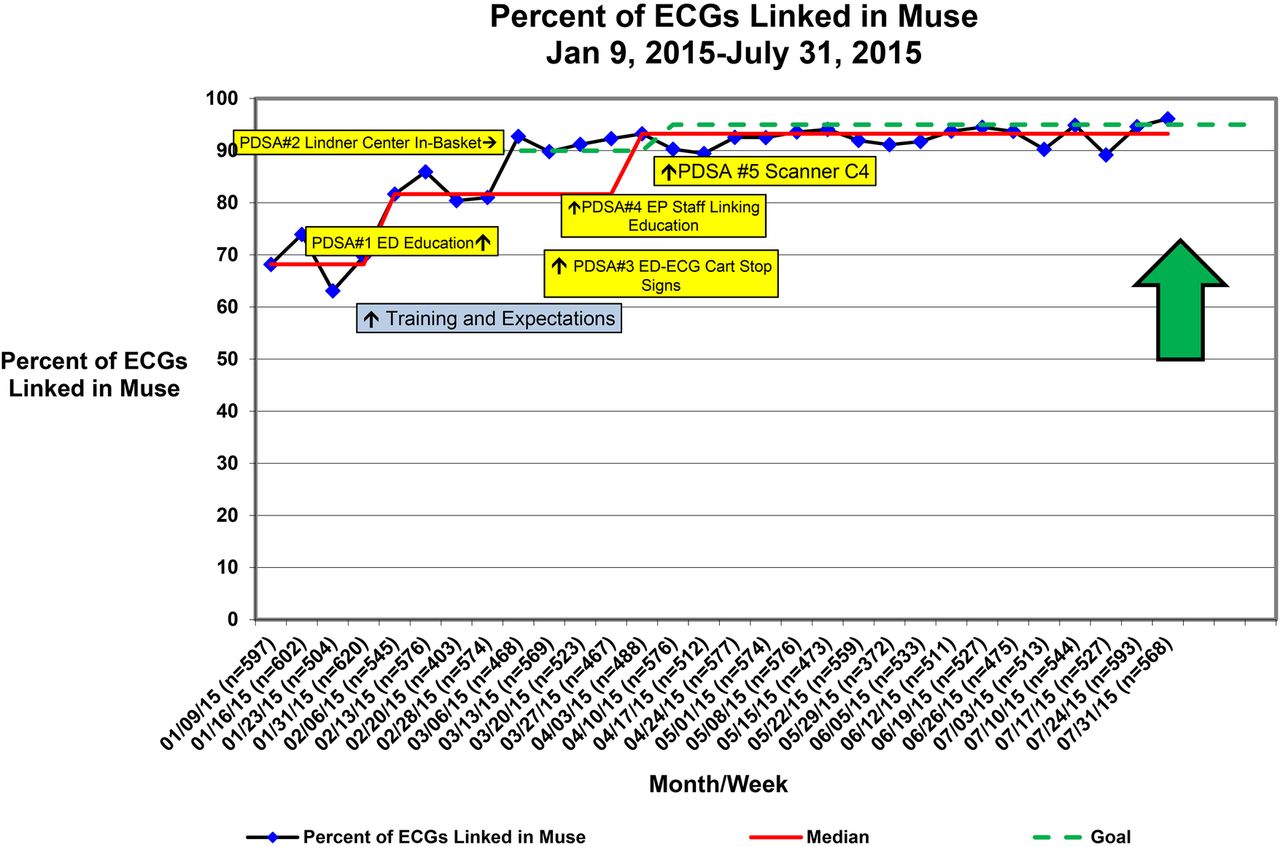
PDSA Cycle 1 Emergency Department (ED) Education for those who perform ECGs. There are a large volume of ECGs obtained in the ED with many different technicians and nurses that perform the ECG. The technicians and nurses in the ED were educated on proper use of ECG order and linking to MUSE. There was coordinated nurse education that was started with managers and spread to all providers that perform ECGs. The education process was effective with improvement in proper order linkage but the level of reliability was low. There is also significant turnover in staff and requires multiple cycles of education throughout the year. This intervention improved ECG order linking within the ED from 35% to 85%.
PDSA Cycle 2 Creating specialized electronic in-baskets in MUSE. Certain hospital or clinical locations that were poor performers had specialized electronic baskets that allowed our technicians to link the order prior to being finalized. We worked with the IT department and successfully routed these ECGs to a specific electronic in-basket. Out ECG technicians then were able to successfully link the order to the ECG prior to being routed to the reading Electrophysiologist. This change improved ECG order linking within these specific locations from 14% to 94%. This system continued to rely on a proper order placed by the ordering provider prior to the ECG being performed by the technician or nurse.
PDSA Cycle 3 Stop sign reminder on ECG machines. This change was easy to implement but over time did not have a significant impact. The change did not improve ECG order linking. Low level of reliability but easily seen and placed next to confirmation button.
PDSA Cycle 4 ECG readers trained to link order if not performed. Prior to confirmation of ECG, our four trained ECG readers evaluated if an order was placed and linked. If the order was present but not linked the ECG reader would link prior to confirmation. There were only 4 Electrophysiologist to train and this was a simple step requiring a single change in the MUSE electronic reading system. The change improved ECG order linking by 1%, overall from 91% to 92%. This change was later in our project and we had already seen substantial increases in ECG order linking at the start of this PDSA.
PDSA Cycle 5 Added a scanner to all ECG machines. High level of reliability requiring the technician or nurse to have an order placed in Epic so the bar-code scanner could access the order and link electronically to the MUSE ECG system. The system was easy to use (most technicians and nurses were already using a bar-code scanner for other tests). We allowed for a manual override for emergency type situations. This was first tested in select units that were high performers (high ECG order linking) including our own Cardiology ECG technicians. After identifying minor issues the change was slowly spread to all outpatient and inpatient units successfully. This system relied on an order being present prior to performing the ECG and if not present the scanner would not work. Once scanned, the order was automatically linked to the ECG in our reading system. Since implementing this change the ECG order linking from 92% to 95%.
Results
The project measured ECGs that were performed but did not have an EPIC order linked to the MUSE reading system. We reviewed the percentage of appropriately linked ECGs in the system. This measurement was performed by evaluating the number of appropriately linked ECGs over the total ECGs performed in a time period. FMEA and Pareto chart determined the most common failures were related to: 1) ECG order not electronically linked properly, 2) duplicate ECGs and 3) ECG order was not electronically placed. We performed multiple interventions including: 1) ECG acquisition education, 2) created reminders on the machines, 3) specialized electronic linking system for physician readers and 4) bar-code scanners for all ECG machines.
When the project started 68% of the ECGs performed at our institution had an appropriate order linked to the ECG reading system MUSE. After our described interventions, 95% of the ECGs were linked appropriately (figure 2). When evaluating locations outside of Cardiology Division, only 35% of the ECGs were linked appropriately and increased to 90% at the end of the project (figure 3). The individual improvements were described in the Strategy section under each PDSA. The improvement in ECG orders linked to MUSE allowed our institution to directly report results in EPIC improving patient safety. If an ECG order was not linked to MUSE, the ECG would not be reported directly into our hospital electronic system. To find results the provider would have to enter the electronic record and then search specifically for that individual ECG result. If the order is directly linked to MUSE, the result is automatically sent to the ordering provider and required that provider to review and sign-off on the result. Therefore, the percentage increase in ECG linkage was directly related to resulting the order to the provider. In addition this project has resulted in improved billing and resultant revenue. In direct comparison between fiscal year (FY) 2014 to FY2015, ECG acquisition increased by only 2% while billing for ECGs performed increased by 23%. So over the past year our billing improved by over 20% with only a small increase in overall ECG performance, which was directly related to an increase in the electronic order linked to the ECG. This proper order allowed for the hospital to bill appropriately for the performance of the ECG.

{kind=link}
{kind=link}
{kind=link}
Lessons and limitations
ECGs are performed by many different technicians and nurses at our institution. Within the Cardiology department we were able to train our staff and subsequently have a high appropriate linking of ECGs early on. The majority of poor performers occurred outside of Cardiology and required interventions with higher levels of reliability. When there are large numbers of technicians and nurses performing studies, education alone is not reliable enough for long-term success. We created systems including electronic in-baskets to link ECGs prior to being confirmed, allowing readers to link ECGs that were not appropriately linked and utilization of bar-code scanners that were simple and reliable to create an improvement in appropriate linking of ECG orders to our electronic reading system. For patient safety we felt that we could not remove ECG machines from all clinical settings which continues to allow a low percentage of ECGs performed incorrectly.
Conclusion
Utilization of quality improvement methodology allowed us to identify failures for ECG order linking to our electronic reading system MUSE. We established multiple successful interventions amongst different hospital locations and improved our compliance, reporting and patient safety, and billing of ECGs performed in a busy Children's Hospital.
Reference
Footnotes
Declaration of interests Nothing to declare
Ethical approval According to the policy activities that constitute research at (Cincinnati Children's Hospital Medical Center) this work met criteria for operational improvement activities exempt from ethics review.