Article Text

Abstract
Our Family Health Team is located in Toronto, Canada and provides care to over 35 000 patients. Like many practices in Canada, we took an opportunistic approach to cervical, breast, and colorectal cancer screening. We wanted to shift to a proactive, population-based approach but were unable to systematically identify patients overdue for screening or calculate baseline screening rates. Our initiative had two goals: (1) to develop a method for systematically identifying patients eligible for screening and whether they were overdue and (2) to increase screening rates for cervical, breast, and colorectal cancer. Using external government data in combination with our practice's electronic medical record, we developed a process to identify patients eligible and overdue for cancer screening. After generating baseline data, we implemented an evidence-based, multifaceted intervention to improve cancer screening rates. We sent a personalized reminder letter to overdue patients, provided physicians with practice-level audit and feedback, and improved our electronic reminder function by updating charts with accurate data on the Fecal Occult Blood Test (FOBT). Following our initial intervention, we sought to maintain and further improve our screening rates by experimenting with alternative recall methods and collecting patient feedback. Screening rates significantly improved for all three cancers. Between March 2014 and December 2016, the cervical cancer screening rate increased from 60% to 71% (p<0.05), the breast cancer screening rate increased from 56% to 65% (p<0.05), and the overall colorectal screening rate increased from 59% to 70% (p<0.05). The increase in colorectal screening rates was largely due to an increase in FOBT screening from 18% to 25%, while colonoscopy screening remained relatively unchanged, shifting from 45% to 46%. We also found that patients living in low income neighbourhoods were less likely to be screened. Following our intervention, this equity gap narrowed modestly for breast and colorectal cancer but did not change for cervical cancer screening. Our future improvement efforts will be focused on reducing the gap in screening between patients living in low-income and high-income neighbourhoods while maintaining overall gains.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Cancer is the leading cause of death in Canada, yet mortality and morbidity can be prevented through regular screening for cervical, breast, and colorectal cancer.1 Primary care providers play an important role in screening – identifying and approaching eligible patients, counseling on the risks and benefits of screening, and referring for or performing relevant tests.
Our Family Health Team is located in downtown Toronto, Canada. In 2014, we provided primary care to approximately 35,000 patients at five clinic locations; in 2015, we opened a sixth clinic location and accepted an additional 5,000 patients in the following two years. Prior to 2014, our practice did not have complete baseline data on our own cancer screening rates, nor were we able to proactively identify patients due for screening. We hypothesized that methods of screening varied by physician because there was no coordinated recall effort. The practice used an electronic medical record (EMR), but data were not always accurately entered which precluded the usefulness of electronic reminders, particularly for colorectal cancer. Finally, our practice serves a diverse, urban community including many patients experiencing social disadvantage and it was unclear if our screening rates were equal for all patient groups, particular those with different income levels.
We first sought to create a method for easily identifying patients overdue for screening using data from our practice EMR and a new provincial cancer screening registry. We determined that our baseline screening rates for cervical, breast, and colorectal cancer were 60%, 56%, and 59% respectively. We then aimed to increase cervical, breast, and colorectal cancer screening rates to 67%, 60%, and 67% within a six month period using evidence-based quality improvement strategies. Our screening targets were informed by the average screening rates in our health region and province. We did not have explicit goals regarding income-related inequalities, but rather wanted to understand how screening rates differed between socioeconomic groups, which would inform future initiatives. Once we increased screening rates, we sought to maintain our improvements, reduce resources expended, and optimize the patient experience.
Background
When compared to countries of similar size and wealth, most Canadian family physicians struggle to generate lists of patients overdue for cancer screening. Only a quarter of Canadian family physicians report that they can easily generate a list of patients needing preventive cancer care.2 The issue is not that Canadian family physicians lack data, but rather, that the information is often disorganized or compiled by external agencies who do not have the ability to directly integrate with practice EMR systems. Without lists of overdue patients, most Canadian family physicians take an opportunistic approach to cancer screening.3
In 2014, the Ontario government introduced a central provincial cancer screening registry that contains screening information for cervical, breast, and colorectal cancer for all patients in Ontario enrolled to a medical home.4 Physicians can access the cancer screening registry electronically, which provides them with lists of their patients who were eligible for screening. The lists contain details on patients' last screening and whether they are up-to-date or overdue. Physicians need to create an account to securely download the information for their own patients.
Studies suggest that quality improvement (QI) initiatives based in primary care practices can increase cancer screening rates.5–9 The following interventions directed at patients and providers have been shown to increase cancer care rates:
Patient reminders and recalls tell patients that they are due or overdue for screening and can be sent by text (email, letter, etc.) or by telephone.5
Small media interventions communicate educational or motivational information about cancer screening via videos or printed materials (brochures, pamphlets, flyers, etc.).6
Provider assessment and feedback interventions evaluate and/or inform physicians on their cancer screening performance5
Provider reminder and recall interventions tell physicians that a patient is due or overdue for cancer screening.6
Baseline measurement
We measured cancer screening rates in accordance with Ontario's cancer screening guidelines. For cervical cancer, we calculated the percentage of women age 21 to 69 who had a Pap smear within the last 3 years. Women with known cervical cancer or prior hysterectomy were excluded from the denominator. For breast cancer, we calculated the percentage of women age 50 to 74 who had a mammogram within the last 2 years. Women with known breast cancer or prior mastectomy were excluded from the denominator. For colorectal cancer, we calculated the percentage of adults age 50 to 74 who either had a Fecal Occult Blood Test (FOBT) in the last 2 years or a colonoscopy in the last 10 years. Adults were excluded from the denominator if they had known colon cancer, bowel resection, or inflammatory bowel disease.
In March 2014, baseline screening rates were 60%, 56%, and 59% for cervical, breast, and colorectal cancers, respectively. Initially, we planned to measure these data quarterly to monitor progress. Although we were initially delayed, we were able to meet this goal early in 2015.
Design
This QI project had two distinct but related goals. First, we aimed to identify patients overdue for cervical, breast, and colorectal cancer screening using data from the provincial cancer screening registry together with the practice EMR. Second, we aimed to increase these screening rates using an evidence-based QI intervention. The intervention included three main components. Each overdue patient received a personalized reminder letter. Physicians reviewed their patients' screening status and indicated who should be contacted. The letter included a message signed by the patient's family physician and brochures about the relevant screening tests. We modified this intervention by experimenting with phone calls as an alternative recall method and collecting patient feedback on the process. Also, we provided physicians with individualized feedback on their cancer screening rates and compared these to screening rates among their peers in their clinic and the entire Family Health Team. Finally, we updated charts with accurate data on the FOBT and improved our EMR reminder function. This project was guided by an interdisciplinary team that included students, physicians, health disciplines, executives, and administrative support.
Strategy
PDSA #1: Identify patients overdue for cervical, breast, and/or colorectal cancer screening and calculate baseline screening rates
Plan: We sought to determine whether the provincial cancer screening registry contained accurate information about which patients were overdue for cervical, breast, and colorectal cancer screening. We predicted that the data would be accurate for breast and colorectal cancer, but not for cervical cancer as our Pap tests were processed in the hospital and the registry did not have access to hospital test records.
Do: In May 2014, we tested the accuracy of the data by having three physicians compare the provincial cancer screening registry to their own patient records.
Study: All three physicians found that the registry contained correct breast and colorectal cancer screening data, but incorrect cervical cancer screening data. We also found that provincial colorectal screening information was more accurate than our own medical records, due to problems with how FOBT tests were uploaded into our EMR.
Act: We determined that we should use data from the provincial screening registry to identify patients overdue for breast and colorectal cancer, but that we needed to use our practice EMR to identify patients overdue for cervical cancer screening. We used the Visual Basic programming language in Microsoft Excel to merge data from the registry (for breast and colorectal cancer) and our practice EMR (for cervical cancer) to generate an integrated list of patients eligible and overdue for any of the three tests. A small group of physicians reviewed these lists and agreed they were largely accurate. We then prepared a list of patients overdue for screening for each physician in the department
We determined that the baseline screening rates for the Family Health Team were 60%, 56%, and 59% for cervical, breast, and colorectal cancer, respectively. Patients living in low income neighbourhoods were less likely to receive screening. The absolute difference in screening rates between the lowest and highest income quintile were 3% (cervical; p>0.05), 10% (breast; p<0.05), and 11% (colorectal; p<0.05).
PDSA #2 - Increase baseline cancer screening rates using a multi-faceted, evidence-based approach
Plan: By the fall of 2014, we aimed to raise cervical, breast, and colorectal cancer screening rates to 67%, 60%, and 67%, respectively. We designed a multifaceted intervention that incorporated four evidence-based strategies: i) personalized recall letters for patients signed by their physician, ii) inclusion of small media (brochures) with the mailed letter, iii) physician audit and feedback, and iv) improved point-of-care reminders in the EMR. Due to the centralized nature of our department's administrative staff, and the human resources required to send the reminder letters, it was not practical to tests the effectiveness of the letters on a small scale, and spread if effective. Rather, we had to take advantage of the resources available and send letters for all practices at one time.
Do: For each physician in the Family Health Team, we prepared an integrated list of patients overdue for any of the three screening tests using methods developed in PDSA #1. Physicians were sent a link to an electronic copy of their list of overdue patients and asked to identify patients who should be sent a reminder letter. Links were sent over secure email and lists of overdue patients were saved to a secure folder only accessible to the physician and a handful of project staff.
Initially, few physicians reviewed their lists with some reporting that the task was overwhelming. We extended deadlines and ultimately provided outstanding physicians with a paper copy of the list that only included overdue patients. Ultimately, 49 of 51 physicians reviewed their report and indicated which of their patients should receive a recall letter.
We used the Microsoft Word mail merge function to create a personalized letter for each patient from their specific family physician asking them to book an appointment to discuss the relevant screening tests. A single letter included information on all overdue tests for each patient. In August 2014, 7,493 letters were mailed to patients along with relevant brochures.
We used the list of overdue patients prepared for each physician to create a personalized feedback sheet for each physician that summarized cancer screening rates for his/her practice compared to average screening rate for physicians at their clinic site and the Family Health Team. These were distributed to physicians' clinic mailboxes.
Electronic medical record charts were manually updated with data on FOBT from the cancer screening registry and abnormal results were highlighted for physician review. This process increased the accuracy of data in the EMR and enhanced point-of-care reminders.
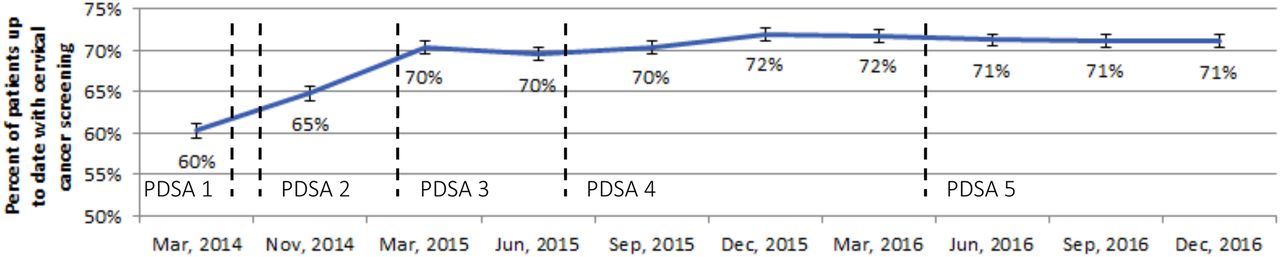
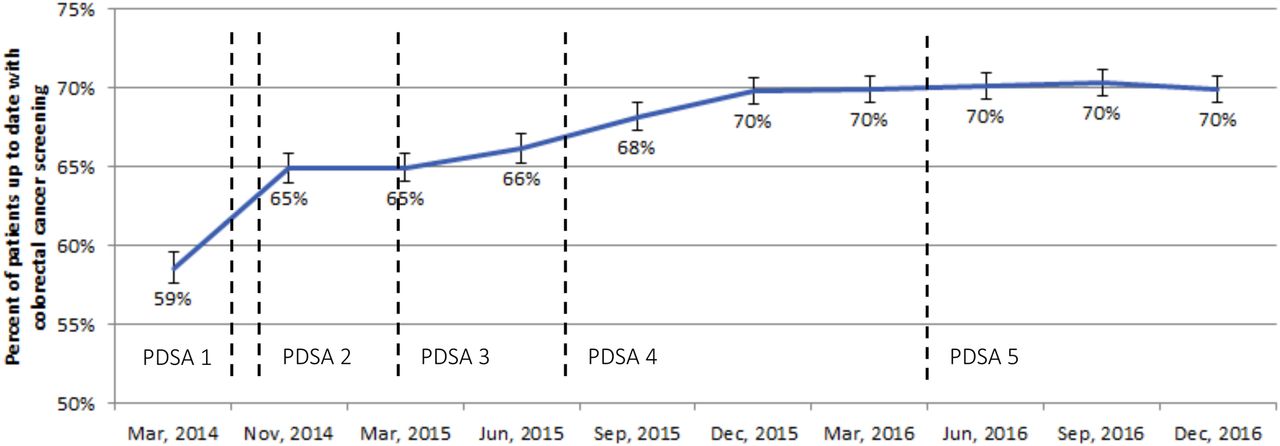
Study: By November 2014, cancer screening rates had increased from 60% to 65% (p<0.05), 56% to 65% (p<0.05), and 59% to 65% (p<0.05) for cervical, breast, and colorectal cancer, respectively (Figures 1 to ⇓3) . Differences in screening rates between patients living in the lowest and highest income quintile persisted for cervical and breast cancer but were slightly reduced for colorectal cancer.
We suspected that increases in our screening rates were mostly due to proactive recall of overdue patients by mailed letter but were unable to disentangle the relative contributions of each component of the multifaceted intervention. Mailing recall letters and informational brochures cost approximately $14,000 (Canadian). About 300 of the mailed letters were returned to sender.
We also learned that some patients who received cervical cancer screening letters had already received a Pap test. After investigating the issue, we found that some patients had a Pap test captured in the provincial registry that did not appear in our own practice EMR. This situation occurred, for example, if patients were new to our practice or were seeing a consultant who performed the test at an outside lab.
Act: We planned to improve how accurately we identified patients overdue for cervical cancer by using data from both the practice EMR and the provincial cancer screening registry.
PDSA #3: Improve the accuracy of our method for identifying patients overdue for cervical cancer screening
Plan: Instead of relying solely on our EMR data, we aimed to combine data from both the EMR and provincial registry to more accurately identify patients overdue for cervical cancer preventative care and determine the screening rate. We hypothesized that our cervical cancer screening rate was higher than the 65% we observed in November 2014.
Do: In March 2015, we obtained cervical cancer screening data from the provincial registry and the EMR separately. We then used Statistical Analysis System 9.3 to merge these data sources into a single database that included information on whether the patient had a Pap test documented in either the provincial registry or our EMR. We counted the date of the last Pap test, as their true date of latest Pap test regardless of whether this information was obtained from the EMR or the provincial registry and used this information to determine which patients were overdue for screening.
Study: Using the methods described above, we calculated our cervical cancer screening rate at 70% as of March 2015 (Figure 1).
Act: We now calculate cervical, breast, and colorectal screening using data from both the practice EMR and provincial registry as each data source alone contains incomplete information. After determining this more accurate method of calculating screening, we sought to determine whether other methods of recall, aside from mailed letter, were feasible and their relative cost and effectiveness.
PDSA #4: Maintaining gains in screening rates and testing different recall methods
Plan: To maintain gains in screening rates, we decided to recall patients overdue for screening annually. In the summer of 2015, we undertook a randomized trial to compare the effectiveness and cost of a mailed letter compared to a phone call. We predicted that phone calls would be less costly and similarly effective to mailed letters. We thought the results of the randomized trial would inform future work but also enable us to maintain the overall gains in screening rates. We realized that maintaining rates may be particularly challenging as our practice opened a sixth practice site in 2015 and accepted approximately 5000 new patients over the next two years.
Do: In the summer of 2015, we randomized 5270 patients to receive either a letter or phone call to recall them for cancer screening.
Study: Although we planned to complete this PDSA in the summer of 2015, the phone calls took longer than expected, and we did not finish contacting patients until December 2015. The results of the randomized trial are pending. However, our experience taught us that phone calls were more logistically difficult and consumed significant staff resources which would make them challenging to sustain in the long-term. Through this period and after, our screening rates were maintained or increasing (see Figure 1 to ⇓3). However, we have not been able to reduce disparities in screening by neighbourhood income quintile (Table 1).
Act: We continue to recall patients annually for cancer screening. In the summer of 2016, we decided to recall patients using mailed letter only. To try and improve equity in screening, we have embarked on a qualitative research study to work with patients living with a low-income to understand how we can make screening more accessible for them.
PDSA #5: Understand the patient experience of being recalled for cancer screening
Plan: We wanted to understand what our patients thought of our efforts at cancer screening recall and what we could do to improve. We predicted that patients would appreciate being proactively recalled by their family physician.
Do: In the spring of 2016, we randomly selected 40 patients who had been recalled by either letter or phone call the previous summer. We called these patients and asked them a few open-ended questions to understand their experience of being recalled for screening and get their feedback on how our intervention could be improved. We spoke to patients who we reached directly on the phone but did not leave a voicemail to avoid triggering unnecessary anxiety among patients.
Study: We spoke with 8 of the 40 patients we called; we were unable to reach the remaining patients. Patient feedback was largely positive, however many patients indicated that they were already planning to come for screening and were only a few weeks or months overdue. As such, they did not act on the letter. We realized that recalling newly overdue patients may not be an efficient use of resources. Patients also suggested adding a space on the recall letter where they could note the date and time of their appointment.
Act: As a direct result of patients' feedback, we now only recall patients who are either six months or more overdue, or who are newly eligible due to age. Despite recalling fewer patients, our gains have been maintained for more than two years since this work began (figure 1 to ⇓3). We have also made changes to our letter based on patient suggestions.
Results
We successfully identified patients overdue for cancer screening by merging data from a provincial cancer screening database with our practice EMR. We undertook a multifaceted, evidence-based quality improvement initiative that included proactive recall of patients overdue for screening using mailed letter. The intervention significantly increased cervical, breast, and colorectal cancer screening rates over a six-month period (Figures 1 to ⇓3). We increased our data accuracy for cervical cancer by including data from more than one source to identify overdue patients. In the two years following our initial intervention, we continued to recall patients proactively and screening rates were maintained or increased (Figures 1 to ⇓3). We learned that recalling patients more than six months overdue by letter seems to be the most efficient use of resources in order to maintain the increases in cancer screening rates.
We found that patients in our practice who lived in low income neighbourhoods were less likely to be screened for cervical, breast, and colorectal cancer. Our intervention did not seem to have a sustained impact on income-related disparities in screening (Table 1).



{kind=link}
{kind=link}
{kind=link}
Ratio of Cancer Screening in Lowest vs. Highest Income Quintile, Over Time.
Lessons and limitations
We started this initiative with the dual goal of better understanding cancer screening in our Family Health Team, and then increasing these rates. We owe our success to the dedication and efforts of the interdisciplinary working group leading the initiative, the family physicians involved, and our administrators who provided us with the needed resources. Engaging approximately fifty physicians in the initiative was logistically challenging. Each physician was required to sign up for the provincial cancer screening registry, delegate an administrator to access their data, verify which of their patients should be recalled for screening, and see the patients that made an appointment as a result of the recall effort. Despite these tasks, the physician response to this initiative was overwhelmingly positive with most feeling grateful to have an organized approach that enabled them to better meet screening targets for their patients.
Throughout this process, we also learned that administrative data sources can be imperfect. As mentioned, the provincial cancer screening registry contains inaccurate data on cervical cancer screening for our Family Health Team. As a result, it was necessary to merge these data with our practice EMR data to get a more complete understanding of cervical cancer screening. One limitation was that the provincial cancer screening registry did not have accurate data on patients who were not sexually active or patients who identified as transgender and changed the gender on their health card – two groups where screening needs may be different than indicated by the provincial database. Because most family physicians verified which patients should be recalled, it is unlikely that patients were contacted inappropriately. However, future efforts will focus on better identifying these patients in our EMR.
The multifaceted nature of our intervention was both a strength and a limitation. We used multiple evidence-based strategies at the same time to try and increase our screening rates which may have made our intervention more successful. However, it also means that we were not able to assess the relative contribution of each method in increasing cancer screening rates. It is notable, however, that our gains in cancer screening were maintained during a period where we welcomed an additional 5,000 new patients to our practice, many of whom had not previously had a family doctor. Others have also found that multifaceted interventions in primary care are a promising approach to improving screening rates.9 ,11 Our intervention was also dependent on information we received via the provincial cancer screening registry but other aspects of our intervention are still generalizable to practices in other jurisdictions that can generate lists of overdue patients from their EMR.
Finally, we noted income-related disparities in screening for all three cancers. Our intervention was associated with a modest narrowing of these inequities for breast and colorectal cancer but disparities remain. Income-related disparities in screening are well documented and more study is needed on how they can be successfully addressed.12 ,13 We are undertaking research to better understand the views and needs of patients living with a low-income and how we can make cancer screening more accessible to the them.
Conclusion
Data from a practice electronic medical record and external reports can be combined to generate an accurate list of patients overdue for testing. These lists can be created quickly and inexpensively. A multifaceted QI initiative that incorporates systematic recall by mailed letter, physician audit and feedback, and improved point-of-care reminders can improve overall cancer screening rates. Recalling patients by mail was more feasible given practice resources than recalling by phone calls and incorporating patient feedback helped improve our letters. Our next steps include understanding barriers to cancer screening for patients living with a low income to reduce income-related disparities in cancer screening.
Acknowledgments
The authors gratefully acknowledge the work of the working group guiding this initiative, particularly Madison Giles and Lisa Miller. They also acknowledge the thoughtful guidance of Dr. Aisha Lofters, Amy McDougall, Dr. Ed Kucharski, Dr. Fok-Han Leung, Jean Wilson, Dr. Judith Peranson, Dr. Karen Weyman, Laurie Malone, Dr. Morgan Slater, Dr. Noor Ramji, Dr. Renata Leong, Dr. Rick Glazier, and Dr. Sumeet Khanna.
Footnotes
Declaration of interests Nothing to declare.
Ethical approval This initiative was formally reviewed by institutional authorities at St. Michael's Hospital and deemed to neither require Research Ethics Board approval nor written informed consent from participants.