Article Text

Abstract
Electronic prescribing is a form of paperless prescribing that is reported to reduce prescription mistakes and increases the cost effectiveness of the process. In England, around 1.5 million prescriptions are generated in general practice daily. Thus by reducing costs and increasing efficiency of this system through electronic prescribing, costs can be driven down.
In this Quality Improvement project, a GP practice in London with approximately 3000 patients on record was assessed for its electronic prescribing rates throughout 3 intervention cycles over a period of 2 months. A baseline value of how many patients were already assigned to electronic prescribing was obtained and a period of normal change over a fortnight without any intervention was also assessed (an increase in 15 patients). These values were then used to illustrate any benefits of the interventions completed during the intervention cycles. An introduction of a new electronic prescribing form saw fortnightly uptake rates increase by 20%. The addition of leaflets and posters in the practice produced a decrease of 26% in fortnightly uptake rate. The final intervention included a staff meeting, computer notes to remind staff of electronic prescribing and attaching the new forms to paper prescriptions. This saw an increase in rates of 80% over two weeks. Overall, this project has illustrated that information provision of electronic prescribing needs to be more than just forms or posters. Indeed, the most effective way of improving rates relies on having a driven and motivated staff who are themselves well informed on electronic prescribing alongside adequate information placement for patients to access.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
This project was completed in a GP practice in an inner London borough with 4th year medical students overseeing the project alongside the practice staff. The patient population of the practice encompasses 3084 patients, with the average patient aged between 22-55.
Prior to any intervention, approximately 70% of the patients were utilising paper prescriptions. After discussions with the practice manager and the clinicians, it was evident that reducing the number of paper prescriptions would help manage the finances of the practice into other areas better serving the patients. Electronic prescribing has also been shown to minimise the rate of prescription mistakes.1 By reducing mistakes on prescriptions, patients, the practice and pharmacists would all benefit. Furthermore, patients themselves have an increased flexibility in collecting their prescriptions whether that be close to home, work or a high street as the Electronic Prescribing Service (EPS) can be accessed from any participating pharmacy.
This 2 month project aimed to improve the fortnightly patient uptake rate of electronic prescribing from the baseline value of 15 patients over 2 weeks by 50% to 23 patients with completion in April 2016. During this time, three fortnightly cycles of intervention were implemented and assessed for any changes in electronic prescribing rate.
Background
The Electronic Prescription Service was introduced in 2010 and is expected to fully replace paper prescriptions generated in General Practice in the future. Approximately 1.5 million prescriptions are produced daily in England alone. Furthermore, this figure is expected to increase annually by 5%.2 EPS allows a general practice doctor to generate a computerized prescription for a patient and send that directly to an allocated pharmacy. This pharmacy is chosen by the patient and can be any pharmacy that is part of the EPS. This provides an extremely flexible arrangement for the patient and for those on repeat prescriptions, encourages fewer visits to the practice to pick up a piece of paper. In addition, the issue of lost prescriptions becomes redundant. Furthermore, it was found that in a typical GP setting approximately 7.5% of prescriptions contained an error, however that is bearing in mind that only 1% would incur severe consequences.3 Nonetheless, paperless prescriptions has been shown to drive down prescribing errors.1
Due to the fairly new introduction of EPS in the UK, information regarding its effectiveness in reducing costs, streamlining patient care and reducing prescription errors is lacking. Currently, an EPS costing survey has been completed with the purpose of evaluating the cost and effectiveness of electronic prescribing and is due for release soon. Nevertheless, in case studies from pharmacies in London, electronic prescriptions have already been seen to make up 60%-75% of their prescriptions.4
Inadequate training in usage of computers and EPS has been seen to be an issue with practitioners themselves being reluctant to use electronic prescribing. Electronic prescribing has been shown to initially require a learning curve as practitioners become more familiar with the system. However, once this form of prescribing becomes habitual after adequate training and support, the process of prescribing has been illustrated to be quicker and also less prescription mistakes were also observed.5 ,6
Baseline measurement
Prior to the first intervention, a 2 week control period was used to count the number of patients who nominated a pharmacy under EPS. This information was readily available using the general practice's electronic patient records (EPR). For the following 3 intervention cycles, each also lasting 2 weeks, by using EPR the total number of patients registered for EPS could be seen. Any changes to this number from the previous record could then be calculated and so any improvements could be deduced.
For the first two weeks of the project no interventions occurred and the baseline increase in EPS registrations was calculated. The number of patients who elected to use EPS in this time grew from 1129 (36.4% of the practice population) to 1144 (37.1% of the practice population), an increase of 15 patients over 2 weeks. Our outcome of interest was the fortnightly increase in the total number of patients who elected to use EPS. This was an increase of 1.33% in the baseline period, overall which totalled 15 patients.
Design
In interviews with practice staff, it became clear that there were several barriers to increasing the uptake of EPS. Awareness of the service was poor amongst patients. The busy pace of work meant that clinicians and administrative staff had little time to explain the benefits of the service and the process of opting-in, and there was a paucity of written material to assist with this. The practice had a high turnover of patients as it is within a part of London with a relatively mobile population, meaning that patients would need to be constantly recruited to EPS in order to keep uptake steady. Therefore, the interventions were devised to increase awareness of EPS amongst patients and staff and reduce the workload associated with recruiting the patients to the service.
The practice lacked a formal mechanism for recruiting patients to EPS, relying instead on incidental verbal promotion of the service by clinicians and administrative staff. It was therefore decided that a simple leaflet describing EPS should be designed, including details of nearby pharmacies and a tear-off application form for the service. Further interventions would encircle on visible cues around the practice to attract patients and encouraging staff to be pro-active in registering new patients.
The timescale to implement each cycle of change was mainly constrained by the organisation of the medical school year. It was decided to carry out 4 cycles over a 2 month period, with each cycle lasting 2 weeks.
The project itself was a tool to educate and train staff into providing knowledge about electronic prescribing to the patients. Templates of the new posters alongside the new EPS application form were made available to the practice to ensure long term recruitment of patients to the system.
Finally, after discussion with the clinicians and administrative staff and assessing the baseline uptake of EPS over a fortnight at the practice, it was felt that a fortnightly increase of 50% was an ambitious yet achievable goal. This would translate to an increase from 15 patients registering to EPS (an increase of 1.33%) to 23 patients over a fortnight (an increase of 2%).
Strategy
PDSA Cycle 1 (15th to 26th February 2016) A single simple patient information leaflet including information for nearby pharmacies (location, contact details, walking distances, opening hours) was devised. The leaflet also included a detachable registration form which could be left in a box at reception to minimise queuing for a receptionist. The leaflet was introduced on the first day of the cycle. Uptake increased from 1144 patients registered to 1162, the total patients in the practice now registered to EPS totalling 37.7% (an increase of 1.6%). The increase of 18 patients over this cycle translated to a modest increase of 20% from the fortnightly baseline value of 15 patients. In interviews with practice staff, it was felt that the leaflets greatly increased the ease of explaining EPS and recruiting patients to the service. While staff were very pleased with the leaflets, it was felt that the majority of patients were unaware of EPS and were not asking for information about the service, and therefore fewer leaflets were being handed out. Due to this, the next cycle was centred on promoting the service to the patients and a series of posters were created to display in the waiting areas and consulting rooms.
PDSA Cycle 2 (29th February to 11 March 2016) The aim of this cycle was to assess the impact of the posters promoting EPS to patients. Posters were introduced on the first day of the cycle. Unfortunately, this cycle did not have the impact that was wished for. The number of patients registered to use EPS increased from 1162 to 1173, the total patients in the practice now registered to EPS totalling 38% (an increase of 0.9%). Although there was an increase of 11 patients, this was less than the baseline value of 15 patients. Therefore with regards to our aims, there was an observed drop of 26% from the baseline value. This was a surprising result, and on reflection it was felt that although the posters were very visible, patients would have more confidence in the service if it was directly promoted by clinicians or other staff at the practice. Overall this cycle of intervention was too passive to provide an increase in uptake.
PDSA Cycle 3 (14th March to 12th April 2016) The aim of this cycle was to understand and remedy the reasons for the faltering uptake of EPS. Meetings with staff groups were held to learn more about how to increase enthusiasm for the project and how to promote EPS in the context of a busy general practice. Clinicians asked for a simple prompt to remind them to offer EPS to patients, but they did not want anything that would take up space on their computer screens or otherwise distract them from their patients. Clinicians said they would attach the new EPS patient information leaflets to prescriptions that they gave. Reception staff suggested incorporating a simple tick box within the new patient registration form, and agreed to attach the EPS patient information leaflet to repeat prescriptions. At the end of this cycle, the number of patients registered to use EPS rose from 1173 to 1200, with the total amount of patients registered to use EPS totalling 38.9% (an increase of 2.3%). This increase of 27 patients over the 2 weeks translated to an increase of 80% from the baseline value of 15 patients. Due to the success of this cycle we chose to extend this cycle for another 10 days to assess whether the increased uptake could be sustained. At the end of the second fortnight 1228 patients were registered to use EPS, an increase of 28 new patients. The rate of uptake had held steady and slightly improved to an 87% increase from baseline value of 15 patients.
Results
Our study aimed to use promotional interventions across 3 cycles, each of 2 weeks duration, to improve the uptake of electronic prescribing in a London GP practice. At baseline, the practice had approximately 30% of its patients using electronic prescribing services, with a rate of new registrations being 15 patients every 2 weeks.
We performed 3 cycles of interventions aimed at either the patient or the practice staff. The first cycle saw an increase of 20% (18 patients) from the baseline value of 15 patients. The second cycle saw a drop of EPS registration from the baseline value. The final implementation cycle saw a big increase of 80% from the baseline uptake rate, and this was seen to continue even after the project had come to an end.
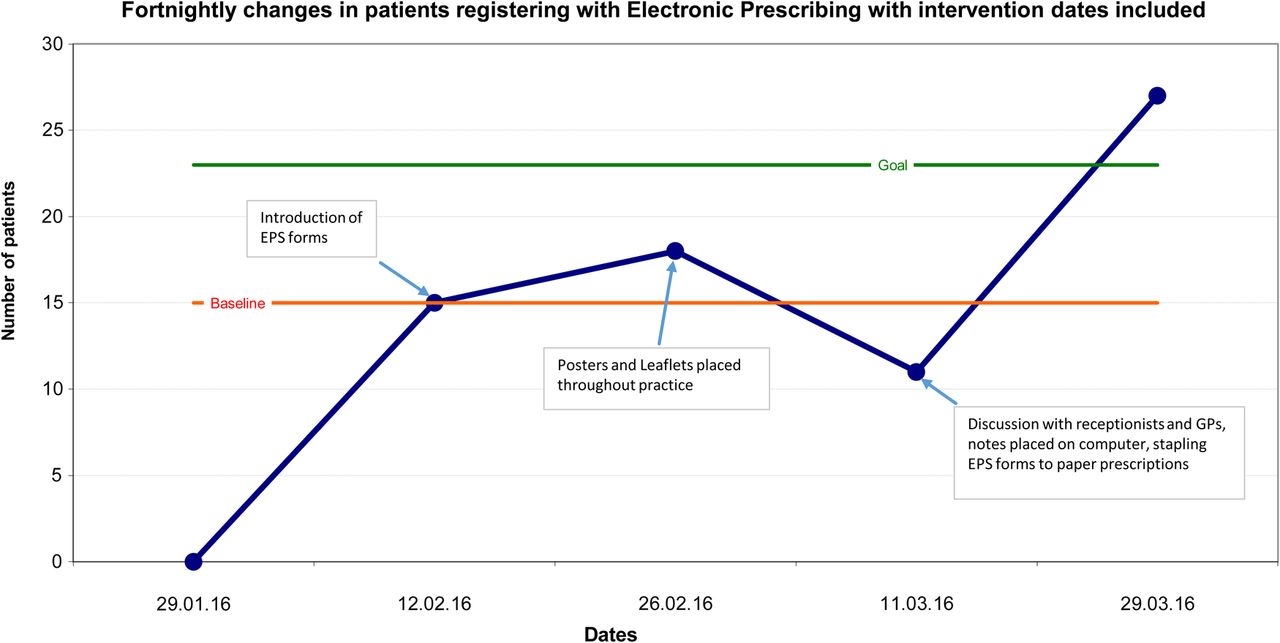
Our study had 4 cycles across a period of 8 weeks, of which the first was without intervention to establish a baseline rate of increase and the subsequent weeks with interventions. During the first cycle, a baseline figure of patients already registered to receive electronic prescriptions was collected and the number of new additions to this figure was assessed at the end of a 2 week period. Over this time, 15 patients opted for electronic prescribing. All information obtained during the project was taken from the General Practice's electronic patient records. The second cycle measured new patient registrations after introducing a new EPS leaflet at the reception desk. Over these 2 weeks, 18 patients signed up to EPS (Table 1, Figure 1). This was a 20% increase from baseline. The third cycle measured new patient registrations after posters were placed throughout the practice advertising the service to patients. This cycle saw only 11 patients registering with EPS, a decrease of 26% from baseline. The final cycle was aimed at encouraging the practice team, applying reminder notices to computer screens, and attaching the EPS form to paper prescriptions. This intervention saw a surge in EPS registrations with 27 new patients signing up over 2 weeks, a baseline increase of 80%. At the end of the project including the extra 10 days to assess sustainability of the project, 39.8% of the practice population were registered for EPS.
{kind=link}
Fortnightly changes in patients registering for Electronic Prescribing with intervention dates included.
Data resulting from each cycle of measurement including subsequent interventions
Lessons and limitations
Multiple challenges were experienced whilst conducting this project. These challenges were largely due to the nature of a student-led project; the time allocation to the project had to fit within other curricula responsibilities. Furthermore, as students are placed throughout South-East England for the majority of the academic year, there were implementation and data collection issues. With these obstacles in mind, the interventions were designed to require minimal student presence in the practice. By scheduling measurements every two weeks, across an eight week period, it was felt that an adequate amount of data could be collected without disrupting the practice and this would also be more feasible with regards to the academic year.
However, this approach did present its own difficulties. Firstly, although the geographical barrier was compensated by the 2 weekly intervals, data collection did prove to be difficult as the actual data was only accessible at the practice itself. Furthermore, as there was no student presence for two weeks between each visit it was difficult to ensure a consistent intervention was being implemented. Indeed each cycle was completely dependent on the actions and cooperation of the staff in the practice; the GPs performed the prescriptions, the administrators uploaded new patients onto the electronic prescribing system and all had a role in patient contact and promotion of the intervention. As the intervention's success was completely dependent on the involvement of the practice staff, successful communication between the staff and the students was imperative.
Due to this dependency upon the staff to promote EPS to maximise patient uptake, knowledge of EPS and the project targets had to consistently be reinforced within the practice. This was done during a meeting every 2 weeks. This approach was limited as the staff team was made up of multiple members who worked on different days of the week. Members not working that day were not present to receive the necessary information. The subsequent effect could have been that these individuals may not have the tools or the motivation to comply with the intervention. A formal education program of EPS for all staff to ensure complete understanding of the benefits provided by EPS and how to access it would also be an improvement to this project as it would add to the motivation of the team.
To improve on this project, a longer time period of assessment would be desirable. Extending the duration with increased frequency of measurement during the baseline period would provide greater insight. The resultant data would allow more accurate comparison against any intervention. Similarly, increased duration and measurement frequency would benefit each intervention cycle, reducing susceptibility to random fluctuations in rates. Greater amounts of data to allow statistical analysis to prove significant benefits of an intervention would improve the robustness of this project. Although these alterations are ideal, one of the greatest limitations was student availability during the intervention cycles. The authors feel this intervention would be best performed by students during a focussed GP placement without other commitments, as is feasible for final year medical students who may be placed in a GP setting for up to 3 months.
The project was designed to increase recruitment of patients to EPS via improving awareness and education of the patients and practice staff. As we spent limited time in the practice and had no patient contact, there was no opportunity for our presence to enter bias into the study. Prior to beginning this project, there was no existing information regarding electronic prescribing readily available at the practice and no formal way of signing up to the system. Thus there were no other incentives increasing EPS registration other than the ones the project put in place. One factor that could have influenced patients of this particular practice to sign up was that there were many local pharmacies part of the EPS. As this would positively skew the results compared to practices where there are not many surrounding pharmacies part of EPS, this could have been a confounding variable. However, the area surrounding the practice is a typical London residential area. To fully appreciate the results of the interventions, it would have been of interest to extend the baseline period to help identify any natural fluctuations in EPS uptake.
With regards to generalizability, this project is limited. The population sample was small and the project was completed over a short period of time. To gain a better idea of how effective these interventions are, this project would need to be completed over a longer period of time on a larger population. However, in essence, there are some conclusions that can be taken from this project and that is that simple measures can improve EPS recruitment and in a short amount of time.
EPS in itself, as it is paperless, is sustainable and more efficient then paper prescriptions. The leaflets, computer notices and posters were cheap and effective measures to put into the practice. To ensure these are utilised after the project is over, templates were left with the practice manager. Although a drawback of the project was the minimal student presence, this did on the other hand illustrate that the recruitment of patients to EPS did not need intensive encouragement. The results show that simple reminders on clinician's computers and leaflets attached to prescriptions made the biggest difference. Indeed when the final cycle was left to continue with no student presence at all, uptake rates continued at an 87% increase from baseline rate. Due to these facts, with the right motivation from staff, it is plausible for this project and the interventions to be sustainable.
Conclusion
EPS is a service that is due to become the main pathway of prescribing and indeed replace paper prescriptions in the future. Thus this project aimed to encourage its usage in a busy inner London General Practice. 3 cycles of intervention were introduced to the practice and assessed for effectiveness. The first two weeks before any intervention was introduced was evaluated to see what the normal baseline increase in EPS usage was. In this time, 15 new patients signed up to EPS and this figure became the baseline rate. Following this, the first cycle of intervention which included a new EPS form saw a 20% increase in EPS registrations from baseline. The subsequent cycle of posters saw a drop of 26% in EPS uptake rate. The final intervention of computer screen reminders and attaching the EPS form to paper prescriptions saw the most drastic increase in the project, an increase in 80% from baseline value.
Overall, the project has been successful and has achieved the goal of increasing fortnightly EPS uptake rates to over 50%. Despite having several challenges to data collection, the project has shown that simple promotional interventions focused on both the patient and the practice staff can increase the rate of patient uptake. This project was undertaken with very simple changes, over a 2 month period and in one GP practice. Therefore, it is difficult to fully extrapolate this data for a UK wide perspective. However, this project is very promising in that it is a proof of principle. It is very fathomable that EPS can be increased quickly, with very simple measures and that EPS can become the mainstay of prescribing. As EPS becomes more common ground in the NHS, patients will become more aware of the service and register for it and so the accompanying implications of benefits to patient safety, cost effectiveness and convenience should also follow.
EPS is a highly benefiting service for the GP practice, patient safety and cost-effectiveness. Problems with EPS have been described in the literature with regards to an initial learning curve and reluctance to use the service. However, these issues have been raised and with adequate training and education these should be easily tackled. As EPS is fairly new, it is expected that with further increases in the uptake of EPS, future problems will be more easily recognised and improved upon. The main concern of EPS which has not been looked at by this project is the downstream effect on the pharmacy with increased workload especially those in closest vicinity to an allocated GP with EPS facilities.
As the electronic prescribing service was only introduced to primary care in 2010, there is not a substantial amount of literature assessing its impact within GPs in the UK and indeed on methods on how to increase patient uptake rates of the service. Therefore it is difficult to fully appreciate how translatable the findings here are. However in a quality improvement project completed in a paediatric unit in Texas, electronic prescribing rates were significantly improved on through provider education on electronic prescribing and changing the way patients were registered; similar findings to this quality improvement project.7 To continue this project, it would be of great interest to try increasing electronic prescribing in a larger GP practice and in a variety of different geographical locations encompassing varying patient populations. During the final year of medical school, medical students can be placed in a GP practice for 8 weeks across England. This would pose the authors of this project an opportunity to perform a similar project to explore these further steps and would also help eliminate the issues of student presence that was faced during this project.
The results gathered from the interventions are sustainable. The interventions relied on simple promotion and enhanced communication; two factors that are recognised as being beneficial and in good use throughout the NHS. As technology improves and cost-efficiency and patient safety becomes further scrutinised, many GP practices are embracing Electronic Patient Records and so Electronic Prescription Services can be taken upon in a similar way. Therefore, many GP practices will be in a similar situation as the studied practice in this project and in an early phase of EPS incorporation. The problems we experienced of communication and time are universal and we feel any further study will benefit from our learned lessons.
Acknowledgments
We would like to acknowledge Dr. Ann Wylie, from Kings College London for continued academic support and to Dr. Jacqueline Bayer, Dr. Jane Livingston and Ms Aneet Garcha for their motivation and drive in our project.
Footnotes
Declaration of interests Nothing to declare
Ethical approval This project was exempt from ethical approval as the work was deemed an improvement study and not a study on human subjects; local policy meant that ethical approval was not required.