Article Text

Abstract
Malnutrition in hospitalized patients is a major cause for hospital re-admission, pressure ulcers and increased hospital costs. Methods to improve the administration and documentation of nutritional supplements for hospitalized patients are needed to improve patient care, outcomes and resource utilization. Staff at a medium-sized academic health science center hospital in the southeastern United States noted that nutritional supplements ordered for patients at high risk for malnutrition were not offered or administered to patients in a standardized manner and/or not documented clearly in the electronic health record as per prescription. This paper reports on a process improvement project that redesigned the ordering, administration and documentation process of oral nutritional supplements in the electronic health record. By adding nutritional products to the medication order sets and adding an electronic nutrition administration record (ENAR) tab, the multidisciplinary team sought to standardize nutritional supplement ordering, documentation and administration at prescribed intervals. This process improvement project used a triangulated approach to evaluating pre- and post-process change including: medical record reviews, patient interviews, and nutrition formula room log reports. Staff education and training was carried out prior to initiation of the system changes. This process change resulted in an average decrease in the return of unused nutritional formula from 76% returned at baseline to 54% post-process change. The process change resulted in 100% of nutritional supplement orders having documentation about nutritional medication administration and/or reason for non-administration. Documentation in the ENAR showed that 41% of ONS orders were given and 59% were not given. Significantly more patients reported being offered the ONS product (p=0.0001) after process redesign and more patients (5% before ENAR and 86% after ENAR reported being offered the correct type, amount and frequency of nutritional products (p=0.0001). ENAR represented an effective strategy to improve administration and documentation of nutritional supplements for hospitalized patients.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
It is estimated that at least one-third of patients arrive at the hospital malnourished. Malnutrition in hospitalized patients is a major cause for hospital re-admission, pressure ulcers, malpractice claims, and increased hospital costs.1 ,2 Fragmented nutritional care and missed opportunities to assess, administer and document prescribed interventions and nutritional supplements in hospitalized patients have been reported in the literature.3 ,4–6 Methods to improve the administration and documentation of nutritional supplements for hospitalized patients are needed to improve patient care, outcomes and resource utilization.7 Nutritional supplements are commonly ordered for patients with malnutrition, increased nutritional demands or high risk for nutritional deficiencies and are effective in improving quality of life, decreasing mortality, decreasing cost, decreasing inflammation markers, and improving nutritional indices.8–10
The setting for this project was an academic health science center hospital in the southeastern United States. The hospital has 1,691 licensed inpatient beds and had approximately 86,000 inpatient hospital admissions in 2015. Staff at this hospital noted that nutritional supplements (oral nutritional supplements (ONS) and tube feedings) ordered for patients at high risk for malnutrition were often inconsistently offered or administered to patients and/or not documented clearly in the electronic health record. This issue has been noted at other hospitals in the U.S. and internationally.3–5 ,11 The current system for administration and documentation of nutritional supplements at our hospital was fragmented leading to errors of omission, communication lapses, missed nursing care and documentation inaccuracies. There were limited methods for healthcare professionals to document ONS administration and assess the administration history in a standardized manner. At our hospital, the nutrition supplement order set was a treatment order set that did not facilitate scheduled administration and documentation of the ONS order. The most accurate method of documenting ONS administration was to administer the product and document the product volume administered in the intake flow sheet in the oral intake row and place a comment in the drop-down box indicating that the product was an ONS product (Ensure, Glucerna, etc). This method was problematic as it did not allow health care professionals to readily know the type, amount and frequency of ONS product given. For example, if 240ml was documented in the intake flowsheet row, it was unclear whether that volume was a fluid consumed with/between meals or it was the ordered ONS product. Healthcare providers often had to speak directly to the patient or nursing staff to ascertain the ONS product they received over the past days in the hospital. Also, the administration and documentation methods did not allow for standardized documentation if the product was not given and what the reason for the non-administration was. For example, if the ONS product was not given, generally it was not documented and/or it was documented on a progress note not linked to any order.
The SMART Aims for this project include: AIM #1: By December 2015, administration of oral nutritional supplements will increase by 25% compared to baseline administration rates. AIM #2: By December 2015, the percentage of formula returned to food and nutrition services will decline by 25%. AIM #3: By December 2015, documentation of administration (given or not given) of oral nutritional supplements will increase to 100%.
Background
Improving patient nutritional status has the potential to improve quality of patient care, clinical outcomes and reduce costs. The benefits of oral nutritional supplement (ONS) use on improving key clinical outcomes are well documented in the literature and include: reduced complication rates [falls, infections, pressure ulcers, anemia, and cardiac complications], length of hospital stay, readmission rates, costs of care, and mortality rates.12–14 A study published in the American Journal of Managed Care reported that patients who used oral nutritional supplement (ONS) had a shorter length of stay by 2.3 days, decreased episode costs, and reduced 30-day readmission rate compared to a matched sample that did not use ONS while hospitalized.15 In a Dutch study, malnourished long-term care facility residents who received nutritional interventions had a lower risk of falls.16
The Agency for Healthcare Research and Quality reports that medication errors are one of the most common types of inpatient errors. A medication error refers to an error (of commission or omission) at any step along the pathway that begins when a clinician prescribes a medication and ends when the patient actually receives the medication.17 All prescription medications, herbals, vitamins, nutritional supplements, over-the- counter drugs, and others should be included in the medication reconciliation process, however many hospitals do not administer and document nutritional supplements in the same process as other prescribed medications.18 In many hospitals, nutritional products, like ONS and tube feedings, are treatment orders and are not included in the medication order set or medication administration record (MAR) and there are often fragmented limited methods to document administration or non-administration by nurses. Therefore, dietitians, physicians, nurses and other health care providers have difficulty determining administration history of ONS, other than patient, family or nurse report or incidental documentation in the intake/output record. Further, the health record allowed nurses to document the intake of oral fluids (in mL) but did not allow for an efficient method for determining the type of fluid the patient received. Therefore, it is difficult for health care providers to have a clear picture as to the patients' compliance with the ONS, if they consumed the product, and/or reasons why they did not consume the product.
Hospitalized patient compliance with nutritional supplements has been inconsistent in the literature. One study reported compliance with prescribed nutritional supplements was low in hospital and in the community and that only 43% of the study population consumed more than 80% of the prescribed amount.19 A systematic review of 46 studies revealed a mean compliance rate of 67% in hospitalized patients with prescribed ONS orders.20 However, in our hospital on a random one-day review of the formula room return rate of ONS products, we found that 75% (90 returned products/out of 119 products) were returned unused to the formula room indicating that we had a significant problem with administration and compliance for our patients.
Hospitalized patient compliance with nutritional supplement orders is a complex, multifaceted issue. Through a review of the current literature concerning ONS, the literature reveals trends in factors that either decrease or improve consumption and administration of ONS. According to the literature, there were many factors affecting patient compliance such as flavor, taste, texture, predictability of supplementation, and offering variety.19 Encouragement by caregivers and an appropriate ambiance were also noted as factors improving compliance for older adults living in nursing homes. The top factor most often noted in improving compliance was administration of high protein, energy-dense, and with special emphasis on low volume formulations which resulted in significantly higher ONS and total energy intakes.21 Some studies described that these formulations should also be nutrient rich and supplemented with fiber. Not only did these formulations increase compliance, but they were also positively associated with improved nutritional status in nursing home residents.22 Dietary counseling/patient education was also noted as being a factor in higher compliance with ONS. In one study looking at ONS consumption rates of radiotherapy patients, results showed that dietary counseling sustained significantly higher rates and impacts on patient outcomes than other methods had even three months after radiotherapy.23 Another study reviewed many factors influencing ONS consumption and concluded that compliance was more highly related to the information given as well as the will of the patient. This study advised that more emphasis should be placed on the importance of ONS consumption through specific patient education.24 Although the articles reviewed gave much insight into patient compliance factors to ONS, further research examining other common and suggested methods to improve ONS consumption is necessary in improving compliance rates and consequently improving nutritional status of residents.
In addition to reviewing factors that influence patient compliance with ONS, research has been conducted to review factors that affect health care professionals' (HCPs) compliance in prescribing ONS. One study that was unable to identify a single significant factor in ONS administration concluded that: “Health care professionals have a wide-range and different views on criteria used to prescribe ONS and factors affecting their subsequent intake”.19 Despite the wide-range of views that HCPs have on this matter, the most significant factors listed in other studies were specificity of the ONS order, time of delivery of ONS, and education on ONS administration as well as emphasis on its importance. One study revealed that initiation of nutritional support was delayed in critically-ill obese patients compared to normal or underweight patients.25 In a study conducted to observe nursing home staff delivery of ONS products to residents with ONS orders, results showed that ONS delivery times are not consistent with the orders given and that staff spent little time promoting consumption of ONS to their patients.26 Interventions tested by other studies to improve the issue of inconsistent times of delivery showed that establishing a distinct supplement administration round and signage above the beds of patients who needed assistance with ONS consumption resulted in higher compliance rates.27 In regards to improving staff education, another study revealed that a nutrition education program resulted in higher compliance rates as shown in screenings performed six months and one year post-intervention. It was noted that one year after the intervention, screening for malnutrition risk was better, dietary advice was given more often, and ONS was prescribed for a greater number of patients who were at risk for malnutrition than before.28 Based on the improved rates of compliance from these studies, education to staff on the importance and basic administration guidelines of ONS can positively influence the rates of compliance as well as the efficiency and vigilance of staff in appropriately administering ONS to patients who need them.
In evaluating the problem, we looked to the literature to identify if any solutions have been proposed for this problem or other errors of omission of ordered medications or products. A study published in the Journal of Nursing Care Quality described an approach where nutritional supplements were given as scheduled medications and they found pressure ulcer incidence, length of stay, 30-day readmissions and costs of care were reduced.11 Similarly, a quality improvement study reported a process improvement project that improved the rate of errors of omission of insulin by 54% by adding scheduled standardized order sets, extensive nursing staff education, and enhanced efficiency of the existing process.29 Because of the positive findings of both of these studies, our team decided to redesign our current process and add nutritional supplements to the medication order sets in the electronic health record and medication administration record (eMAR). Further, we created a tab within the EMAR that was focused on nutritional medications. In the EMAR, prior to redesign, we had tabs for all, scheduled, as needed (PRN), respiratory, continuous, chemotherapy medications.
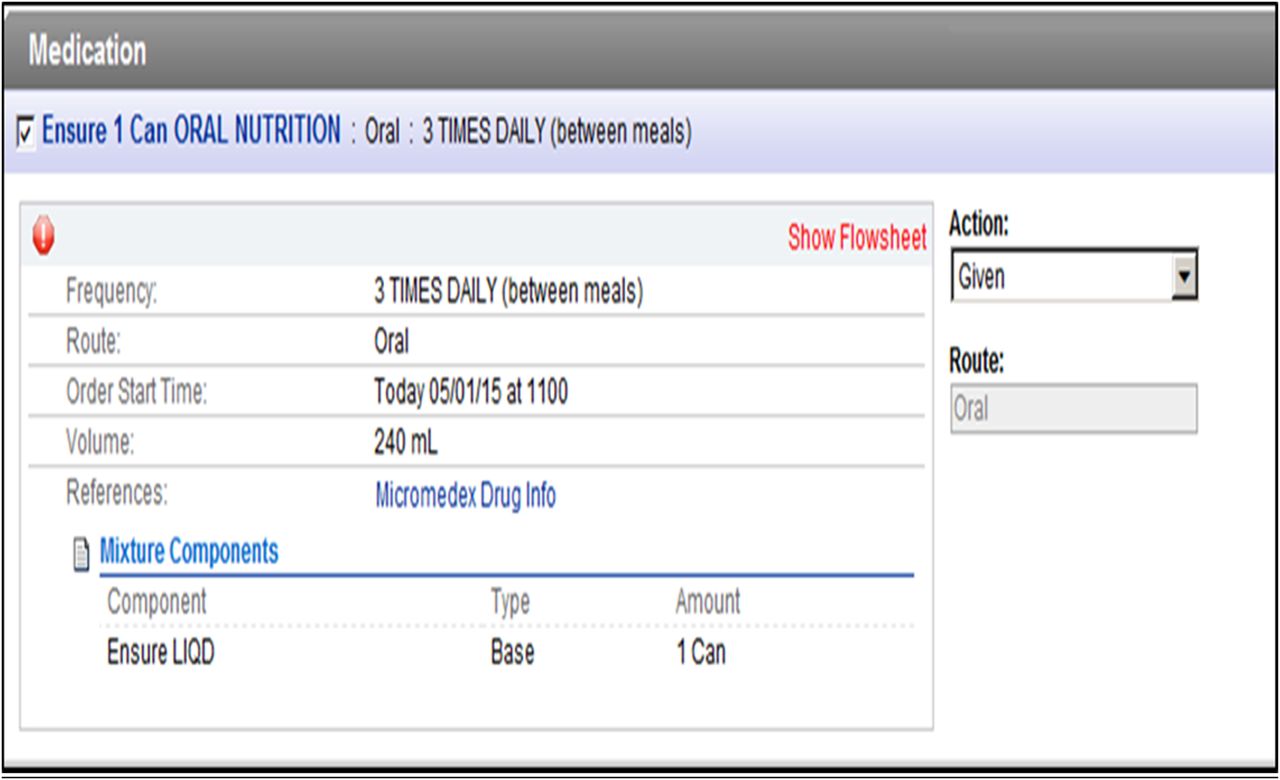
By adding the ONS order to the medication order sets and adding an electronic nutrition administration record (ENAR) tab, we sought to standardize nutritional supplement ordering, documentation and administration at prescribed intervals. Additionally, nurses would be prompted in the ENAR to document the administration (or non-administration) of the ONS and this would improve provider communication and medication safety to accurately reflect administration or non-administration and the reasons why the patient did not receive the nutritional medication.
Baseline measurement
The project began in August 2014 and the multidisciplinary nutrition improvement team met weekly to plan and implement the project. Baseline evaluation of the state of administration and documentation of ONS was done in November-December 2014. A total of 124 patients were surveyed during the 4 day prevalence period (pre-process change). The units included were 2 medical units and 2 oncology units. Out of 124 original patients, 111 patients were included in the analysis. 13 patients were excluded from the analysis because they were discharged or their ONS orders were changed by the time of the interview and medical record review. Results for baseline evaluation include the following: a total of 85,920ml ONS products were delivered to these patients to be consumed and 4,675ml (5%) of ONS was documented as consumed (with comments that it was ONS) in the intake flowsheet of the patient medical records. 80% (N=93) of patients did not accurately know the amount and frequency of ONS product they were ordered. 48% (N=45) of patients interviewed reported not being offered ONS during the previous hospital day. 83% of patients reported that if they were offered ONS, they accepted it. 17% of patients reported that if they were offered ONS they declined to accept it due to various reasons (nausea, did not like it, did not feel well, etc). 96% of patients were not offered the correct type and amount of ONS products. The most frequently reported reason for patients not consuming the ONS product was that “it was not offered to the patient” (54% of patients reported this as the reason they did not consume the product in the ordered amount). The second most frequent reason was that the patient either “was not feeling well” or “was nauseous” (12%).
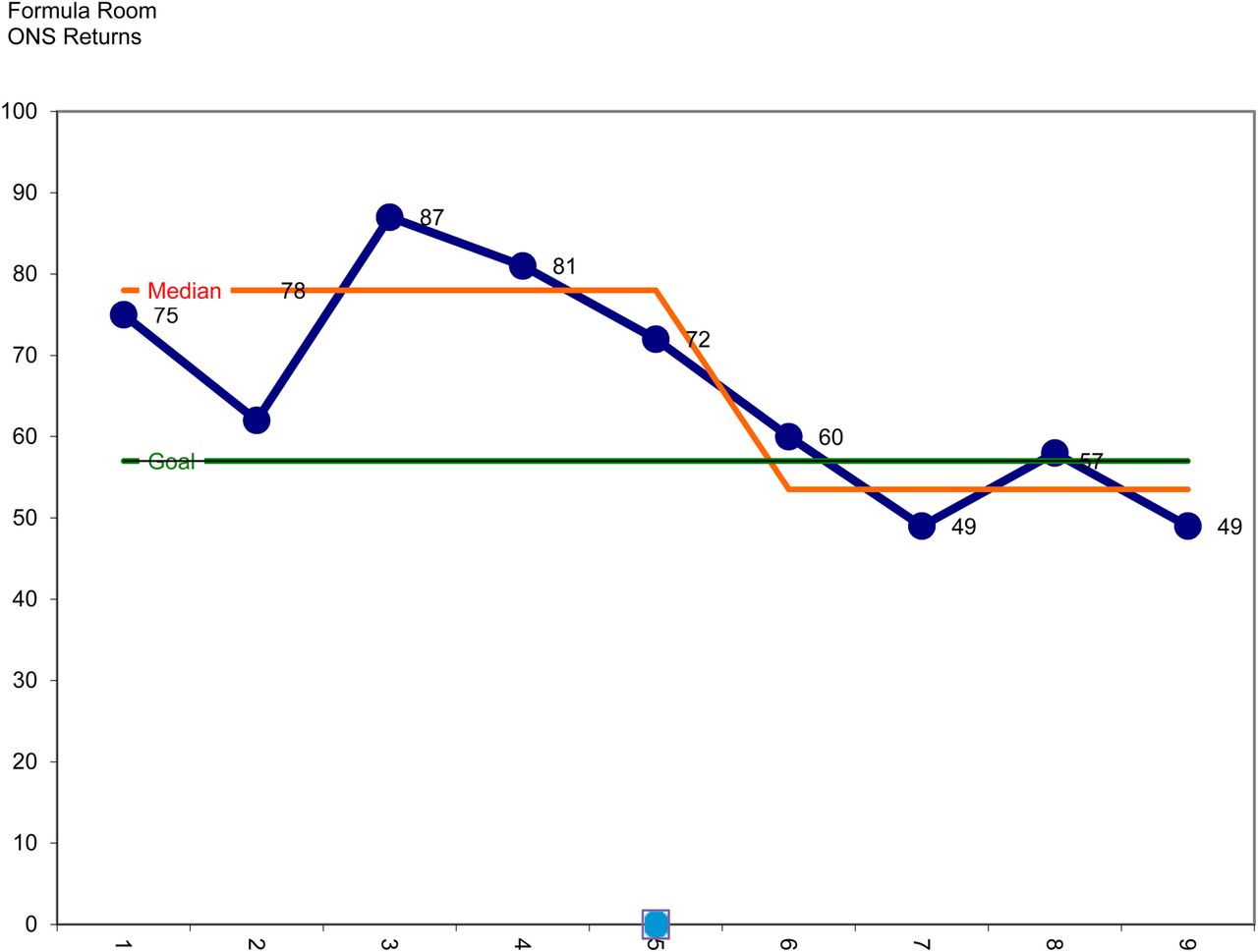
The mean return rate for ONS formula at baseline was 76% (range: 62-87%) returned over a 4-day period, meaning that on average only 24% of ONS products were potentially consumed by patients and 76% of them were returned to the formula room unopened. This data informed our next steps in that we became even more convinced that a process change needed to occur to improve the administration and documentation of ordered nutritional supplements.⇓⇓⇓⇓
Formula Room ONS Returns (Baseline)
Implementing ENAR to Decrease ONS Returns
ONS Administration and Documentation Improvement Project (ENAR) – PDSA
{kind=link}
{kind=link}
{kind=link}
Electronic Nutrition Administration Record (ENAR) Administration Screen (EPIC)
Design
The baseline data collection showed that there was a significant problem with administration of ONS for hospitalized patients as an average of 76% of ONS products were returned to the formula room unopened following the 24-hour periods that they should have been consumed. The multidisciplinary team met to develop a plan and met with administrative and clinical stakeholders to get commitment to go ahead with the project and provide resources (personnel, time, money, etc). The team initially included the Director of Dietary Services, clinical nursing faculty, and critical care nurse leader and critical care physician. Because we intended to modify the electronic health record (EPIC system), we added informatics professionals and clinicians from nursing, medicine, nutrition, pharmacy and quality and patient safety departments. We also included a statistician to assist with planning and establishing our aims, methods and measures. We had smaller meetings with portions of the team that impacted different areas and often had larger meetings with the entire team. Communications via email and by telephone were also important in facilitating the project moving forward. We identified aims at the initial onset of the project and wrote a proposal and contract that all stakeholders in the health science center signed.
The team searched Pubmed, Health Science Center databases, Google Scholar and internet searches to identify current evidence and literature regarding the state of administration and documentation of oral nutritional supplements in hospitalized patients. We used key search terms such as: oral nutritional supplement administration, documentation, compliance, electronic health record, and nutrition supplement administration strategies. The team met with stakeholders located on inpatient units not directly associated with the process improvement team (staff nurses, pharmacists, physicians, dietitians, hospital administrators, and hospital directors) to assess the current process of how nurses administer and document nutritional supplements and how physicians, nurse practitioners, physician assistants, and dietitians assess, order and evaluate them. A process flow pattern for hospital staff was identified and then a new process redesign was created based on the new system. We met with the team weekly via in-person meetings and via email and formulated ideas to improve the existing electronic health record and create new medication order sets to be used for nutritional supplements. The team reached out to peer institutions, users and administrators nationally who utilize similar EPIC health record software system to identify best practices and solutions. The team met with hospital administration and councils on quality and safety to assure the process redesign was supported by hospital administrative and technical resources, there were no concerns as to patient and quality issues in the planning of the process change, and the project was in-line with overall health system goals and strategic mission. A process redesign strategy that focused on creating new medication order sets that included nutritional products was decided upon after careful review and deliberation by all stakeholders involved. The new nutritional medication order sets included all nutritional products (including oral liquid supplements, protein powders, miscellaneous nutritional supplements and tube feeding formulas). This paper describes only the oral nutritional supplement measures however the process redesign involved improvement of all nutritional supplement categories, including tube feedings.
The project team met weekly during the planning stages and the IT team worked to create, build and test the order sets and administration and documentation screens in the EPIC system. The project team worked to identify risks associated with this implementation and any risks identified were reviewed and strategies implemented to manage them.
There was some initial resistance to add nutritional supplements to the medication administration record (MAR) due to concerns that this might add to errors or increase the length of the MAR. Ultimately, it was decided to add the nutritional supplements to the MAR to decrease medication errors and improve administration and documentation of these nutritional medications. Prior to implementation of the new system, staff education and training was carried out in multiple sessions to assure that all staff (nurses, patient support techs, nursing assistants, physicians, physicians assistants, nurse practitioners, dietitians, pharmacists) knew the new process for ordering administering and documenting nutritional medications. The project was undertaken from August 2014 to December 2015, with implementation of new process occurring July 2015.
Our data collectors included one Registered Dietitian, one doctoral-prepared clinical nursing professor (ARNP), four undergraduate honors nursing research assistants, and one Registered Nurse who is also a second-year PhD in nursing student. This process improvement project used a triangulated approach to evaluating pre- and post-process change including: medical record reviews, patient interviews, and nutrition formula room log reports. PDSA cycles were completed during the planning and implementation of the intervention and post-implementation of the ENAR to improve the administration and documentation outcomes after process change.
Strategy
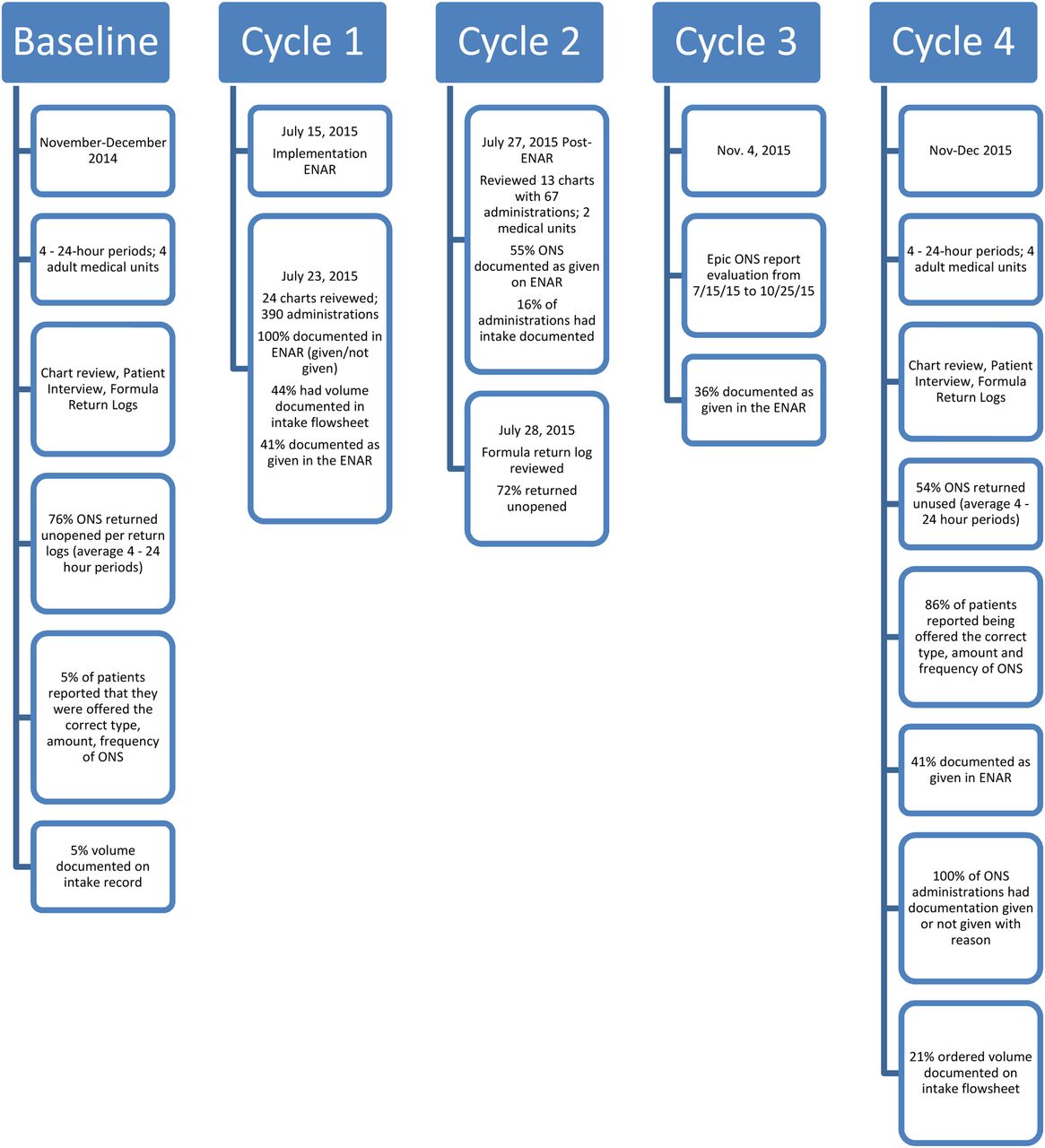
PDSA Cycle1 (July 2015): This phase included analysis, planning, building, testing, training and implementation for new ENAR system and ONS ordering, administration and documentation process. A new process of ordering, administration and documentation was introduced in the electronic health record (EHR) (Epic EHR system) and implementation for the ENAR was July 15, 2015. The aim of this cycle was that both administration and documentation of ONS will be improved after ENAR compared to baseline. Hospital staff (physicians, nurses, dietitians) were educated via email blasts, live group training sessions and 1:1 training in early July 2015 and on July 15, 2015 the new ENAR system went into effect in our hospital for adult inpatients. Approximately 1 week after the new process change and ENAR implementation, quality improvement reviews for random patients on 4 inpatient units at the hospital was done by informatics staff to assess the effects of the ENAR on administration and documentation of ONS. Twenty-five ONS orders were reviewed. Out of 25 individual ONS orders, 11 (44%) had volume documented in the correct area on the intake flow sheet. 14/25 (56%) did not have volume (mL) documented in the intake row of the medical record. Of those 25 orders, there were 390 total administrations (given or not-given). 390/390 (100%) had documentation of either given, not given or held. 159/390 (41%) were documented in the ENAR as being “given” to patients. 231/390 (59%) were documented as “not given”.
PDSA Cycle 2 (July 27-28, 2015): The aim of this cycle was that a greater percentage of formula would be recorded as “given” in the ENAR, a greater percentage of volume would be recorded in the intake record of the flowsheet and less formula would be returned to the formula room unused. Chart reviews on all patients with ONS orders on 2 medical units revealed 13 charts with a total of 67 ONS administrations. 37/67 (55%) ONS administrations documented as “given” on ENAR. 16% of administrations had volume of intake documented in the intake flowsheet. Formula return logs for a one day period were reviewed to determine the amount of unused products returned unopened. A 72% return rate was found for ONS products over a one-day period. Based on this data, more education for staff via email tip-sheets, 1:1 nurse education at the computer on the correct process of documentation of intake volume, nurse manager follow-up and providing feedback to nursing staff was done. Recommendations to include a link to the intake flowsheet row directly on the administration screen (instead of having to go to a separate flowsheet tab) was provided to the IT department.
PDSA Cycle 3 (November 2015): As a follow-up to see the effects of the ENAR on administration and documentation, a report was created and generated by the informatics team to include the number of ONS administration actions, % given, and % not given. We found a total of 9,874 ONS product administration entries for the period between 7/15/15 to 10/25/15. We found that 36% (3,585/9,874) were documented as “given” in the ENAR and 64% (6,289/9,874) were documented as “not given”. This data was shared with the team and additional staff education and training was given via email tip-sheets, nurse manager followup and 1:1 nurse training.
PDSA Cycle 4 (November-December 2015): A similar approach as was done at baseline evaluation of ONS administration and documentation was completed in November-December 2015, four months post-ENAR implementation. Adult inpatients on four medical units with ONS orders were interviewed and their medical records reviewed to evaluate administration and documentation of ONS products. For this post-process change evaluation, a total of 102 patients with ONS orders were surveyed during the four day period, over four weeks (post-MAR process change) with 59 patients having complete data and able to be interviewed. At baseline, a total of 85,920ml ONS products were delivered to these patients to be consumed and only 4,675ml (5% of total) of ONS was documented as consumed (with comments that it was ONS) in the intake flow sheet of the patient medical records. Post-ENAR, 56,955ml ONS products were delivered to these patients to be consumed and 11,812ml (21% of total) was documented in the intake flow sheet. At baseline, the mean return rate for formula was 76.25% returned over 4 day period. After the process change, the mean rate of returned ONS products over the four day period was 54%, signifying a decrease unused return rate by 23%. Further, documentation in the ENAR showed that 41% of ONS orders were given and 59% were not given. If the nutritional medication was not administered, the nurse indicated the reason using a drop-down box with option. Reasons for non-administration included: patient refused (72%), other reason/contraindicated (21%), NPO status (5%, and medication not available (3%). After the ENAR implementation, there was statistically significant improvement in patient knowledge of amount and type of ONS ordered (p=0.0001). Further, more patients reported being offered the ONS product (p=0.0001) and more patients (5% before ENAR and 86% after ENAR were offered the correct type, amount and frequency of ONS (p=0.0001). When asked is they generally liked the ONS product they were ordered, 72% of patients interviewed reported that they generally like the product while 28% reported that they did not like the product. 54% of patients reported being educated about their ONS and 29% reported no education about their ONS products, while 17% could not recall if they had received education about their ONS orders or reasons for ONS. Of the patients who reported receiving education, 76% of them reported that the education increased the likelihood that they would take ONS in the future and 69% of those educated reported that the education influenced them in taking ONS at home after discharge from the hospital.
Results
After the initiation of the ENAR, patients were significantly more knowledgeable about their ONS orders (p=0.0001), they were offered ONS more (p=0.0001), they accepted it more (p=0.0001), and they were offered the correct type, amount and frequency of the products more (p=0.0001). The formula room returns decreased from a mean of 76% to 54% after the process change, meaning 46% of ONS products were utilized on the unit for patients. The electronic health record documentation also reflected improved intake documentation, increased from 5% before to 21% after, although this was still under-reported based on the MAR documentation. MAR documentation revealed that 41% of ONS ordered products were given and 100% of orders were documented as given or not given. If orders were not given, reason for non-administration was documented in a drop down box by nurses.
SMART AIM #1: By December 2015, administration of oral nutritional supplements will increase by 25% compared to baseline administration rates. The results of this project showed that 5% of the ordered volume was documented in the intake record as administered. However, this number is speculated to be lower than actual patient consumption due to the fact that 23% of the products were not returned so they may have been consumed. The administration of ONS rate was at maximum an average of 23% administered over multiple (4) 24-hour periods based on the formula room returns at an average of 76.25% over this same period. After the process change, the intake documentation showed that 44% of administration records had at least some volume documented in the intake record and overall 21% of the ordered ONS volume was documented as consumed in the intake records that were evaluated.
SMART Aim #2: By December 2015, the percentage of formula returned to food and nutrition services will decline by 25%. To reach this goal, formula returns needed to decrease from baseline to at least 57%. The percentage of formula returned before the process change was 76% and after the process change it was to 54% unused, indicating a 29% decline over time.
SMART Aim #3: By December 2015, documentation of administration (given or not given) of oral nutritional supplements will increase to 100%. Before the process change, documentation of intake of ONS was 5% of the total volume ordered and there was no consistent method for documentation of administration or non-administration of ONS in the medical record. After the process change, 21% of of all volume ordered was documented in the intake flow sheet, indicating an improvement by 16% from baseline. Post-ENAR, 100% of orders had documentation indicating administration (given or not given with reason) in the nutritional medication administration record. Forty-four percent of orders had at least some volume documented in the administration area, indicating that nurses provided the patients with at least some volume during 44% of the administration attempts.
Lessons and limitations
Many lessons were learned during this project. We learned the importance of working together in a multidisciplinary team. We found that frequent team meetings (in-person and teleconference) were helpful in troubleshooting problems, identifying barriers and planning solutions, and getting stakeholder by-in and input. During the implementation phase, we had multiple daily conference calls for the first week of implementation to assure a smooth transition and troubleshooting of problems. For example, initially ENAR built was routed through the pharmacy which resulted in added workload for pharmacists as nutrition orders and changes made to rate appear in pharmacist work queue for verification similar to medication workflow. The IT team was able to build an alternative path that bypass pharmacy altogether and that improved staff by-in, efficiency and work flow. Additionally, the dietitian department assisted on the morning of implementation day by inputting new order sets for existing patients so that physicians and ordering healthcare professionals could quickly write new orders for existing patients using the new order sets. This allowed for a smooth transition of the use of the new order sets. In terms of limitations, our results could have been due to chance/random fluctuations in ONS consumption patterns by patients and/or administration and documentation by nursing staff. Going forward, we need to continue to evaluate patterns in administration and documentation of ONS; specifically looking for ways to improve the documentation of intake of ONS for hospitalized patients. One solution is to have a linked tab during the administration process that automatically allows the nurse to input the ONS volume into the flowsheet record. This was unable to be fully accomplished with our process redesign due to the limitations of the health record system capabilities. Other health systems planning a similar transition to eNAR should consider linking the volume administered directly to the intake flowsheet to decrease steps of documentation process and improve documentation accuracy. Since this process redesign, our health system has implemented similar ENAR system at the mental health hospital, rehabilitation hospital and pediatric inpatient units in our health system.
Conclusion
Errors in omission of nutritional supplements was found to be a significant problem at our hospital. We found that an average of 76% of products ordered were returned unopened and 5% of the ordered volume was documented in the intake record of the electronic health records with comments that it was ONS. We found that 96% of patients interviewed were not offered the correct type, amount or frequency of the ONS product that was ordered them on the study days. The most frequently reported reason why patients did not accept the ONS product was because “it was not offered to them”. A process redesign was initiated in July 2015 that changed the way that nutritional supplements were ordered, administered and documented. The nutrition order set was changed from a treatment order set to a medication order set and included in the medication administration record (MAR) with a separate nutrition administration record tab (ENAR). Prior to and after the implementation of the new process, extensive staff education was performed via email blasts and live training sessions.
Improved patient and financial outcomes are seen with ONS use by hospitalized malnourished patients. According to calculations based on Phillipson, et al. (2013), for every 1% increase in patients provided ONS, an average hospital can save $929,000. 15 In our system, we improved the administration by at least 16% according to the intake flowsheet records. This could indicate a substantial cost savings for healthcare systems and patients. This study underscored the need for improved administration and documentation systems to enhance nutrition assessment and interventions. The addition of nutritional products to the medication record has the opportunity to improve medication reconciliation, patient education, use of healthcare resources, administration of ONS, and communication among health care providers and patients.
Acknowledgments
The authors would like to acknowledge the University of Florida College of Nursing, the University of Florida Health System and the W. Martin Smith Interdisciplinary Patient Quality and Safety Awards Program for the support of this project. The authors would like to acknowledge the statistical support from Mr. Gared Garvan and research assistants Samantha Smith, Kate Krause, Amber Bart, Shannon Dunne, and Zandra Christopher Wingfield.
References
Footnotes
Declaration of interests None declared.
Ethical approval The academic health science center's institutional review board approval was obtained prior to beginning the study.