Article Text

Abstract
“Early Aspirin” or a medium dose of aspirin 6 hours after Coronary Artery Bypass Graft (CABG) Surgery is strongly recommend by international guidelines (EACTS 2007/AHA 2011 guidelines, Level1a evidence) to protect venous graft patency. However, compliance with Early Aspirin prescription at our centre is poor due to long standing hospital cultural practices and lack of awareness.
We completed a two-cycled retrospective audit of 53 (September 2015 Baseline), 65 (January 2016 First Cycle) and 58 (June 2016 Second Cycle) consecutive CABG patients. Interval interventions included educational presentations, educational leaflets/posters, pharmacy liaison and modifications to e-prescription order-sets. Medical, nursing and pharmacy staff were involved in the audit strategies. Early aspirin prescription improved from 23% to 48% to 55% while administration of Early Aspirin improved from 17% to 38% and finally to 48% by second improvement cycle. Significantly, the proportion of patients with omission of early aspirin despite a clear clinical indication, decreased by 50% over the audit period. Important practical considerations were the last dose of anti-platelets preoperatively and amount of of bleeding from mediastinal drains post operatively. A multidisciplinary team based approach led to a 139% improvement in prescription and 182% improvement in administration of “Early Aspirin” after CABG surgery.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Anti platelet therapy is a crucial part of post-operative management of patients undergoing cardiac surgery. The leading indication for aspirin post cardiac surgery is to reduce the incidence of vein graft occlusion after CABG (coronary artery bypass graft) surgery. There is Level 1a evidence that administration of “early aspirin” (defined as 300mg of aspirin within 6 hours post surgery) after CABG improves early and late saphenous vein graft patency, and results in a survival benefit. Early aspirin is strongly recommended by the European Association of Cardiothoracic Surgeons 2007 Guidelines and the American College of Cardiology 2011 Guidelines. 1 ,2
At present we do not have any institutional guidelines at our centre regarding early aspirin post CABG surgery. At our 187-bed specialist cardiothoracic centre, we perform just under 2000 adult cardiac surgery cases per year. Hence, appropriate Early Aspirin prescription post CABG surgery is crucial. However, due to lack of awareness, long standing hospital culture and technical problems with electronic prescriptions, there has been poor adherence to international guidelines. This audit identified that only 23% of patients were prescribed a loading dose of “Early aspirin” at baseline measurement and we aimed to improve this to 70%. Additionally, 66% of patients had lack of Early Aspirin administration despite clear indication for it. We aimed to identify clinical reasons for deviation from guidelines and reduce inappropriate omission of Early Aspirin despite clear indication for it to less than 20%.
Background
A meta analysis of 20 trials including more than 5000 patients who had had coronary artery bypass grafting, concluded that anti-platelet therapy was associated with prevention of occlusion in 92 (SD 15) patients per 1000 (21.1% of anti-platelet allocated patients versus 30.3% of corresponding controls).3 In a multi centre prospective cohort study, CABG patients treated with aspirin within the first 48 hours postoperatively had a lower incidence of postoperative myocardial infarction (2.8% vs. 5.4%, P < 0.001), death (1.3% vs. 4.0%, P < 0.001) and relative risk reductions of acute kidney injury, stroke and bowel ischemia compared to patients who did not receive aspirin.4 However, aspirin does not seem to improve graft patency if started more than 72 hours after CABG surgery and meta-analysis has shown the optimal reduction in odds of venous graft occlusion if a medium dose of aspirin is given 6 hours post operatively.5
The European Association of Cardiothoracic Surgeons 2007 Guidelines and the American College of Cardiology 2011 Guidelines recommend that a medium dose (150-325mg) of Aspirin should be administered within 24 hours post CABG surgery.1 ,2 There is a trend towards improved outcomes with earlier administration and giving aspirin at 6h is agreed as the optimal strategy that best balances bleeding risk versus survival benefit. Systematic review has recommended that a ‘fail safe mechanism’ for prompt post operative aspirin should exist.6 Though current evidence for improved clinical outcomes is only limited to saphenous venous grafts, guidelines recommend that Early Aspirin be given to patients with arterial grafts as well.
Baseline measurement
Data was collected retrospectively from the Electronic Patient Record System. Data from consecutive patients who underwent elective or urgent isolated Coronary Artery Bypass Graft Surgery with or without cardiopulmonary bypass was collected in the following arbitrarily selected period: Baseline- 27.08.2015 to 20.09.2015 (53 patients). The primary outcome studied was the proportion of patients who received Early Aspirin post CABG.
Pre-operative, intra-operative and post operative variables that could influence clinical decisions were documented. These included the last dose of pre-operative anti-platelet drugs, factors associated with an increased risk of bleeding/clinical risk such as: intra-aortic balloon pump (IABP), past history of bleeding from abnormal sites, peptic ulcers or known bleeding disorders. Intra operative considerations such as bypass or off pump surgery and nature of grafts used was documented. Early post operative complications such as resternotomy, excessive bleeding from mediastinal drains, clinical suspicion of cardiac tamponade were acknowledged to account for practical deviations from guidelines.
Out of 53 patients in the Baseline measurement, only 23% of patients (12/53) had a prescription for a 6 hour loading dose of aspirin. Furthermore, only 17% of patients (9/53) were actually administered the prescribed loading dose of Aspirin. 6/9 patients received aspirin within 6 hours, 3/9 of these patients had a delayed administration of 300mg aspirin (up to <12 hours post operative). Of the remainder 3/12 patients with prescriptions, 1 patient's dose was withheld due to clinical reasons of ‘excess bleeding’ in drains and 2 patients had an incorrect prescription.
On review on relevant preoperative factors – 9% (5/53) of patients had received a regular dose of 75mg aspirin on the morning of the day of the operation (D0). None of the patients had pre-operative conditions associated with increased risk of bleeding but 1/53 patients had a documented allergy to aspirin. 3/53 (6%) patients had early post operative complications. 1/53 patients needed a resternotomy, 1 patient had a PEA arrest and 1 patient was reported to have ‘excessive bleeding’ from drains but this did not meet resternotomy thresholds and later settled.
Design
As a foundation doctor rotating in ITU, reviewing post operative CABG cases was a routine part of my job and it was clear from Baseline results that there was poor compliance with guidelines on Early Aspirin. I discussed my aim to improve the primary outcome, that is, increase the proportion of isolated CABG patients who are administered Early Aspirin 6 hour post operatively, with my Anaesthetic/Intensivist Consultant. We decided to study our local practice in further detail to identify the unique limitations that might be specific to our centre.
Firstly, colour coded zones to classify clinical practice were defined as follows:
RED ZONE: Omission of 6 hour Early Aspirin in patients despite clear indication of Early Aspirin. These patients had received their last dose of regular low dose pre-operative aspirin >24 hours prior to the operation, with no clinical pre-operative conditions/factors associated with increased risk of bleeding and developed no early post-operative complications.
GREEN ZONE: Omission of 6 hour Early Aspirin in patients who might have an acceptable clinical reason for this. Probable reasons include continuation of regular dose aspirin including D0 pre-operatively, loading dose of aspirin <24 hours pre-operatively, presence of pre-operative factors that suggested an increased bleeding risk or early post operative complications.
On further study it was evident that 66% (35/53) of patients in our baseline measurement were in the RED Zone, that is, they did not receive Early Aspirin despite it being clearly clinically indicated. The reasons for omission in the above patients was a lack of a prescription in 62% (33/53) of patients and an incorrect prescription in 4% (2/53) of patients. Thus, the leading limiting factor was shown to be a lack of appropriate “Early Aspirin” electronic prescriptions.
The baseline results were discussed informally with cardiothoracic consultants, registrars, critical care nursing staff and pharmacy staff to understand baseline knowledge, prevalent opinion on early aspirin, and to invite suggestions for suitable interventions. Discussions with cardiothoracic surgeons helped establish that in a few instances there seemed to an information technology error and aspirin suppositories thought to have been prescribed were not visible on the ‘worklist manager’ or e-medication chart. However, the major reason for paucity of prescriptions was a hospital culture that did not specifically promote Early Aspirin prescription and a natural inertia to changes in long-standing practice. Three areas for corrective measures were identified as follows:
Increasing awareness among medical staff and highlighting deficiencies in practice.
Correcting information technology (IT) system errors.
Education on Early Aspirin for the nursing and pharmacy teams to help coordinate efforts for change.
Descriptive statistics were used to document the trends in the primary outcome. Data after improvement cycles was collected retrospectively from the Electronic Patient Record system at approximately 3-4 month intervals to document the general trend in early aspirin prescription rates over the period of 1 year. The audit department was also contacted to ascertain if similar historical audits had been performed in order to compare our results.
Strategy
Cycle 1 – Interventions
Multiple interventions were designed in an attempt to rapidly improve Early Aspirin prescription.
Presentation: The results from the baseline measurement were presented at the Joint Anaesthesia and Cardiothoracic Surgery Audit Meeting. The evidence supporting Early Aspirin was detailed and the fact that it was routine protocol is several cardiothoracic centres nationally and internationally was stressed. Surgeons were encouraged to lead their teams in ensuring that the grafts they have placed during surgery are protected.
IT Error identified: The root cause of the allegedly prescribed but subsequently “lost” aspirin prescriptions was also explained by liaising with the IT team. Due to a recent change in the licensing category of aspirin suppositories in the hospital pharmacy, electronic prescriptions made via older ‘personal order sets’ were being automatically discarded. The need to update all order sets was stressed.
Emails and Reminders: An email highlighting the salient points of the presentation was sent to all doctors in the cardiac surgery department. We also encouraged nursing and pharmacy staff to provide reminders and regular feedback by alerting medical teams to absence of early aspirin prescriptions.
Nursing specific Leaflet: Lastly, a nursing specific intervention for all staff working on the Post Operative Critical Care Unit was arranged. A single page leaflet on Early Aspirin for nurses was distributed through the Critical Care Education Team and daily 5 min presentations during morning handover were given over the period of one week.
Cycle 1 Results:
The data to asses results from the first improvement cycle was collected 2.5 months after the baseline measurements presentation. The prescription of Early Aspirin improved from 23% to 48%. The number of patients in the Red Zone decreased from 66% to 45%.
Cycle 2 – Interventions
Presentation: The results from the first cycle were once again presented at the 2 monthly Joint Anaesthesia and Cardiothoracic Surgery Audit Meeting. We congratulated the medical, nursing and pharmacy teams and on the positive trends in early aspirin prescription and encouraged continued improvement.
More IT Concerns: Further information technology concerns were highlighted during the ensuing discussion after the talk. While there were no longer any “lost” prescriptions, the default setting of “Morning” on the e-prescription occasionally resulted in aspirin suppositories being prescribed for the following day as opposed to 6 hours post operatively. Following this feedback we worked with the Electronic Patient Record (EPR) Committee and successfully modified the default frequency for aspirin suppositories from a daily “morning” dose to a blank ‘required field’ allowing prescription of a “once only” and a “time critical dose”.
Stickers: Additionally, we continued with the drive to increase awareness. Yellow stickers with a bold reminder slogan for Early Aspirin were strategically stuck on all mobile and stationary computer carts in the Critical Care Area and in all Cardiac Theatres.
Cycle 2 Results:
Data for the second cycle was collected 3.5 months after the second audit presentation.
The results showed that the awareness drives and multidisciplinary team based approach had been successful in dramatically improving Early Aspirin prescription after CABG surgery to 55% and proportion of patients in the Red Zone decreased to 33%. (See Figure 1 and Figure 2)

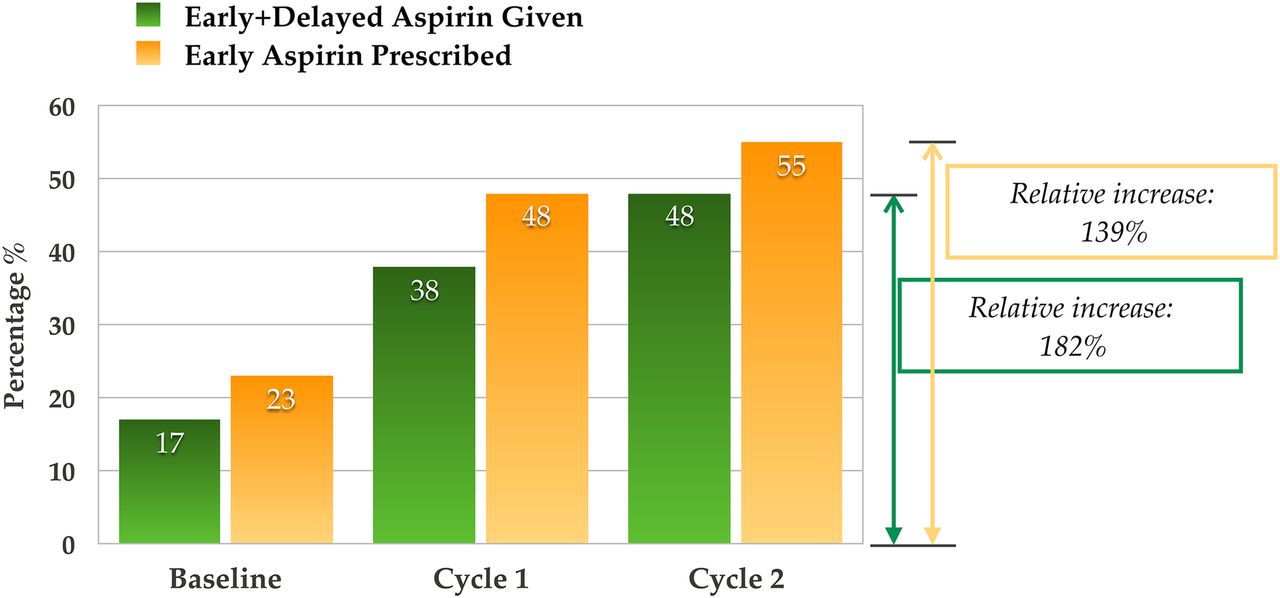
The prescription of Early Aspirin dramatically improved from 23% to 48% and finally to 55% by the second cycle. The administration of loading dose of 300mg aspirin (Early Aspirin and delayed aspirin up to 12 hours post operatively) also showed improved trends from 17% (Baseline) to 38% (Cycle 1) and finally to 48% (Cycle 2)
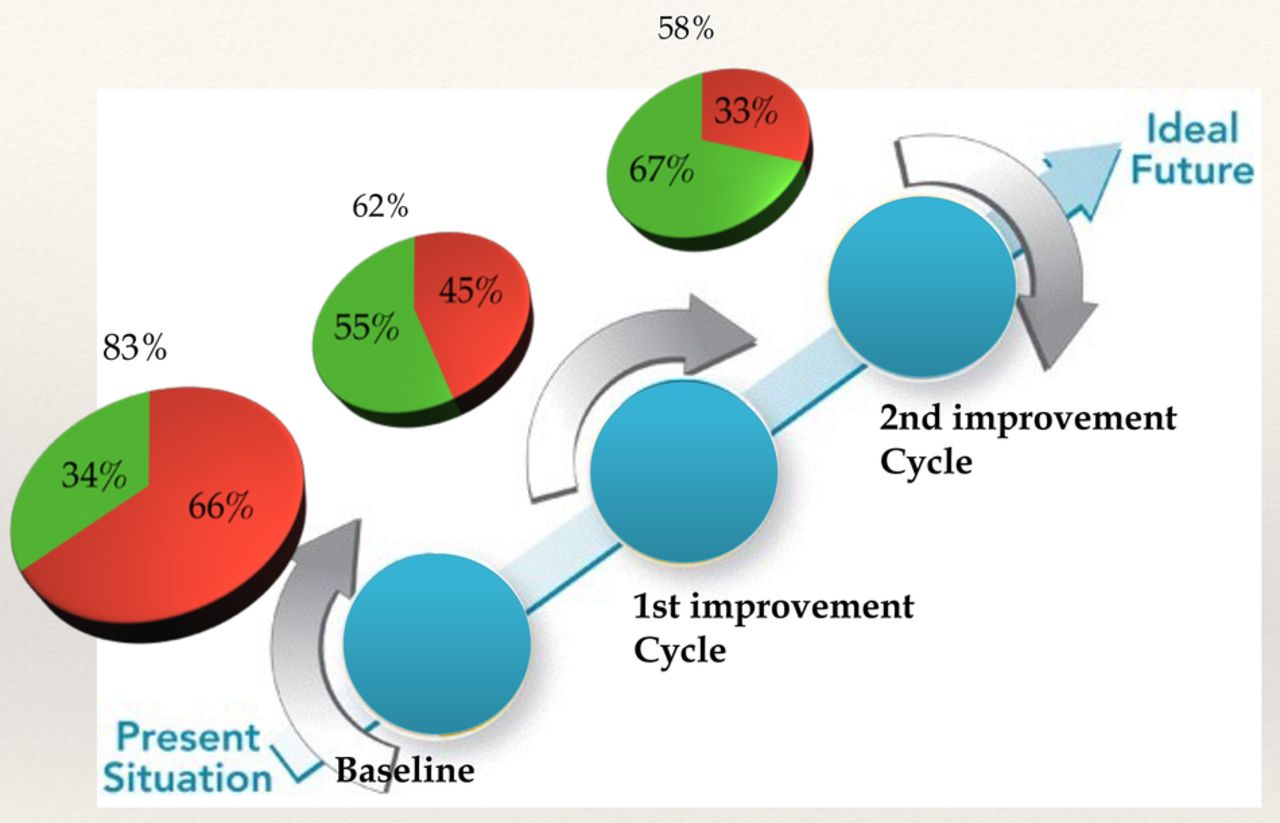
The size of each pie chart represents the proportion of patients in whom Early Aspirin was NOT GIVEN/OMITTED in each Cycle (83%,62% and 58% respectively). These patients are further divided into the Red Zone (no clinical reason for omission) and Green Zone (acceptable clinic reason for omission). The proportion of patients in the Red Zone decreased from 66% (35/53) patients, to 45% (29/65) patients to 33% (19/58) patients at baseline, Cycle 1 and Cycle 2 respectively.
The findings were informed via email to all medical staff in the cardiac surgery and anaesthetics department. The topic has become a subject of healthy debate in the hospital and we expect continued positive trends.
Results
The prescription of Early Aspirin dramatically improved from 23% to 48% and finally to 55% by the second cycle. The administration of loading dose of 300mg aspirin (Early Aspirin and delayed aspirin up to 12 hours post operatively) also showed improved trends from 17% (Baseline) to 38% (Cycle 1) and finally to 48% (Cycle 2) [Figure 1].
The proportion of patients in the Red Zone decreased from 66% (35/53) patients, to 45% (29/65) patients to 33% (19/58) patients at baseline, Cycle 1 and Cycle 2 respectively. Thus, the proportion of patients with omission of Early Aspirin despite clear indication for it decreased by 50% over a 10 month period following audit led changes. [Figure 2].
In patients who were not prescribed “Early Aspirin”, a regular dose of 75mg aspirin was commenced routinely from the morning of first postoperative day with or without other anti-platelets.
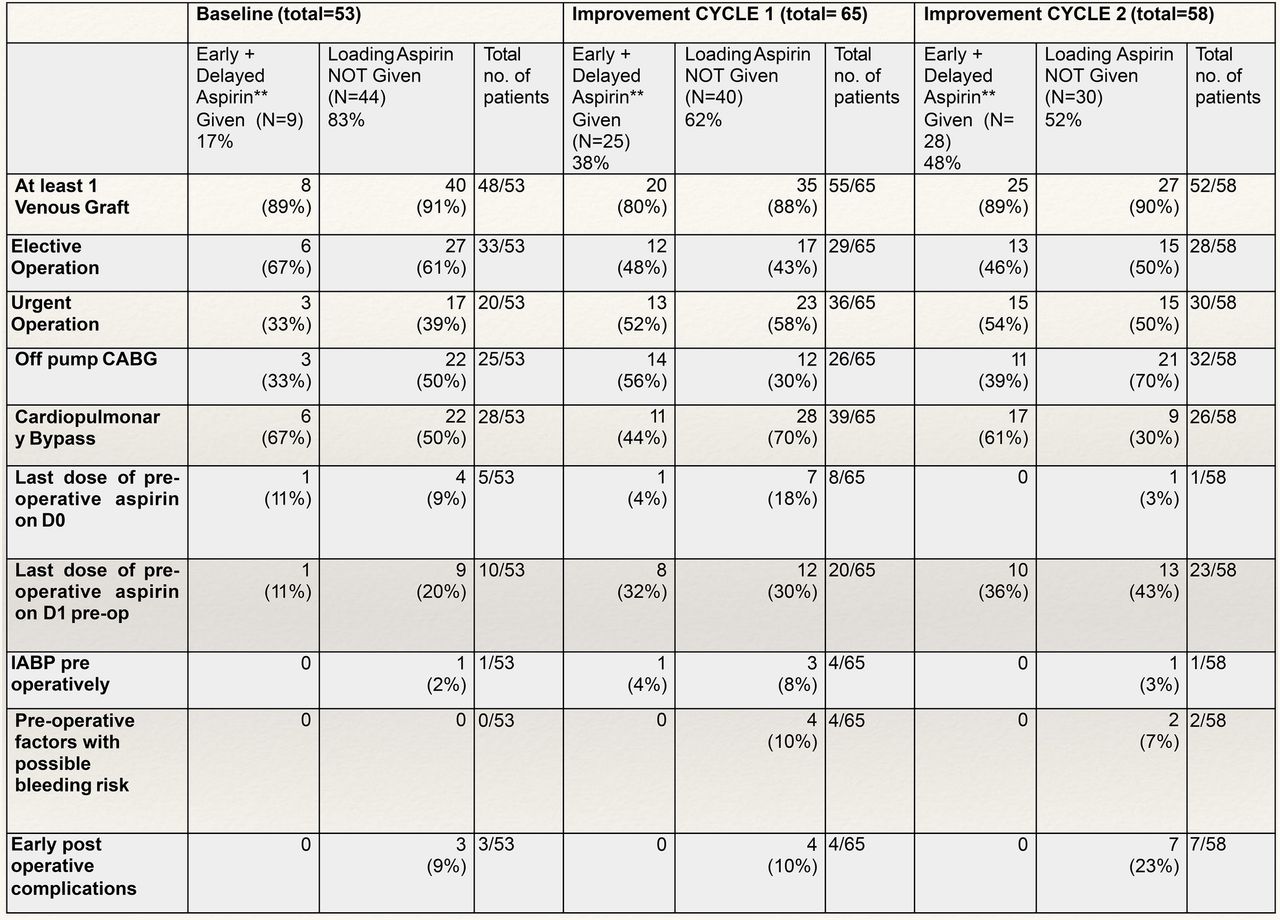
A detailed review of pre-and post operative factors for both improvement cycles is tabulated in Figure 3. The salient features are summarised below:
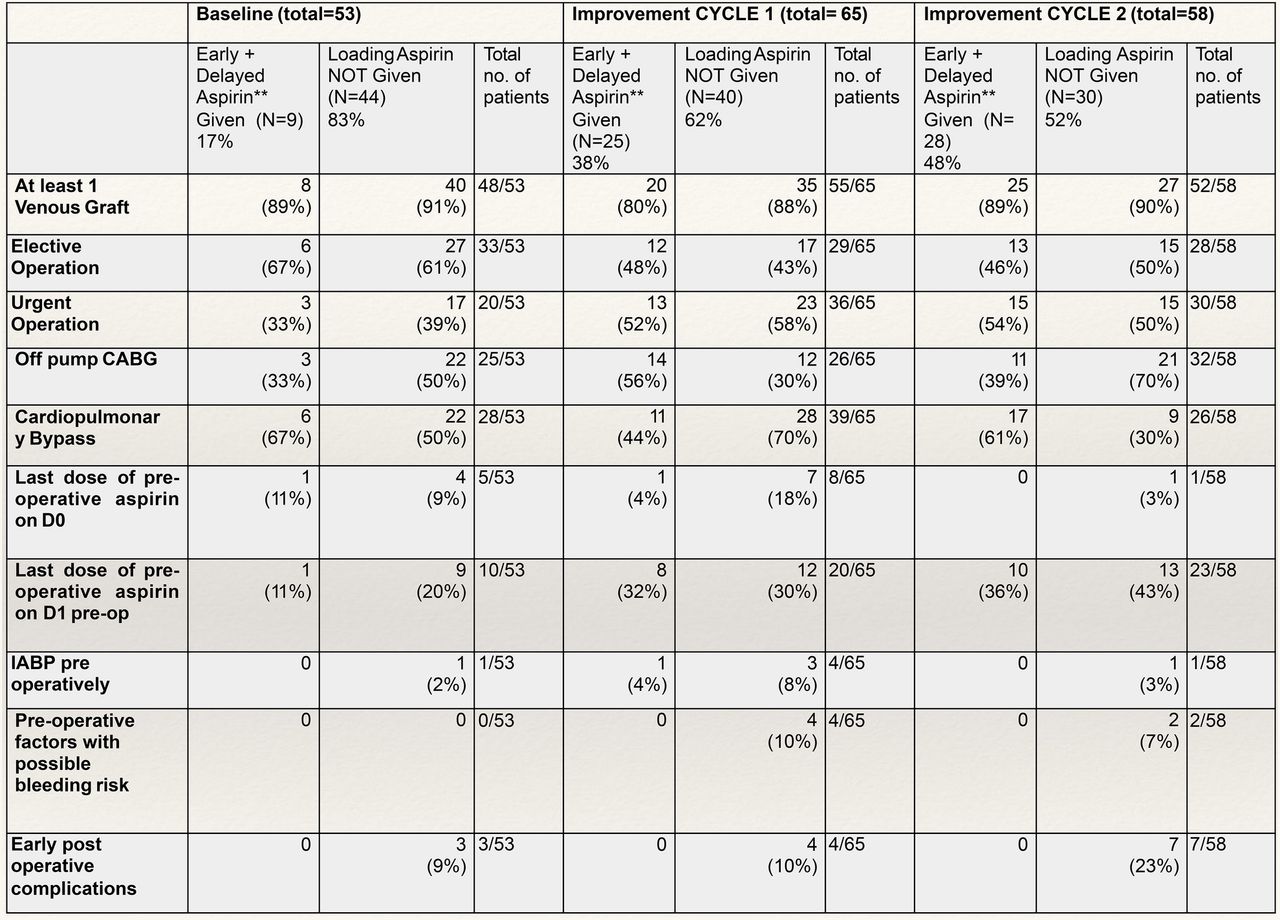
Detailed tabulated results
Out of 65 patients in Cycle 1 (01.01.2016 – 31.01.2016): 48% of patients (31/65) had a prescription for “Early Aspirin” and 38% (25/65) of patients received a loading dose of 300mg Aspirin. 20/25 patients receivded aspirin appropriately within 6 hours, and 5/25 patients received a delayed dose upto 12 hours.
On pre-operative factor review – 8/65 of patients received regular 75mg aspirin up until and including the morning of surgery (D0). 4/65 patients had relevant pre-operative co-morbidities including peptic ulcer disease, < 7 days omission of thienopyridine anti platelet drugs (clopidogrel, ticagrelor) pre-operatively and a past medical history of per rectal bleed on dual anti platelet loading. Early post operative complications identified included 2 resternotomies, 1 suspected cardiac tamponade and 1 patient with ‘excessive bleeding’ in drains. For Cycle 1 mean bleeding into drains by 6 hours post operative was 351mls (2SD 430mls), excluding patients needing a resternotomy.
Out of 58 patients in Cycle 2 (01.06.2016 – 20.06.2016): 55% (32/58) of patients had a prescription for “Early Aspirin” and 48% (28/58) of patients were administered the loading dose of 300mg of Aspirin. 23/28 patients received Early Aspirin appropriately within 6 hours post op and 5/28 patients received a delayed dose between 6-12 hours.
Additionally from a pre-operative view point, 1/58 patients continued to receive regular aspirin including the morning of the operation (D0), 2/58 patients had gastric ulcers and 1 patient was allergic to aspirin. Early post operative complications included excessive bleeding (below resternotomy thresholds) that settled with blood products in 4/58 patients and 3/58 required a resternotomy.
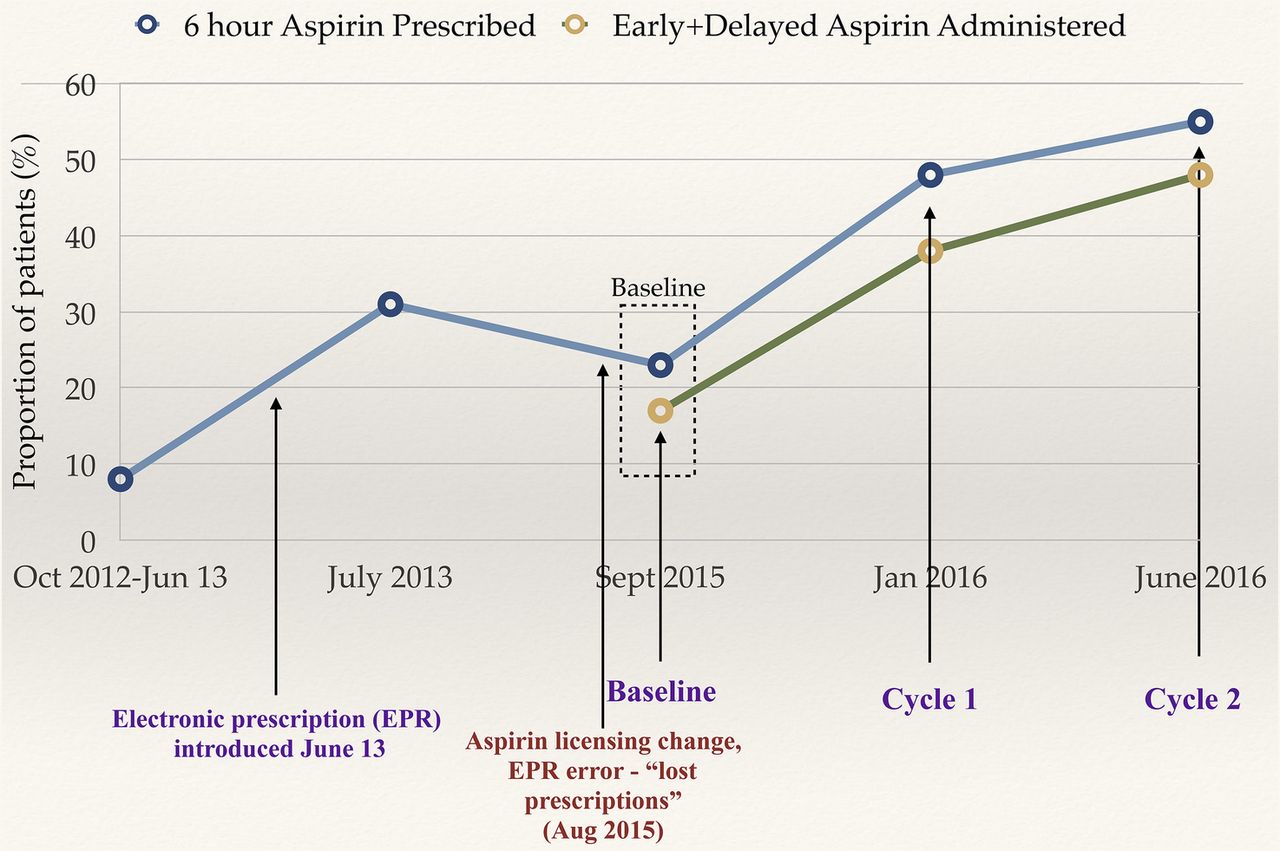
Lastly, the run chart attached [Figure 4] shows the trends in Early Aspirin prescription over time and includes results from a similar historical retrospective audit at our centre that aimed to document the Early Aspirin prescription rates in patients undergoing CABG surgery prior to (49 patients) and after (77 patients) introduction of the electronic prescription system in June 2013. It can be seen that electronic prescribing vastly helped improve the proportion of our CABG patients who were prescribed Early Aspirin from 8% to 31%. However, the proportional Early Aspirin prescriptions did not show much variability between July 2013 (31%) and Sept 2015 (23%) though further data in interval periods would have been helpful. A recent change in the licensing category of aspirin suppositories in our hospital pharmacy a month prior to our Baseline assessment also led to an IT error resulting in some intended prescriptions being “lost”. This might partially account for the slightly lower baseline measurement of our audit. Nevertheless, the significant improvements in Early Aspirin prescription after Improvement cycles can be clearly seen.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Run chart
Lessons and limitations
EACTS and AHA guidelines strongly recommend “Early Aspirin” post CABG surgery. We identified problems with compliance for prescriptions of Early Aspirin at our large tertiary centre. We systematically analysed possible causes and invited open discussion that helped identify hospital culture as the primary limiting factor.
A multi pronged and phased strategy included changing culture through education, repeated reinforcement of the message with visual prompts such as stickers/leaflets and solving information technology problems. Importantly, we engaged non-prescribers in the audit process and asked for their opinion on how prescription rates could be improved. We believe this inclusive approach was essential for change.
Statistical analysis was limited to descriptive statistics due to the obvious prescriber bias against Early Aspirin prescription. We expected this unquantifiable bias to confound results if comparisons were to be made against different categorical variables such as pre-operative anti-platelets, nature of grafts and complications that are illustrated in Figure 3.
However, clinical practice often varies from guidelines due to a number of reasons. Furthermore, it is important to acknowledge that the guidelines do have limitations such as the lack of definition of acceptable bleeding in the post operative period for the safe administration for Early Aspirin. Previously published studies use thresholds for resternotomy as the definition for “excessive bleeding”.7 Our hospital policy sets resternotomy cut-offs at >200mls/hour for 2 hours or >1000 mls in the first 6 hours. However, we suggest that in the absence of published evidence, there might need to be more conservative local guidelines to determine safe bleeding thresholds for administration of Early Aspirin. Across all improvement cycles, 2 patients had a prescribed dose of aspirin witheld by nursing staff due to concerns of excessive bleeding that did not meet criteria for resternotomy. The level of bleeding causing clinical concern remains a subjective definition and a significant limitation.
Guidelines are also unclear whether patients continuing 75mg aspirin up to the day prior to surgery (last dose on D1 pre-operative) should be reloaded with a medium dose of aspirin post-operatively or alternatively should receive their usual dose of 75 mg aspirin within 6 hours. This is a decision that can be left to clinical discretion. Additionally, whether patients who continue to receive regular low dose aspirin on D0 or the morning of the operation would merit from Early Aspirin at all is an little explored area of study. However, studies in primary coronary intervention populations have shown improved inhibition of platelet activity with peri-procedural reloading of anti platelets above regular maintenance dose.8 ,9 Thus certain clinical scenarios do need further clarifications, yet broadly the guidelines are useful for routine care.
We also acknowledge that our audit could have been improved by identifying a senior team leader, perhaps one in Cardiac Surgery and one in Anaesthetics to champion the cause and ensure delegation of responsibility. Currently the responsibility for prescription of post operative medications is that of the anaesthetist but prescription of Early Aspirin is shared between anaesthetists and cardiac surgeons. Consequently, there is a risk of lack of accountability or an expectation that some else might do the prescribing.
Additionally, limitations of our audit design include multiple interventions in each Improvement Cycle. Therefore it remains unclear which specific intervention was responsible, and to what degree, for the improvement noted in each cycle. We also note that none of the proposed interventions were tested for benefit on a small scale before hospital wide implementation, and hence it remains a possibility that some interventions did not have any benefit. Our approach to the problem was to identify simple solutions based on first principle reasoning and simultaneously roll out multiple interventions in the hope of a cumulative improvement effect. However, this limits intervention-effect analysis and hence replicability in different settings. Additionally, hospital wide interventions and IT changes were relatively easy to implement in our dedicated 187-bed specialist cardiothoracic centre hospital due to ease of accessibility to IT and other hospital teams, uniformity of electronic systems and common hospital-wide indication of use of aspirin. The practicalities of implementing change might be more complicated in larger multi-speciality centres.
Lastly, infrequent measurement at only 3 points with interval periods of months lends to a possibility that the variation in Early Aspirin prescription documented could be due to random fluctuations. However, the authors strongly feel that the historical audit data supports our hypothesis that poor Early Aspirin prescriptions at baseline were indicative of long standing cultural practices. Hence, it logically stands that the subsequent large improvements in Early aspirin prescription and administration are reflective of audit led changes. Ideally, a prospective study, such as continuous monthly assessments of all CABG cases over a year would be necessary to conclusively confirm sustained improvement.
Furthermore, local hospital guidelines for Early Aspirin would greatly help in ensuring a sustained change and clarify policies such as bleeding thresholds. However, this is currently still in development. In the future creating uniform ‘order sets’ for post operative CABG care could also help standardise medications. The sustainability of interventions depend on teamwork and feedback loops between prescribers and non-prescribers to ensure that the common goal of early aspirin for CABG patients is achieved.
Conclusion
In conclusion, our final results post Improvement Cycles show that 48% of isolated CABG patients at our centre are administered “Early Aspirin” while 55% of our patients are prescribed “Early Aspirin”. In comparison, a prospective study of 200 cases from a large teaching hospital in London showed that 69% of their patients received a medium dose of aspirin within 6 hours.7
Although scope for further improvement remains – our inclusive, multidisciplinary approach led to a 139% relative improvement in prescription and 182% relative improvement in administration of “Early Aspirin” after CABG surgery over the period of 10 months. We also successfully decreased by 50% the proportion of patients with an incorrect omission of Early Aspirin despite clear clinical indication. It is clear that continued, sustainable change is necessary and to this effect development of hospital guidelines, dedicated ‘CABG order sets’ and repeated audit cycles are being planned. Our audit strategy highlights the importance of identifying unique local limitations in clinical practice followed by the development of targeted, team based strategies to change hospital culture.
Acknowledgments
The authors kindly acknowledge Amr Moussa and Mr. Neeraj Mediratta for sharing the results of their 2013 audit.
Footnotes
Declaration of interests Nothing to declare.
Ethical approval According to the policy activities that constitute research at Liverpool Heart and Chest Hospital, this work met criteria for operational improvement activities exempt from ethics review.