Article Text

Abstract
Referral and flow management is an important part of outpatient care; some patients require to be seen earlier than the next available appointment because of the nature of their presentation. We did not have a clear pathway for urgent patients being referred to our pediatric neurology service. When we reviewed this process in our Quality Improvement meeting we identified wide variation in the length of time such patients wait to be seen in clinic ranging from 2 to 11 weeks. Only 25% of patients identified as requiring urgent clinic appointments were seen in clinic within 2 weeks of triage.
A new triage system was designed to identify urgent patients consistently. Three PDSA cycles tested change ideas: the first cycle tested introducing an urgent triage system, the second cycle tested giving urgent appointments directly from the triage decision utilising clinic cancellations and the third PDSA tested double notification of appointments for all urgent patients using the call centre and the neurology specialist nurses.
After the third PDSA the percentage of patients seen within 2 weeks of triage increased from 25% to 80%. This change was tested across one clinic initially then tested across two more clinics. Our balancing measure, the third available routine appointment, remained stable indicating that improving access to emergency patients did not affect the waiting time for routine appointments.
With good management of triage it is possible to improve access for urgent patients to be seen in clinic without impact on availability of routine appointments, resulting in better quality of care and patient satisfaction. Earlier appointments also improve clinic attendance rates.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Only 25% of all patients identified as Urgent by the pediatric neurology service at Hamad Medical corporation, Qatar are seen in clinic within 2 weeks of the triage time. Appointments ranged from 2 weeks to 11 weeks for patients identified as urgent retrospectively when the new triage system was tested.
This leads to patient dissatisfaction with the service and higher no-show rate. We did not have a uniform triage system for outpatient referrals which led to inconsistency in the identification and appointment process.
Our service provides tertiary care for all children requiring paediatric neurology consultations in the whole country, being the main academic health centre. We receive referrals from pediatric emergency centres and primary health care as well as from our colleagues within general paediatrics and paediatric sub-specialties, the service receives around 2000 referrals per year.
Background
Referral management is an important part of providing good quality outpatient care; some patients are referred urgently and require an earlier appointment than the next routine appointment because of their clinical condition. Triage for clinic appointments has been subject to a lot of change in recent years. In many healthcare systems special pathways have been developed to ensure patients referred for suspected cancer are seen within a short period of time and an 18 week pathway from referral to diagnosis is in place in most UK trusts.
Some healthcare organisations such as Royal Bournemouth in the UK and Florida State University Hospital in the USA have established a triage clinic to ensure urgent patients are identified promptly and consistently.1 ,2 In Pat Walker Medical Center, Arkansas University a nurse triage system is conducted by phone for referrals. A trained nurse will review all referrals followed by a phone call to ensure that sick and more vulnerable patients are identified and prioritised to be seen urgently.3 In primary healthcare in many parts of the world same day appointments are offered when patients are felt to need urgent attention; examples include the services offered in the UAE under the umbrella of the primary health care services there, where a pioneering project was introduced to ensure all patients requiring urgent appointments are seen the next working day in a 6 day working week system.
Valsangkar et al studied the impact of effective triage and applying the lean process on surgical wait time and found a three fold decrease in the wait time once the new triage and the lean process were integrated.4 Slusar et al evaluated a novel strategy to triage hematology referrals in the ambulatory care setting. Making an effective triage decision resulted in resolving 58% of the issues raised before the clinic review and 90% of the referrers were satisfied with the service.5 Layton et al concluded that the use of triage systems is an effective strategy to reduce the impact of limited provider availability relative to patient census in times of limited resources.6
The paediatric neurology team at HMC receives all referrals for children with neurological conditions as it is the only tertiary referral service for paediatric neurology in the state of Qatar. There are six consultants, two fellows and three specialist nurses. Outpatient clinics are a mixture of general neurology and specialised clinics for epilepsy, movement disorder and neuromuscular conditions.
As effective triage and better access for urgent patients is essential for patient safety, improves attendance to clinics and improves patient and referrer satisfaction, our team identified this area as a priority for our Quality improvement activity and we reviewed our clinic flow over the previous 12 months to identify areas for improvement.
It was clear from the review that we needed a uniform triage system that enabled us to identify urgent patients promptly and consistently among the team members and to work on defining urgency and ensuring that urgent patients are seen within a specific time frame.
The team agreed that 2 weeks is an appropriate time frame for most urgent patients, except patients with symptoms suggesting increased intracranial pressure who should be directed to go to the ED for immediate review.
Baseline measurement
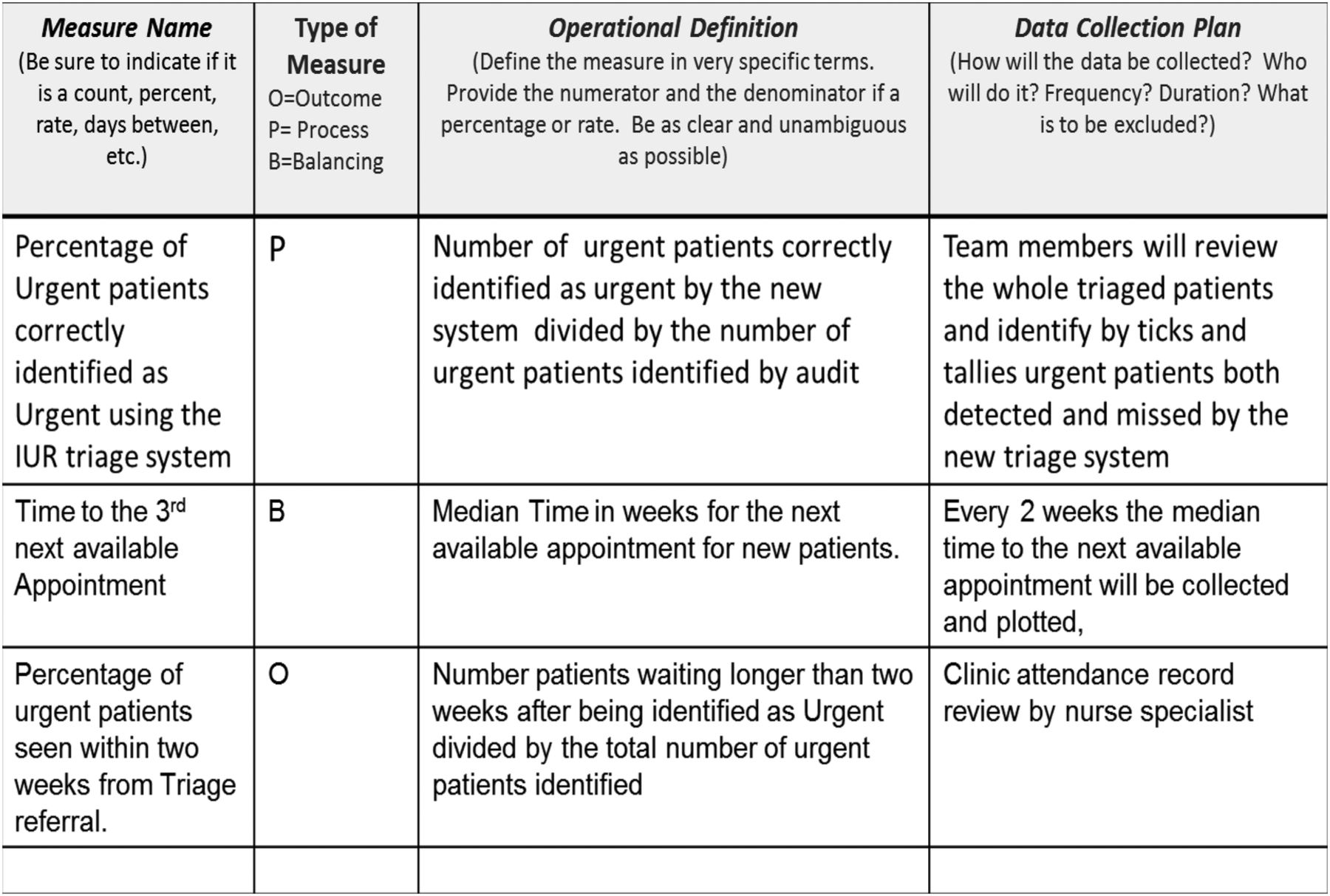
Our outcome measure and main KPI is the percentage of urgent patients seen in outpatients within two weeks of triage as compared to all identified urgent patients referred to Paediatric Neurology at Hamad General Hospital.
The percentage of patients triaged using the new triage system in comparison to all referrals received by Pediatric Neurology was our process measure for the first PDSA while the percentage of patients who were notified of available cancellation slots was our process measure for our second PDSA.
The average waiting time to the third available routine appointment is the balancing measure.
At baseline, only 25% of patients identified as urgent were seen within 2 weeks with a wait for appointments ranging between 2 to 11 weeks.
See Figure 1, Measurement Plan, for details.
Measurement Plan
Design
A high level process map identified the steps for improvement and the team met to discuss ideas for improvement and to implement the Model for Improvement.
PDSA cycle 1 was to introduce a new triage system to improve identification of urgent patients and ensure that inappropriate patients are referred on to the right services while patients who require urgent appointments are identified and dealt with as such.
The team worked on PDSA 2 availing urgent slots for patients identified as requiring such appointments by utilising cancellations and flexible clinic management.
The third PDSA focused on reducing the no-show to urgent clinic slots by improving the notification process and ensuring that patient received appropriate notification of their appointments.
We also monitored our balance measure to understand the effect of the intervention on the routine clinic appointments (third available appointment).
Strategy
PDSA cycle 1: To test whether the new triage system is usable and that it identifies urgent patients correctly.
Plan: all paediatric neurologists were educated about the new triage system which identifies patients as urgent or routine, referring inappropriate patients to other services.
Do: One consultant started to apply the new triage system and recorded how long it took to triage all patients.
Study: the new triage system identified 90% of all urgent patients from the first week and 100% of urgent patients after it was used by all consultants for three weeks. The new triage system did not affect the time it took to triage patients.
Act: The new triage system was built into the routine review of all referrals by the consultants participating in the urgent patient project.
PDSA cycle 2:
To test whether applying the new referral triage and utilising urgent clinic slots will reduce patient waiting time.
Plan: patients identified by the triage system were to be given urgent appointments in the clinic within 2 weeks; the team also applied flexible management by enabling booking into all cancelled and unused clinic slots.
Study: the percentage of patients seen within 2 weeks improved to 60% which met our aim.
Act: we tested this change on two clinics and the results were consistent.
PDSA cycle 3:
To test whether double notification of appointments will increase the percentage of urgent patients seen within 2 weeks.
Plan: neurology nurses were appraised on arranging appointments for urgent referrals and to notify patients in addition to patients receiving a routine notification of their appointment from the call centre.
Do: Once appointments have been made via the referral centre, neurology nurses will contact the family and ask whether they would be able to come or whether they wish for the appointment to be re-arranged. They will also confirm with them the date and time and who will be seeing them.
Study: the percentage of patients seen in clinic within 2 weeks from triage increased to 80% across three neurology clinics.
Act: This change was tested across four clinics after success in two clinics.
Results
Our KPI was the percentage of urgent patients seen in clinics within a 2 week period from the time their referral was triaged.
Our baseline was 25%. Following the first and second PDSA cycles in which we tested a new triage system and raised physicians and schedulers awareness as well as utilised cancellation slots, we achieved the target of 60%. Following the third PDSA focused on notification of urgent patients in order to reduce no-shows, we achieved further improvement to over 80% of urgent patients seen within 2 weeks of triage.
See Figure 2, Percentage of Urgent Patients seen within 2 weeks of Triage for details.

{kind=link}
{kind=link}
Percentage ofUrgent Patients seen within 2 weeks of Triage
Our balancing measure was the median time to the third available appointment as we were concerned that this would be affected by seeing urgent patients. This did not show a change during the study period.
Lessons and limitations
Establishing a new system is always challenging and leads to a lot of skepticism and resistance. However, the fact that all team members were frustrated with the lack of a clear pathway to identify and see urgent patients in the clinics helped to ensure the stakeholders were happy to proceed with the improvement effort.
When patients are identified as needing urgent appointments it is crucial that action is taken immediately to offer them appointments, eliminating the need for multiple steps. Triage may take a bit longer as well as trying to identify the clinic slots but it is time worth spending for the improvement in the quality of care provided.
We were aware from our previous QI work that we have a high no-show rate and this was true for our urgent referrals so we adopted the same strategies that we used in our previous QI project7 of double notification and clear messages to parents about their child's appointments to ensure that they can make the clinic visit.
One limitation was that not everyone in the clinic was willing to participate in the test and we hope that demonstrating the results will encourage them to accept the new system and test it in their respective clinics. The second limitation is in spread as different clinics have different challenges and if we can sustain this improvement within neurology we hope to be able to convince the remaining sections to adopt it across our organisation.
Conclusion
This quality improvement project demonstrated that it is possible to reduce waiting time significantly for urgent patients without affecting the overall waiting for the clinic.Three strategies combined enabled us to increase the rate of urgent patients seen within 2 weeks from 25% to 80% in 6 months.
Acknowledgments
We acknowledge the role of Dr Mohammad Janahi the sponsor for this project and Dr David Vaughn the project coach and Ms Amal Chehab and Ms Hanan Osman our neurology specialist nurses.
Footnotes
Declaration of interests Nothing to Declare
Ethical approval This work was deemed an improvement study and not a research study on human subjects as patients were not affected directly and their treatment was not altered nor were they given an experimental or novel therapy, the local research policy meant that ethical approval was not required.