Article Text

Abstract
The assessment of post-operative patients is vital to identify early complications and ensure patient safety. Good clinical record keeping is essential for effective continuity of care and patient safety in the post-operative period. A group of foundation year 2 (FY2) doctors noted a disparity in levels of confidence and ability in performing this assessment.
The aim of the project was to improve documentation and understanding of day one lower limb arthroplasty reviews by FY2 doctors.
The Plan-Do-Study-Act model for continuous improvement was adopted from September 2015 to July 2016. A composite score comprising the twelve most important review parameters for documentation was used to score the quality of documentation on an ongoing basis. An electronic survey was completed by every FY2 rotating through the department. Interventions included registrar-led teaching sessions and an integrated review form placed in the medical notes. Further iterations of the proforma and further interventions were coordinated with the ward clerks, sisters, physiotherapists and senior clinicians.
The baseline mean composite score was 6.3/12. Following implementation of a standardised proforma this score improved to 10.5 in those who had used the proforma, but 5.7 in those who hadn't. Electronic survey responses showed the proforma and teaching were effective in improving knowledge and understanding of post-operative reviews.
The use of an integrated proforma in the medical notes and teaching it's use at induction, improves the documentation and understanding of day one post-operative reviews. Coordinating ward-based change across a cohort of FY2s, with involvement from the multidisciplinary team and management, affects sustained improvements in patient reviews.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Foundation doctors change rotations every 4 months and induction into new specialities has been shown to be variable in terms of quality and duration.1 The initial weeks of a new job represent a stressful and steep learning curve. A group of foundation year 2 doctors (FY2), on their first orthopaedic rotation found a striking disparity in the quality and consistency of their post-operative reviews. When witnessing more senior colleagues performing the same tasks, they noted a weakness in their own knowledge and ability. The group of FY2s set up a quality improvement project to improve their practice.
The project setting was a 28 bed elective orthopaedic ward in a busy district general hospital in the United Kingdom. The inpatient load was predominantly total knee (TKR) and total hip (THR) arthroplasty patients. Staffing on this ward comprised one nurse to 6 to 12 patients, cared for by a team of doctors, physiotherapists and occupational therapists. Four FY2 doctors provided the medical care on the ward, with assistance from 4 other training and non-training grade doctors, on a rota basis. FY2s rotate through the department every 4 months, meaning there were 12 FY2s in total, over the 12 month period. Post-operative reviews on elective patients were daily, with the first morning after surgery termed the ‘day one post-operative review.’ Prior to this project there was no agreed guidance or standards for such reviews. Patients benefit from a thorough and consistent approach to post- operative reviews. The aim of the project was to improve documentation and understanding of day one lower limb arthroplasty reviews by FY2 doctors. The target for improvement was to show measured improvement in documentation during the first cohort of FY2s which was transferred across subsequent cohorts, and sustainable within the department to the next academic year of trainees.
Background
Early post-operative reviews are key to good peri-operative care, enabling early recognition of potential complications and halting their progression.2 It is essential these reviews cover a wide array of parameters including pain control, venous thromboembolism prevention, early mobilisation, wound breakdown, stiffness and hospital acquired infection. Reviews need to be thorough and accurate but also concise and efficient. Clear, legible and precise documentation is a General Medical Council requirement for good medical practice.3 In the last five years, litigation in surgery has risen by 66% and orthopaedic surgery accounts for the largest proportion of claims.4 The majority of litigation is attributed to communication, both written and verbal.5
There have been many strategies to address the challenges involved in the care of surgical patients. Of these, the strongest evidence lies with checklists and proformas, similar to initiatives in the airline industry.6 ,7
Baseline measurement
A quantitative measure of post-operative review documentation and a qualitative assessment of doctor confidence were used measure improvement during the project.
After discussion with senior orthopaedic surgeons, a composite score comprising the 12 most important aspects of a post-operative review was created (see table 1). One point was awarded for the inclusion of each review parameter, with a maximum score of 12. Baseline data was collected over a one week period in September 2015, from the medical notes of all patients (n=33) with day one post-operative reviews.
The same week, an electronic survey was sent out to all four FY2 doctors containing 10 questions related to their confidence in assessing and documenting day one post-operative reviews in elective TKR and THR patients (see table 1 and 2).
12 point composite score used to analyse post-operative reviews
10 questions sent to each FY2 doctor via electronic survey. SD=Strongly Disagree, D=Disagree, N=Neutral, A=Agree, SA=Strongly agree
Design
A single post-operative review proforma, for both TKR and THR patients, was created after discussion with senior colleagues (see figure 1). The proforma was developed through progressive iterations and ultimately combined in the post-operative multidisciplinary continuation section of the medical notes. This involved the multidisciplinary team (MDT) of physiotherapists, occupational therapists, ward clerks and managers. Teaching was provided to accompany the development of this proforma, as well as amendments to the departmental induction programme given to each cohort of FY2 doctors.

Post operative review proforma
Data was collected prospectively on a once-weekly basis from randomly selected medical notes on the elective ward. 98 sets of medical notes were assessed in total, from September 2015 to July 2016. A score out of 12 was awarded to each day one post-operative review. The same baseline electronic questionnaire was sent to each cohort of FY2s at the start and end of each four-month rotation except the first rotation where only a baseline questionnaire was undertaken at the end of their attachment.
Interventions were planned and implemented using the Plan-Do- Study-Act (PDSA) model for improvement.8
Strategy
PDSA cycle 1: The new proforma (see figure 1) was made available on the elective ward and doctors asked to use it when reviewing patients from September 2015. The review scores of 21 randomly selected medical notes at the end of the cycle, and doctor confidence scores via electronic questionnaire, improved (see results section). Studying the results in this cycle showed doctors were still unsure regarding the use of some parts of the form and it was sometimes difficult to find the form in the medical notes.
PDSA cycle 2: From December 2015, the proforma was placed in the medical notes of every elective patient, on admission to the ward.
This duty was carried out by the ward clerk, after agreement from departmental managers. The proforma was placed next to the multidisciplinary continuation booklet and printed on bright yellow paper to enable doctors to find it with greater ease.
The second cohort of FY2s rotating in December received a registrar- led teaching session regarding the use of the proforma. The results during this cycle showed further improvements in 12-point scoring, based on 25 randomly selected medical notes (see results) at the end of the cycle.
PDSA cycle 3: Due to logistical difficulties and on call rotas, teaching for the third cohort of FY2s, rotating in April 2016, did not take place. Data collection of 19 sets of randomly selected patient notes showed the usage of the proformas decreased dramatically. Acting on this observation, and given the success of the improvement strategy in previous PDSA cycles, the use of the proforma was included in the induction programme presented to all new FY2s rotating through the department. This permanent change to departmental protocol aims to ensure sustainability of improvements observed during the early part of this project.
Results
98 sets of medical notes were assessed between September 2015 and July 2016. Of these, 53 patients received TKR surgery and 45 received THR surgery.
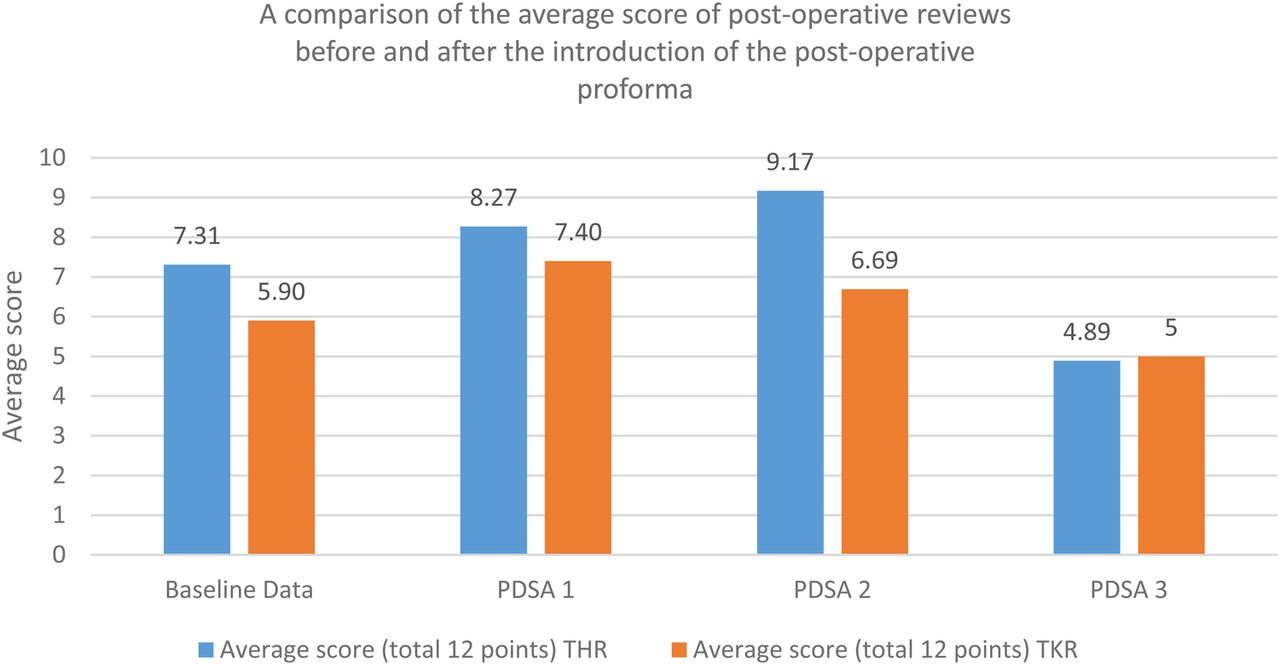
From baseline to PDSA cycle 2, mean scores increased from 6.45 to 7.88. Over this time, THR scores were consistently greater than TKR scores. The highest score (9.17) was for THR during the second PDSA cycle. Scores decreased during the final PDSA cycle, from 7.88 to 4.95.
Figure 2 shows usage rate of the proforma during the PDSA cycles. Baseline data collection showed an average score of 7.31 for THR (n=13) and 5.9 for TKR (n=20). Scores increased to 8.27 (n=11) and 7.4 (n=10) respectively for PDSA cycle 1. PDSA cycle 2 showed an increase of score to 9.17 for THR (n=12) but small decrease to 6.69 for TKR (n=13). Results for the third cycle were lower at 4.89 (n=9) and 5 (n=10) respectively.
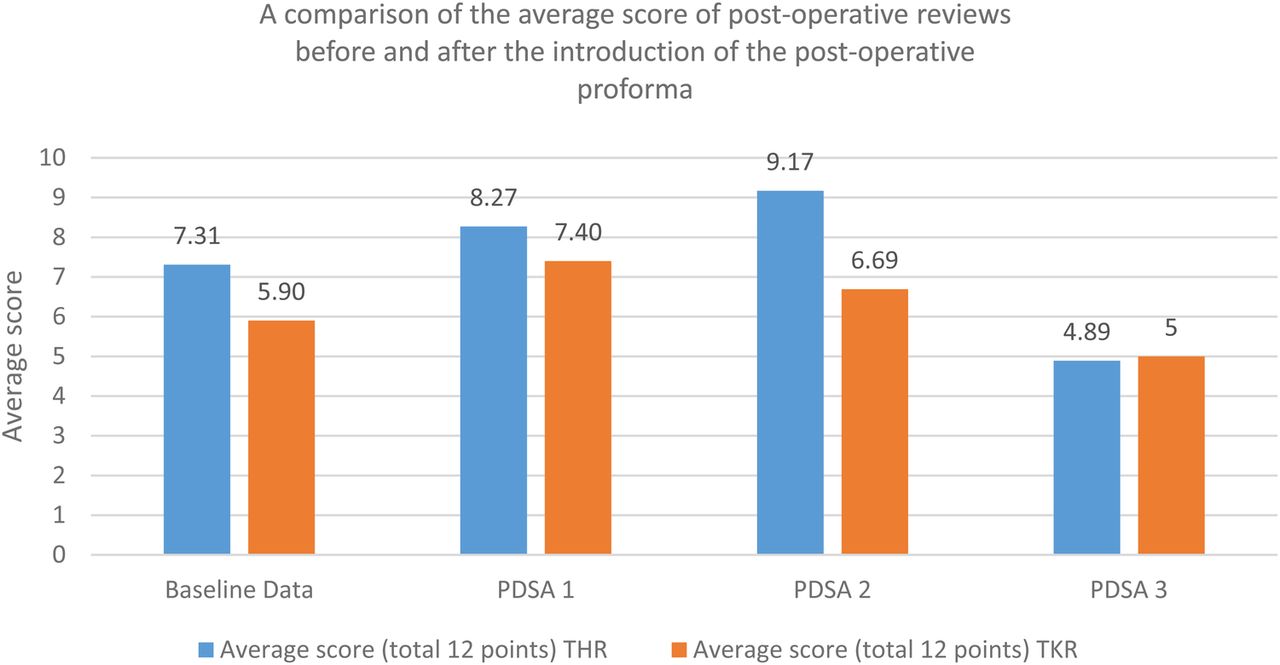
Average score for each PDSA. % used proforma for each PDSA=baseline data (N/A), PDSA 1 (47%), PDSA 2 (42%) and PDSA 3 (0%). THR=Total Hip Replacement and TKR=Total Knee Replacement
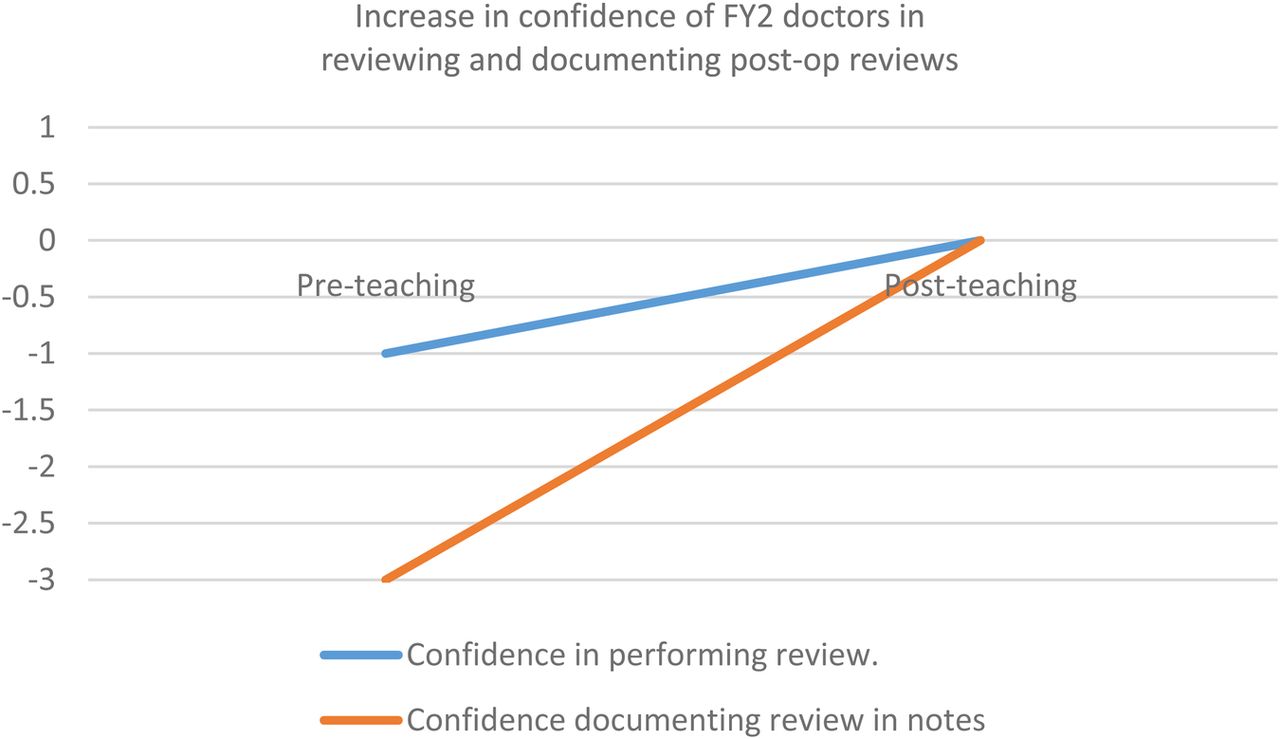
Figure 3 divides scores based on usage of the proforma. The post- operative reviews that used the proforma had scores of 10.57 for THR and 10.50 for TKR whereas those not using the proforma had scores of 5.78 and 5.72 respectively. Response rate of the electronic surveys was 100% (n=16). Figure 4 shows the increase in confidence of FY2 doctors in reviewing and documenting post-operative reviews before and after teaching was implemented.

A comparison of the average score of post-operative reviews with and without proforma. THR=Total Hip Replacemnt and TKR=Total Knee Replacement.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Increase in confidence of FY2 doctors in reviewing and documenting post-op reviews. Y axis represents subjective
Lessons and limitations
This QIP has demonstrated how the use of a day one post-operative proforma for FY2 doctors increased practitioner confidence and clarity of documentation. Due to the nature of rotational medical training, maintaining project momentum and improvements were challenging. The starting points, in terms of knowledge and experience of the FY2 doctors, where not assessed. The cohort was heterogenous and while improvements in confidence were observed, there was no objective pre- and post-intervention testing, meaning absolute knowledge was not assessed. The observed improvement may also have been a chance finding due to the small numbers (n=16) involved.
Measurement bias was addressed by randomly selecting the medical notes assessed, however, assessors were not blinded to the doctor completing the proforma. Results improved when the proforma was used and this is widely generalizable to other healthcare settings, however, sustainability requires a change in protocol in terms of inducting new trainees in the use of the proforma. The proforma was shown successful, however, usage of the proforma was this biggest challenge to sustainability. Incorporating it into the TKR/THR admission bundle improved usage rates and changing the departmental induction programme is key to sustaining the positive changes observed over time.
Experiences from this project have demonstrated the necessity of teamwork to implement meaningful and sustainable improvements to patient care. Collaboration with other healthcare professionals was invaluable to realising the ideas for improvement developed by the cohort of doctors. Identifying a project-champion within each cohort of FY2 doctors, as they rotated, was important to maintain project momentum.
Conclusion
This project has shown that use of an integrated proforma increases confidence and quality of documentation for post-operative orthopaedic reviews. A review proforma was a useful resource, improving confidence and ability across a year of FY2 doctors rotating through an orthopaedic department. Teaching improved FY2 confidence, however, when teaching was omitted results were still better than baseline. The proforma was a useful resource for ward doctors and an effective adjunct to formal teaching. We feel that this proforma acted as an enabling checklist and aide memoire with positive results in line with the literature.6 ,7 The proforma enables contemporaneous and accurate documentation in line with national guidelines.3 ,9 This project highlighted the importance of coordinating ward-based change with help from the MDT. This improves the likelihood of improvements being sustainable past the lifespan of the project.
The positive results and feedback demonstrated here show that provided steps can be put into place to ensure proformas are being used, this project could be replicated in other post-operative settings, with subsequent benefits for patient safety. We believe this project has led to improved post-operative patient safety and increased satisfaction for junior doctors and allied healthcare staff. Next steps have been to amend the induction programme for new FY2s to ensure the proforma continues to be used on an ongoing basis.
Acknowledgments
Irene Richards, Matthew Burwell.
Footnotes
Declaration of interests Nothing to declare
Ethical approval This quality improvement project did not require any ethical approval as was considered exempt. All results and data were fully anonymised throughout.