Article Text

Abstract
Iron deficiency and anaemia are common in pregnancy. Audit data from our tertiary obstetrics unit demonstrated 22% of maternity patients experiencing a postpartum haemorrhage received a transfusion; a third of whom were anaemic on admission intrapartum. Australian Patient Blood Management (PBM) Module 5 Obstetrics guidelines focuses on maximising red cell mass at the time of delivery and reducing the reliance on transfusion as a salvage therapy to treat blood loss. A clinical practice improvement partnership began in February 2015 and completed in April 2016; which aimed to implement systems to improve antenatal identification and management of iron deficiency, and improve postpartum anaemia management. In order to develop change strategies, reasons for poor detection and correction of iron deficiency in the antenatal period were identified following a quality improvement methodology. Education was delivered to maternity healthcare providers. Standardised algorithms and an oral iron prescription handout were developed and piloted. Follow-up audit, staff and patient feedback, and other hospital data were collected to measure outcomes. The rate of anaemia on admission intrapartum fell from 12.2% in 2013 to 3.6% in 2016 following the introduction of unselective ferritin screening and other antenatal interventions. Sixty to 70% of maternity patients screened each month had iron deficiency. The algorithms aided staff to become confident in blood test interpretation and management of iron deficiency and anaemia. Patients found the oral iron prescription handout helpful. Additionally, single unit transfusions significantly increased from 35.4% to 50% (p=0.037) over the project timeframe. This project demonstrated the potential to improve patient blood management in obstetrics, reduce anaemia and transfusions by active antenatal interventions.
- Iron Deficiency
- Ferritins
- Blood Transfusion
- Pregnancy
- Anaemia
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Suspected iron deficiency and anaemia remain a problem for pregnant women coming into delivery, and may lead to a red cell transfusion in the event of postpartum haemorrhage (PPH). An audit of transfusion in PPH at our hospital identified the potential for optimisation of antenatal haemoglobin and iron stores to potentially reduce red cell transfusion requirements and improve outcomes. In addition, red cell transfusion appeared to be undertaken liberally, both in terms of the haemoglobin trigger and the number of units transfused. Having identified a gap in antenatal and peripartum blood management, the hospital and the Australian Red Cross Blood Service (Blood Service) collaborated to conduct a clinical practice improvement (CPI) activity.
The CPI project aimed to align practice with current PBM Module 5 Obstetrics guidelines in two specific ways: (1) to improve the identification and management of iron deficiency during the antenatal period; and, (2) to improve the management of anaemia postpartum by rapidly replenishing iron stores when appropriate and reduce unnecessary transfusion. The PBM Module 5 guidelines state that transfusion should be based on symptoms, especially when the haemoglobin concentration is greater than 70 g/L, and is generally inappropriate when the haemoglobin is more than 100 g/L.1 The transfusion of a single unit followed by clinical reassesment is also advocated. We aimed to see whether implementing PBM strategies in the antenatal and postnatal settings would improve haemoglobin concentrations prior to delivery and reduce the rate of transfusion.
Background
Iron deficiency is the most common cause of anaemia worldwide, and even in developed countries where dietary iron is readily available, remains a significant cause of morbidity.2 Anaemia is associated with fatigue, decreased exercise tolerance and reduced quality of life. During pregnancy, anaemia has a deleterious effect not only on the woman affected, but also on the fetus and subsequent child health outcomes, including reduced birthweight, increased risk of preterm birth and an increased risk of anaemia in infancy.3 ,4 The rising concerns about the safety of transfusion have given rise to a renewed focus on conserving the patient's blood with efforts designed to maximise red cell mass and reduce bleeding rather than rely on transfusion to replace lost red cells.5
The Australian Patient Blood Management (PBM) guidelines Modules 1–6 have been developed to focus clinical practice towards not merely reducing transfusion, but to improve the ability of the patient to tolerate impending blood loss as might be anticipated with surgery or childbirth.1 ,6 These guidelines recognise the need to have adequate haemoglobin prior to such haemostatic challenges, and the need for reserve stores of iron to enable a rapid response from the marrow to replenish lost red cells. They also recommend a focus on the appropriateness of transfusion decisions, both in terms of the clinical triggers for transfusion and the amount of blood transfused, noting that liberal transfusion strategies have not shown benefit, and in many circumstances cause harm when compared with restrictive strategies.7–9
Women are at risk of iron deficiency due to increased iron demands from menstruation, pregnancy and lactation. Obstetric guidelines from developed countries generally recommend screening for anaemia with haemoglobin measurement alone.10–12 Organisations following recommended guidelines will only be detecting iron deficiency if anaemia develops before routine antenatal testing, which in most cases is completed by 24–26 weeks gestation. Non-anaemic iron deficiency and anaemia developing after this time is not routinely screened for or treated. Other guidelines for peripartum bleeding do not address the issue of optimising haemoglobin during pregnancy, which indicates there is variability of clinical practice in preparing pregnant women for a known haemostatic challenge with a significant risk of transfusion.13
Baseline Measurement
Audit data from our tertiary obstetrics unit found that 12% of maternity patients who had a PPH (defined as bleeding in the first 24 hours of childbirth of ≥500 mL and ≥1000 mL following vaginal and caesarean deliveries, respectively13) were anaemic on admission intrapartum.14 A majority of this group (58.5%) required transfusion, whereas maternity patients without anaemia required transfusion in only 17.8% of cases. Iron studies were not routinely taken, but with 49% of anaemic maternity patients having red cell microcytosis and a further 28% having falling mean cell volume (MCV) or low ferritin, iron deficiency was suspected or confirmed in the majority of cases of anaemia. Additionally nine women required a postpartum transfusion in the absence of a PPH, seven of these maternity patients presented anaemic.
Postpartum transfusion was also audited. Although PBM Module 5 guidelines recommend transfusing a single unit of red cells then re-evaluating the clinical need, only 14% of transfusions involved a single unit.15 Transfusions were also assessed as likely to be inconsistent with guidelines in a large number of cases. As a result of the audit, significant under-recognition and under-treatment of iron deficiency and overuse of red cell transfusion was identified.
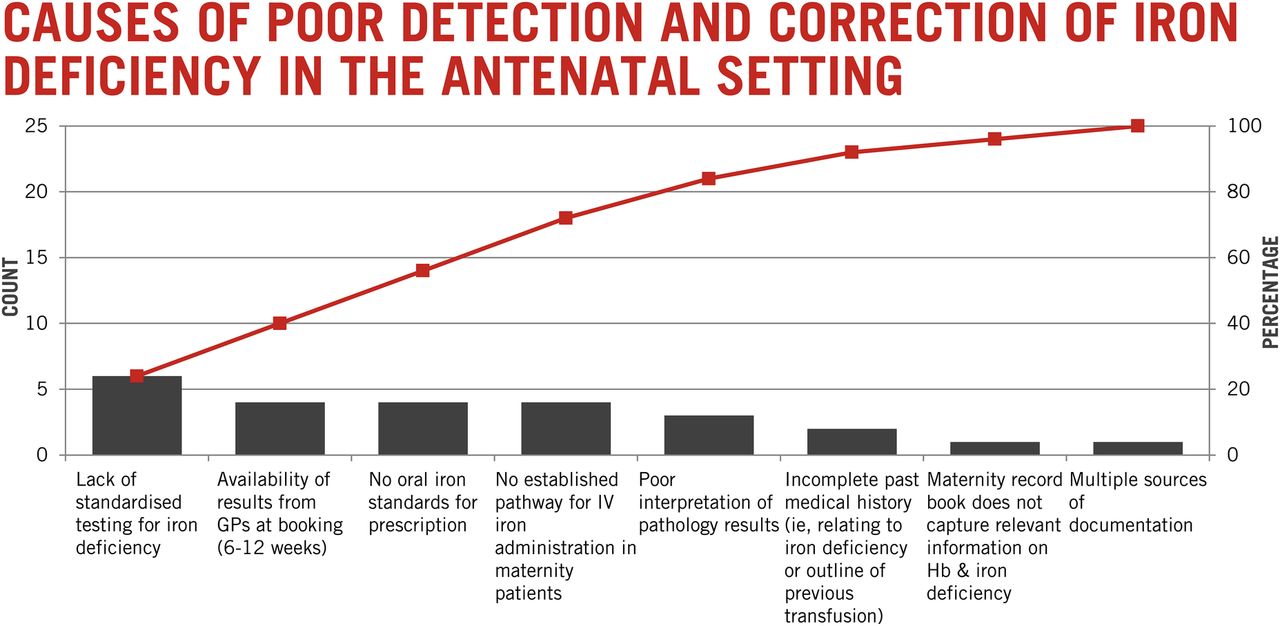
The key areas identified as contributing to poor detection and correction of iron deficiency in the antenatal setting (Figure 1) included a lack of standardisation in testing protocols for iron deficiency; no standardised approach to oral iron prescription with a wide range of products (many of limited efficacy); and, poor interpretation of iron studies. A snapshot audit of 30 pregnant women at booking demonstrated only 10 (33%) had a full blood count (FBC) at booking, 3 (10%) had ferritin measured, and only 4 (13%) had a clinical risk assessment for iron deficiency. Similarly, in the second and third trimesters there were low rates for FBC (53%, 30% respectively) and ferritin (10%, 6%) with no pregnant women offered iron therapy when appropriate.
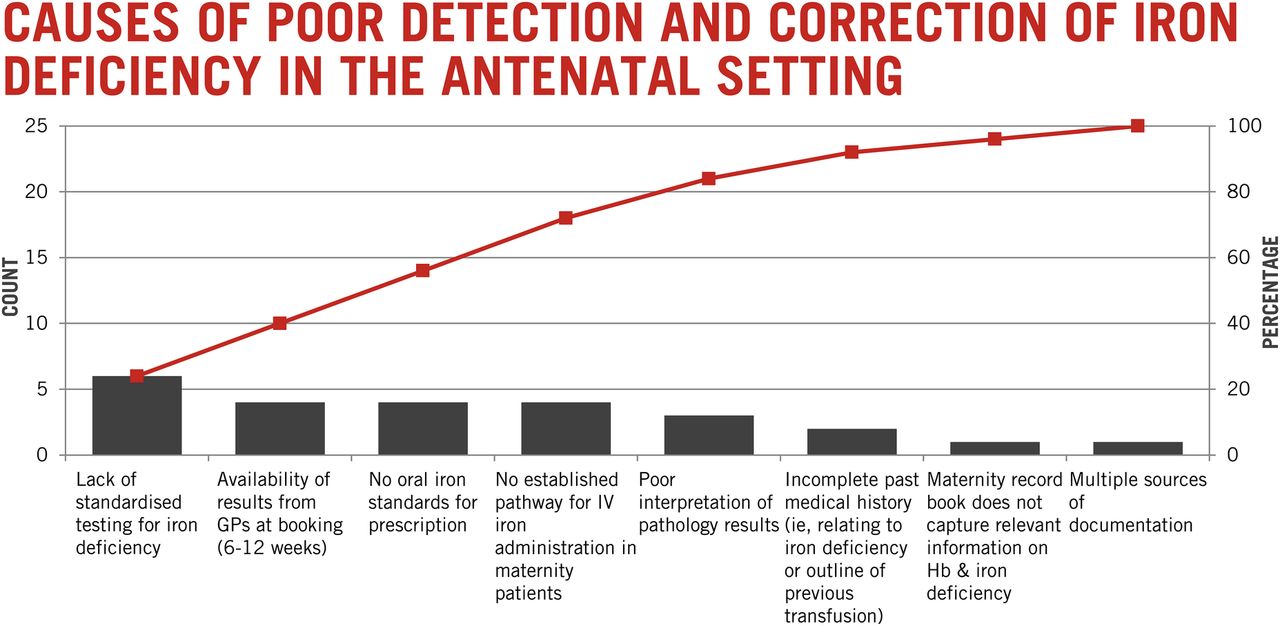
Causes of poor detection and correction of iron deficiency in the antenatal setting
Design
The project was conducted in a tertiary regional referral obstetric hospital with over 3000 deliveries per year which has specialist fetomaternal medicine and neonatal intensive care facilities. Maternity patients delivering at the hospital were identified as having a large number of service entry points including general practitioner shared care, midwife led, standard risk, bariatric and high risk medical, young parent, mental health and substance abuse antenatal outpatient clinics, indigenous health services, and referrals antepartum from local private and interstate hospitals for high acuity care.
In response to baseline results coupled with issues contributing to poor detection and correction of iron deficiency in the antenatal setting, a standardised algorithm was developed for use in all hospital antenatal clinics (Figure 2a). The key features included testing for haemoglobin and serum ferritin on all pregnant women at booking (first antenatal visit) and providing iron therapy to all women with ferritin ≤30 µg/L. Oral iron was preferred but intravenous iron was given when oral iron was poorly tolerated or in late pregnancy when the time to respond to oral iron was limited. Repeat testing was performed as required. The aim was for testing to be conducted with standard antenatal visit when haemoglobin and blood group and screen testing were being performed to avoid additional inconvenience for women. A plan for funding and administration of intravenous iron was developed using iron carboxymaltose as it can be given over 20 minutes by short infusion, minimising the impact on outpatient clinic time. An oral iron prescription handout was developed to provide women with information on the need for oral iron, side effects and the differences between products on the market, highlighting those with doses large enough to be recommended for treatment of iron deficiency (Figure 2b). Implementation was supported by an educational strategy for clinicians and midwives.
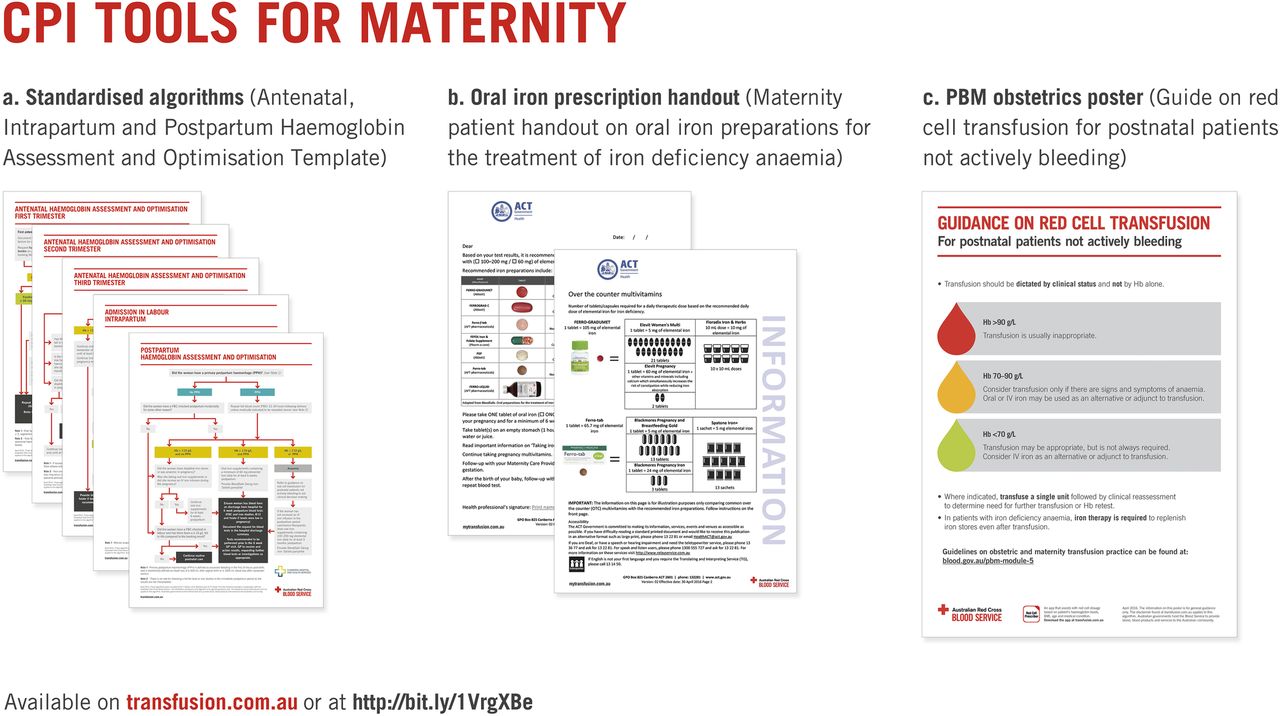
CPI tools for maternity
The impact of interventions was monitored predominantly by observation. Short, open-ended questions were used to elicit target user views on tools developed during the project. Resource utilisation, including pathology testing, intravenous iron and red cell usage rates, were assessed to gauge the impact of interventions, and the effect on pre-delivery haemoglobin and iron deficiency levels were measured to determine the overall outcomes from the interventions.
The CPI activity was led by a multidisciplinary team including representation from obstetrics, haematology and the Blood Service. The improvement team met every month to monitor the project progress. The project began in February 2015 and was completed in April 2016.
Ethics
The audit met institutional ethics committee guidelines for quality improvement. Data collection was also approved by the institutional Human Research Ethics Committee as low risk research. All clinical interventions were conducted within standard clinical practice models and medications prescribed and administered within approved product information. When feedback was sought from patients or staff, providing such feedback was voluntary.
Statistics
Changing variables during the project were plotted in run charts at variable intervals depending on the collection of data with different audits, or monthly for retrospectively collected data. Descriptive statistics were used to feedback survey results. Comparisons before and after interventions were evaluated by the use of two tailed T tests for means or Chi-squared tests where event rates were compared.
Strategy
Antenatal care processes were mapped to maximise the identification of women in early pregnancy and the team reviewed these processes to determine the causes for presenting with iron deficiency. Strategies were then devised and tested to maximise identification of iron deficiency during pregnancy. These were determined by group consensus, aiming to identify potential areas for sustainable changes to practice, considering the ease of implementation and current areas of weakness.
Improvement (PDSA) Cycle 1
Knowledge gaps were identified and addressed with rolling out education across maternity health providers in the hospital. Simultaneously, key stakeholders including midwives and medical leadership were identified and approached to support changes to antenatal clinic and postpartum transfusion practices.
Improvement (PDSA) Cycle 2
Consultation with key stakeholders led to the development of a standardised algorithm and an oral iron prescription handout. The algorithm was posted up in the antenatal clinic wall and handout for patients were provided in the clinic. Feedback from maternity staff and patients were positive. These tools were embedded in practice.
Results
Antenatal
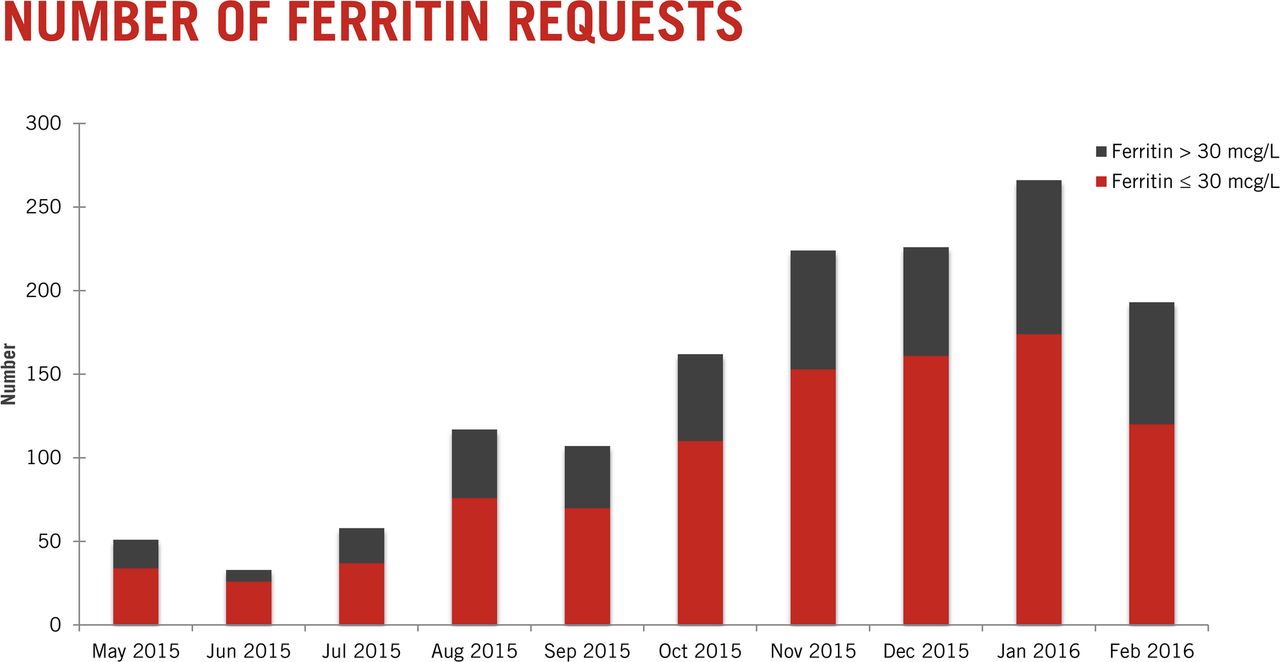
There was a significant increase in the number of ferritin tests being requested from the hospital antenatal settings during the project with 60% to 70% of women screened each month had iron deficiency (Figure 3). An increase in the use of intravenous iron during the same period indicated that iron deficiency, once identified, was treated. A record of women receiving oral iron was not kept as the iron was advised and available from the women's local community pharmacies. Anaemia at delivery improved during the project, with 2/55 women (3.6%) at the end of the project compared to the 53/434 (12.2%) in the 2013 audit.
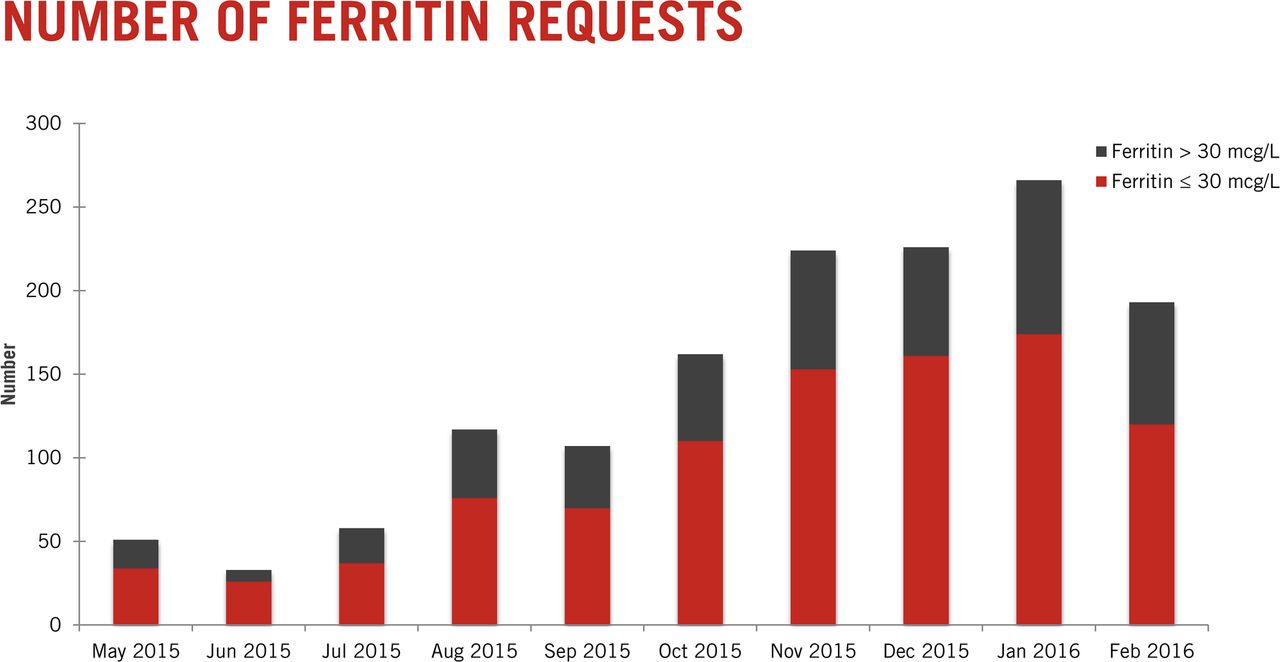
Number of ferritin requests
Patient information
An audit of 24 iron deficient pregnant women was undertaken. Women were contacted approximately 3 weeks after iron deficiency had been identified. Of the 21 women successfully contacted by telephone, 20 had bought and were taking oral iron as recommended by the clinical team. Only 14 (67%) had received the oral iron prescription handout, all of whom found it helpful. If they indicated that it was helpful, patients were asked how they found it helpful, with some of the responses noted in Table 1. Clinical staff were also invited to provide written feedback during the implementation phase, with comments on the tools developed also recorded in Table 1.
Feedback from Staff and Patients on Resources
Transfusions
There was considerable variability month to month in the number of transfusions and the proportion of transfusions that were single unit transfusions, in large part due to the occurrence of large volume PPH. Despite this, the number of transfusion episodes decreased from a mean of 13.1 per month to 8.9 per month (p=0.008), corresponding to a reduction in transfused units from a mean of 26 to 17 per month (p=0.03). There was also an increased proportion of single unit transfusions, from 79/223 (34.4%) to 31/62 (50%, p=0.037) before and after the project interventions and implementation of a hospital-wide single unit transfusion policy (Figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Total and single unit transfusions
Although our educational strategies encouraged clinicians towards a restrictive transfusion strategy, with transfusion generally considered appropriate when Hb <70 g/L, there was no strict cut-off, with clinicians encouraged to consider patient symptoms in the decision to transfuse. Rates of transfusion with Hb <70 g/L remained stable before and after our interventions (32% v 37%, p=0.4). The strategy of considering symptoms after single unit transfusion may have had an impact on transfusion targets, with post transfusion Hb <90 g/L being found in 49% of cases prior to intervention, compared with 61% afterwards (p=0.08).
Lessons and limitations
Conventional practice in obstetrics acknowledges iron deficiency anaemia as a potential cause for morbidity. However, obstetric management guidelines recommend screening pregnant women for anaemia with a FBC only and do not suggest universal screening with ferritin or universal iron replacement in high income countries.10–12 This is despite prior work demonstrating the potential to reduce transfusion with antepartum identification and management of iron deficiency.16 The prevalence of iron depletion is high in young women and pregnancy, particularly during the third trimester when there is an additional strain on iron stores.17 ,18
In response to our own data showing a significant rate of anaemia at delivery (which increased the risk of transfusion postpartum) and new PBM Module 5 guidelines, we implemented a multifaceted quality improvement approach. Examining our processes demonstrated multiple opportunities for improvement, including not identifying pregnant women at risk, lack of appropriate pathology studies to demonstrate iron deficiency, and a failure to intervene when iron deficiency was confirmed. In addition, transfusion practice was liberal, not responding to mounting evidence of lack of efficacy, and potential for harm with such a strategy.
Our interventions were a combination of systemic changes and education. Systemic changes included routine antenatal ferritin testing, the development of patient information and iron prescription forms, standardised management algorithms at antenatal clinics, and intravenous iron infusions available within the antenatal clinic. The results showed a clear benefit in terms of the rate of anaemia at delivery and the number of transfusions. The algorithms and patient information have been made publicly available through the Blood Service, enabling easy and rapid adaptation for other institutions. The results are limited by relatively short follow up, although the systemic interventions have shown considerable benefit and have been embedded within clinical practice.
Education reinforced the systemic changes and was well-accepted by clinical stakeholders. Transfusion practice based on transfusion thresholds did not show a statistically significant benefit, and is the one area within our process completely dependent on education of clinicians alone. Some recidivism is frequently seen in quality improvement strategies reliant solely on education once the initial enthusiasm for intervention wanes. It is hoped that as clinicians get more comfortable with managing anaemic women for short periods of time while their haemoglobin increases, the transfusion thresholds may improve.10 The results of our intervention are less dependent on education than the antenatal haemoglobin optimisation interventions.
Our project is also limited by a lack of formal cost benefit analysis. Red cells are expensive to acquire and administer, and a direct cost saving will occur from reduced usage. With a reduction in red cell transfusions of nine units per month, there are direct cost savings of $401.94 per unit19 (∼$3,617.46 per month), and the cost saving is even higher if administration costs were taken into account.20 ,21 Expenditure on iron, particularly intravenous iron, offsets some of these savings, with 1000 mg of ferric carboxymaltose costing $306.96,22 and additional administration costs expected. Cost of increased ferritin testing is another direct cost. Indirect costs include time lost for infusions, side effects of iron therapy, and risks of acute transfusion reactions. Importantly, any formal cost benefit analysis should include an assessment of the effect of anaemia on the infant and quality of life for the mother.
The strategy for iron replacement in this project included all women with low iron stores, rather than just those with anaemia. There is conflicting data on the impact of non-anaemic iron deficiency in women,23 ,24 and further research in pregnancy to determine the effect of non-anaemic iron deficiency on fetal welfare is justified. Although our project has shown benefits, there are opportunities to refine the process. Further research may be useful to determine the optimal times to assess iron stores during pregnancy. It is anticipated that more active intervention in early pregnancy with oral therapy may reduce the need for intravenous iron later in gestation. Better awareness of iron deficiency in primary care and proactive screening for women considering pregnancy would also offer an opportunity for further intervention. Strategies to improve the prescribing of blood in postpartum women are also warranted and may need to focus on physician perceptions and experience.25 At postpartum, there are many conflicting causes of symptoms that may be attributed to anaemia and further work could focus on identifying symptoms most specific to anaemia to develop more objective criteria for transfusion prescription.
Conclusion
A combination of systemic changes and education that are aligned with PBM Module 5 Obstetrics guidelines were well-accepted by clinical stakeholders, which led to a practice improvement embedded in practice. This CPI project demonstrated the potential to improve patient blood management in obstetrics, reduce anaemia and transfusions by active antenatal interventions. In the process, strategies and tools were developed that may translate readily into other institutions.
Acknowledgments
We thank the maternity staff for their support in implementation of tools and embedding in practice. We also thank the patients who engaged in the project.
Australian governments fund the Australian Red Cross Blood Service to provide blood products and services to the Australian community.
Footnotes
Declaration of interests None declared.