Article Text

Abstract
Asthma is the most common chronic paediatric disease treated in the emergency department (ED). Rapid corticosteroid administration is associated with improved outcomes, but our busy ED setting has made it challenging to achieve this goal. Our primary aim was to decrease the time to corticosteroid administration in a large, academic paediatric ED. We conducted an interrupted time series analysis for moderate to severe asthma exacerbations of one to 18 year old patients. A multidisciplinary team designed the intervention of a bedside nurse initiated administration of oral dexamethasone, to replace the prior system of a physician initiated order for oral prednisone. Our baseline and intervention periods were 12 month intervals. Our primary process measure was the time to corticosteroid administration. Other process measures included ED length of stay, admission rate, and rate of emesis. The balance measures included rate of return visits to the ED or clinic within five days, as well as the proportion of discharged patients who were admitted within five days. No special cause variation occurred in the baseline period. The mean time to corticosteroid administration decreased significantly, from 98 minutes in the baseline period to 59 minutes in the intervention period (p < 0.01), and showed special cause variation improvement within two months after the intervention using statistical process control methodology. We sustained the improvement and demonstrated a stable process. The intervention period had a significantly lower admission rate (p<0.01) and emesis rate (p<0.01), with no unforeseen harm to patients found with any of our balance measures. In summary, the introduction of a nurse initiated, standardized protocol for corticosteroid therapy for asthma exacerbations in a paediatric ED was associated with decreased time to corticosteroid administration, admission rates, and post-corticosteroid emesis.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Asthma is the most common chronic disease of childhood, and accounts for more emergency department (ED) visits than all other chronic paediatric diseases combined.1 Systemic corticosteroids provide anti-inflammatory effects and acutely improve responsiveness to beta agonists.2 Children presenting to the ED for acute asthma exacerbations are treated with beta agonists and systemic corticosteroids. Rapid corticosteroid administration is associated with improved outcomes for patients with asthma exacerbations.3 Prior to 2007, the ED asthma pathway in our freestanding children's hospital included nurse initiated beta agonist therapy by protocol without a physician order, but corticosteroids were administered only after physician evaluation and a written order.
In multidisciplinary feedback sessions, we identified the lack of a nurse initiated protocol for corticosteroids, lack of standardisation in the type of corticosteroid, and lack of standardised dosing of corticosteroids as significant barriers to decreasing the time to steroid administration for asthma patients. We had administered beta agonists by unit dose (7.5 mg for children <30 kg, and 15 mg for larger children), but we administered corticosteroids on a less standardised milligram per kilogram basis. The corticosteroid of choice was either prednisone tablets or prednisolone liquid (depending on age), at 2 mg/kg/day (maximum dose 60 mg per day) to complete in a five day course. There was a consensus among ED physicians and nurses that we could improve our timeliness of care to our ED patients with acute asthma exacerbation. Therefore, we formed a multidisciplinary team of ED physicians, ED nurses, pulmonologists, hospitalists, and pharmacists to address the problem.
The aim of our project was to decrease the time from patient arrival to corticosteroid administration for patients in the ED with acute asthma exacerbations, and to measure the secondary effects of this intervention on patient outcomes.
We performed this intervention at an urban, academic, tertiary children's hospital (Children's National Health System in Washington, DC), with an annual ED volume of approximately 87 000 patients. This ED serves large numbers of patients living in the inner city who are uninsured or have state sponsored insurance (Medicaid), both of which place patients at risk of poor medical management for their asthma.
Background
Corticosteroids are a mainstay for acute asthma exacerbation treatment. However, previous studies reported low adherence to evidence based guidelines in the provision of systemic steroids for acute asthma exacerbation.4 ,5 A one or two dose course of oral dexamethasone has equivalent efficacy to a 5 day course of oral prednisone/prednisolone for the treatment of acute asthma exacerbations, as measured by rates of return for unscheduled care.6 ,7 ,8 In other ED settings, early dosing of corticosteroids, and the use of a clinical pathway for asthma management in the ED, have each been associated with improved outcomes.3 ,9 ,10 Steroid administration for acute asthma exacerbations is delayed during periods of increased ED crowding, supporting the use of giving steroids from triage to reduce the variation of administration timing caused by high patient volume in the ED.11 ,12 Anecdotally, we also noted vomiting after oral prednisolone in a substantial number of cases.
In February 2007 we revised our asthma pathway to incorporate a nurse initiated standing order for the administration of a weight appropriate dose of oral dexamethasone using three weight ranges. In order to measure the effect of the pathway on patient centred outcomes, we compared patients treated under the new pathway to those treated under the old pathway over two consecutive 12 month periods. We hypothesised that ED patients with moderate to severe asthma exacerbations in the new pathway would experience a decrease in the time from triage to corticosteroid administration, a decrease in ED length of stay (LOS), a decrease in admission rates, and a decrease in the rates of emesis. As reducing hospital admission rates might impact rates of return to the ED after discharge, we measured returns to the ED within five days as a balance measure.
Baseline measurement
In order to minimise the confounding effect of the seasonal variability of asthma and ED operations, we chose to include a random sample of children over each 12 month period in the baseline and intervention periods. We scheduled the implementation of the modified pathway for February 2007. We compared treatment of patients during the 12 month interval starting March 2007 to the treatment of those seen during the 12 month interval immediately prior to implementation. We measured the change in a process measure (primary outcome: time from triage to corticosteroid), outcome measures (emesis rate, ED length of stay for children not admitted to the hospital, and admission rate), and three balance measures (unplanned ED return visits for asthma care within five days, ED return visit with admission, and unscheduled follow up visits for asthma to the hospital's primary care clinics).
To obtain baseline performance, we manually collected data from scanned paper charts and the electronic tracking board. We abstracted data to determine the triage time, corticosteroid administration time, ED length of stay (LOS) from arrival to discharge, ED disposition, occurrence of emesis after steroid administration, and any return visits to the ED. Given the high volume of patients with acute asthma exacerbations seen at the ED annually, we obtained a random subset of charts from the baseline and intervention periods. We assessed the chart of every eighth patient with a discharge diagnosis of asthma for eligibility; if ineligible, we assessed the previous chart.
Our baseline time to corticosteroid administration was 98 minutes (standard deviation 65 minutes). We believed that our intervention could decrease this time by at least 15 minutes. To detect a decrease of 15 minutes, 336 patients were required in each group to achieve 80% power in a two sided test with an alpha of 0.05. A run chart was constructed to determine the process stability of the time to corticosteroid administration over time during the baseline phase; mean times for subgroups of 14 consecutive patients were used to create a run chart with 21 points; special cause rules included:
(a) ≥6 consecutive points in an increasing or decreasing direction
(b) Above or below the standardised limits for the number of allowable runs for a set number of observations
(c) ≥8 points in a run.13
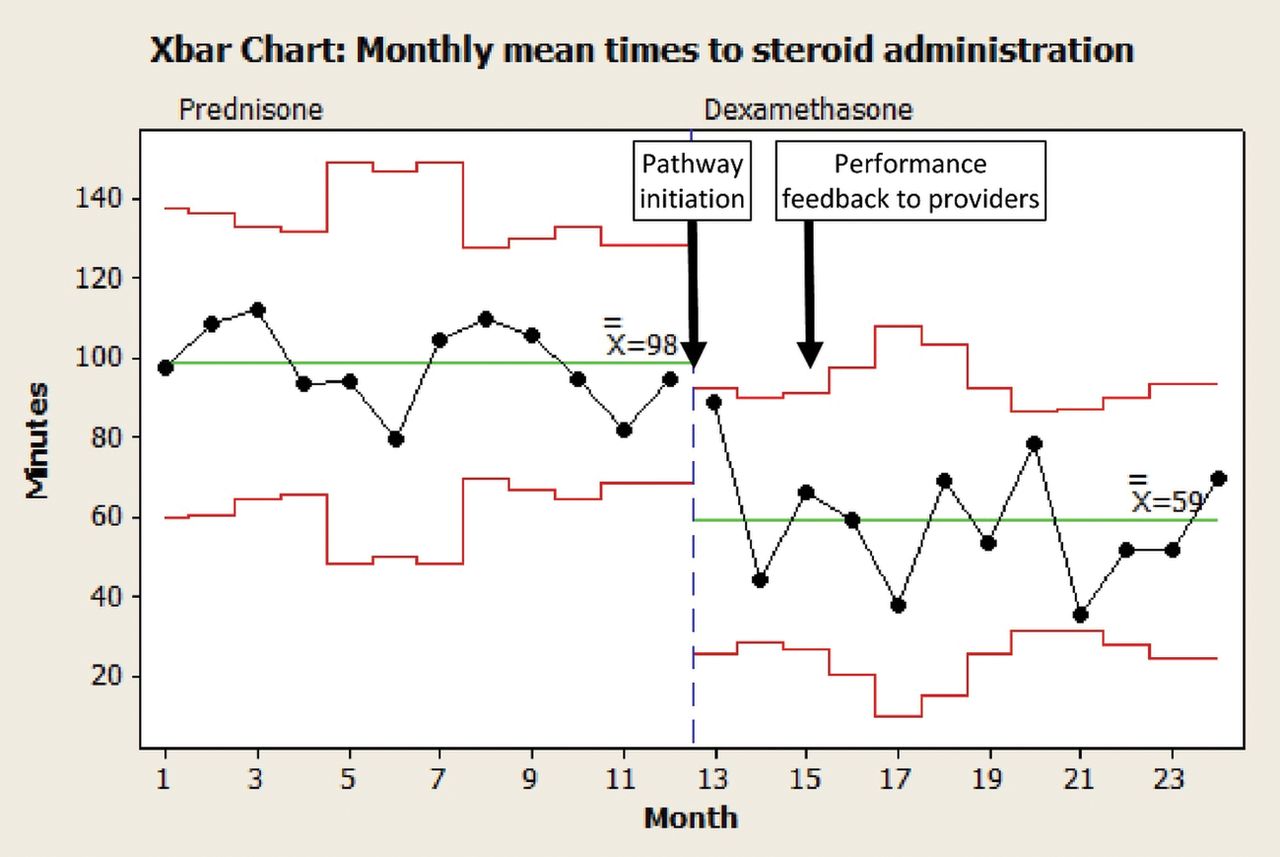
No special cause variation occurred during the baseline phase (figure 1), and our mean time from triage to corticosteroid administration was 98 minutes. The results of our other baseline measures can be seen in table 2.
{kind=link}
Statistical process control (Xbar) chart of the mean times to steroid administration in the baseline (Prednisone) and intervention (Dexamethasone) phases.
For our primary outcome during the intervention phase, we performed an interrupted time series analysis starting one month after the intervention, using a Shewhart X bar chart to determine if special cause variation had occurred, for the monthly mean time to corticosteroid process during the baseline phase versus the intervention phase. The special cause rules used included:
(a) Single point outside control limits of three standard deviations
(b) Eight points in a row on same side of centre line
(c) Six points in a row, all increasing or decreasing
(d) Two of three consecutive points that are >2 standard deviations from centre line.14
During the intervention period, nursing staff were provided aggregate feedback on time from triage to corticosteroid administration approximately every three months.
We analyzed secondary outcome time interval data using the student's t test for normally distributed data, and the Mann Whitney U test for non-normally distributed data. We compared proportions using the chi square. The level of statistical significance was 0.05. Statistical analyses were performed using Microsoft Excel (version 2003) and SPSS Statistics 17.0 (SPSS Inc., Chicago, IL).
We used three balance measures to determine if unforeseen consequences were affecting the patients in the baseline versus the intervention period. First, we assessed the proportion of unplanned ED return visits (ie “bouncebacks”) for asthma care within five days of the original ED visit for those children who were discharged from the ED. Second, we checked the proportion of patients who were discharged from the ED and had been admitted on their bounceback visit to the ED within five days of the original ED visit. Third, because some caregivers might take their child to an alternative care location for an unscheduled asthma follow up visit, we calculated the proportion of discharged children who had unscheduled follow up visits (ie because they were sick, which is not the same as the routine scheduled follow up visits that are recommended with every ED patient discharged with asthma) to the hospital's primary care clinics within five days of the original ED visit.
The Institutional Review Board at Children's National Health System approved this study.
Design
Our team modified the existing asthma pathway by interdisciplinary consensus of ED physicians, pulmonologists, hospitalists, pharmacists, and ED nurses, after a review of relevant literature and consideration of ED logistics. We shared the modified pathway with ED physicians through staff meetings and emails. We educated ED nurses using in-service education in small groups over several months. After several rounds of iterative feedback and changes to ensure feasibility for frontline clinical providers, we finalised a version of the new asthma pathway.
The new asthma pathway was provided as a single page flow diagram and two pre-printed order sheets (one for children <30 kg and one for children ≥30 kg), with dosing recommendations for albuterol, ipratropium, and dexamethasone (appendix 2). Key components of the pathway that were different than previous practice included:
Nurse initiated orders for corticosteroids
Standardisation of the choice of corticosteroids to dexamethasone
Three weight based dose ranges to eliminate the need for dose calculations
Dispensing a second dose of dexamethasone from the pharmacy for home use prior to discharge.
Nurses were encouraged to administer an initial combined unit dose of albuterol and ipratropium, and a single dose of dexamethasone, to patients eligible for the clinical pathway, based on strict inclusion criteria, exclusion criteria, and patient weight range. Patients aged one to 18 years with a chief complaint of acute asthma were included if they had moderate to severe asthma, as defined by an asthma score of four or greater on the modified paediatric asthma score. The asthma score uses five components, each of which are scored from zero (absent) to two (severe); scores can range from zero to 10 (appendix 1). Patients were excluded if they had received systemic corticosteroids within the previous 24 hours, or if they required intravenous corticosteroids in our ED. Dexamethasone was dosed as follows:
<10 kg received 6 mg
10 kg to <20 kg received 12 mg
≥20 kg received 16 mg.
Additional orders, such as home medications or additional doses of albuterol, were ordered by the physician. Our team pilot tested the order sheets on a few patients to ensure that the correct wording, content, and dosages were appropriate for patients with asthma exacerbations.
By standardising the corticosteroid drug and dosage, our multidisciplinary group believed that this would empower our nurses in triage to safely and efficiently administer therapy. We anticipated that the pathway might be used less frequently when large numbers of patients arrived to triage simultaneously, as the ordering and obtaining of the corticosteroid would add time to the triage processing time for each asthma patient. Given the pressure to maintain rapid triage throughput for the safety of all patients in the ED, we recognised this as an inherent limitation to a triage based intervention. In response, we provided an option for the bedside nurse to administer the dexamethasone if the triage nurse was too busy.
Strategy
After several months of project design, feedback, and education, we implemented our pathway on the first day of a new month (February 2007). We posted the asthma scoring system (appendix 1) in all triage areas, and had the ordering forms (appendix 2) placed in all triage and treatment areas of the ED. We met with our administrative assistants to assure that the forms would remain stocked in the appropriate areas, given our paper based ordering system. Nursing educators worked with triage nurses and bedside nursing providers to assure they understood the new protocol for their patients. They also verified that they understood the new dosing regimens. Additionally, if physicians went off of the protocol in ordering a different corticosteroid (eg prednisolone), or different dosing than the set three dosing levels, ordering physicians received real time feedback and correction from the nurse, pharmacist, or available nursing or physician ED leadership. This system of correcting orders was intended to be non-punitive in nature, and helped to fill in any educational gaps from our initial training in the protocol. Initially on a daily basis, then on a weekly basis for the first two months, and afterwards on a monthly basis, members of the quality improvement team met to discuss informal feedback they had received from frontline providers on how to make the process easier to perform. As data was manually collected with paper charts, the analysis of the project's performance happened approximately once per quarter. We communicated the collective performance for our primary aim to our ED nurses and physicians using email, staff meetings, and shift change huddles in the ED.
Results
Asthma was the discharge diagnosis in 2785 visits between 01 February 2006 and 31 January 2007 (baseline), and 3377 visits between 01 March 2007 and 28 February 2008 (intervention). We reviewed 752 randomly selected patient charts in the baseline group and 756 randomly selected patient charts in the intervention group to assess study eligibility, and reach our target of 336 patients per group. Patients were most commonly excluded from the study for asthma scores less than 4 (mild asthma) and age less than 12 months. Baseline demographics for both groups, including initial asthma score, had no significant differences (see table 1).
Demographics and initial asthma scores of patients included in the analysis
Of the 336 patients included in the baseline group, 316 (94%) received prednisone or prednisolone for moderate to severe asthma exacerbation, one (<1%) received dexamethasone, and 19 (5%) did not receive any corticosteroid. In the intervention group, 333 patients (99%) received dexamethasone, one (<1%) received prednisone, and two (<1%) did not receive any corticosteroid.
For the primary outcome, the time to corticosteroid administration decreased from 98 minutes baseline to 59 minutes in the intervention period (p < 0.01).The X bar chart (figure 1) showed special cause variation in this time metric during the intervention phase in month 14 (the second month after the onset of the intervention), and stabilised to indicate a sustained shift in the process.
For secondary outcomes there were no differences in median ED LOS between baseline and intervention groups (259 versus 263 minutes, respectively; p = 0.90). Of the discharged patients there was also no difference in median ED LOS between baseline and intervention groups (303 versus 283 minutes, respectively; p = 0.08). Admission rates were lower for intervention group subjects (15%) than baseline group subjects (24%) (p <0.01) (table 2). Emesis after steroid administration was noted in 27 patients (8%) in the baseline group, and no patients (0%) in the intervention group (p <0.01) (table 3).
Outcomes:
Regarding the balance measures, there were no worse outcomes of balance measures for the patients in the intervention period. Children returned to the ED for continuing asthma symptoms within five days at similar rates in both groups (table 2). Likewise, there were no significant differences between the proportions of discharged patients who returned within five days and were admitted (table 2). Of the 100 baseline and 110 intervention patients followed at our hospital's primary care clinics, there were more unscheduled follow up visits for asthma in the baseline (22%) than in the intervention group (12%), p = 0.04; the decrease in this rate supports the intervention decreasing unscheduled follow up patients, as patients historically attend these visits if they are doing worse clinically (See supplementary - appendices 1 and 2).
supplementary appendices
Lessons and limitations
Our primary lessons learned were around the need for a multidisciplinary buy in for the project, and the need for standardisation of ordering.15 By engaging with stakeholders from all processes in the care of children with asthma exacerbations, we were able to anticipate potential barriers to the behaviour changes we were promoting with this project. One challenge we experienced was getting all of the ED physicians to change their practice in one of the most common conditions treated in our ED. Given that each physician had a long history of treating children with asthma, implementing change required multiple physician meetings with education and discussion, to get everyone on board. By using a single medication and standardising dosing, we eliminated the cognitive load for physicians in determining both the type and dosage of medicine to order. Because the nurse and pharmacist double check all medication dosages, we decreased their cognitive load as well, and decreased the time required for this step in the process. One major barrier in the design of this project was the concept of nurse initiated therapy. This was a concern by our ED nurses who did not want to be acting outside of their licensed scope of practice. We were able to overcome this barrier by engaging with the hospital's nursing leadership. The reasons that enabled nursing leadership to approve of this step was that all physicians had signed off on the protocol prior to implementation, we had pre-printed order sheets, and the determination that ED nurses would be assessing and not diagnosing children with an established diagnosis of asthma.
This intervention was not associated with an improvement in ED length of stay (LOS). It is possible that time to obtain the home dexamethasone dose from the pharmacy contributed to longer LOS in the intervention group. However, based on frontline user feedback, nurses have appreciated this change of improved access to dexamethasone medication, and anecdotally noted that this helped to decrease the time to administer the medication to patients.
We were able to demonstrate sustained changes for one year. Although we do not have intervening data from the end of this study to today, we can confirm that the same principles are still in effect, with standardised dosages of dexamethasone, established first line beta agonist therapy, and early ordering of dexamethasone. Our ED has sustained these practices due to the value that the project adds to the ED healthcare provider and their patients. We communicated our results to other regional community EDs, who had a history of transferring patients with acute asthma exacerbations to our ED for a higher level of care. Given their strong interest in adapting the change concepts to their ED, and our sustained improvements in our own ED, we shifted our focus from trying to set up a new PDSA cycle within our own ED to helping to spread our intervention to a community ED. Given our limited available time and resources to implement quality improvement projects, we reasoned that a set amount of effort in the community ED would yield greater changes in patient outcomes. After implementing a similar pathway, they achieved a significant decrease in the time to steroid administration from 181 to 86 minutes (Walls T et al; in press). The proportion of asthma exacerbations who required transfer to a higher level of care was also significantly decreased.
Our study had several limitations. Although we detected differences in several important outcomes between the baseline and intervention groups, these observed associations may not necessarily be causally related. However, the statistical process control charts demonstrate the temporal and significant relationship between the start of the pathway and the observed results. Second, we performed this study at a single site with highly invested nursing staff, among a population of largely urban, minority, and disadvantaged patients; thus our results may not be generalisable to other settings. However, we have demonstrated that implementation of this asthma pathway had similar results for children treated at a regional community hospital in which only 25% of patients are paediatric (Walls T et al; in press). Third, we were not able to assess the variety of contextual factors that may have affected ED length of stay, such as the number of patients in the ED at any given time, number of patients seen by the same physician delaying medical assessment after initiating treatment, and pharmacy delay in the availability of the home dose dexamethasone. Finally, when assessing for relapse, we did not measure return visits to other EDs in our region; however, Children's National Health Systems EDs see more than 85% of all paediatric ED visits for asthma in Washington, DC, making it less likely that a significant number of return visits were missed.17 It is also unlikely that any rate of missed return visits is systematically different between baseline and intervention groups. We did not show a statistically significant difference in ED LOS in children who were discharged from the ED between the baseline and intervention groups. ED LOS is confounded by factors that we were unable to control for, such as patient volumes and staffing in the ED.
Conclusion
Among patients with moderate to severe asthma exacerbations in an urban academic paediatric medical centre, a nurse initiated ED clinical pathway was associated with improved times from triage to corticosteroid administration, and a decreased rate of admission to the hospital. We found no harmful changes in any of our return rates that served as our balance measures. A decrease in corticosteroid administration time was our primary aim, and this did not change throughout the project. We believed that this primary aim measure would be most directly affected by changes in our healthcare provider behaviour, and less affected by confounders than other measures in this project.
The improvement in the patient outcome measure, ie a reduced rate of initial hospitalisation, is consistent with the known effect of corticosteroids and the improvement we achieved in our process measure: a reduced time to corticosteroid administration. A previous Cochrane review found that corticosteroid administration within one hour of ED arrival significantly reduced hospital admissions of patients with acute asthma, particularly those with more severe asthma.3 Zemek et al performed a similar study in a large tertiary care children's hospital in Canada;16 they demonstrated that nurse initiated corticosteroids for acute asthma before physician assessment reduced LOS and admission rates. However, that study was limited by the sampling period, which did not account for seasonal variation in asthma triggers and ED operations. Furthermore, Zemek at al did not measure rates of emesis or return ED visits within five days.
No children vomited in the intervention (dexamethasone) group. This is consistent with previous studies that have shown a marked decrease in vomiting in the ED when dexamethasone is used instead of prednisolone in children with acute asthma exacerbations.6 It is also supported by the fact that dexamethasone is known to have antiemetic properties.18 We used the parenteral formulation of dexamethasone and administered it orally (in young children) or via oral tablets (in older children), resulting in a decreased volume of medication compared to weight equivalent dosing of prednisolone.
In our study, as in other studies comparing the use of dexamethasone versus prednisolone for treatment of acute asthma exacerbations, there was no significant difference in the rate of children who returned for an unscheduled visit to our ED.6 ,8 One possible explanation for this finding is that the decreased rate of vomiting, and decreased number of doses required when treated with dexamethasone, may have resulted in improved compliance with oral corticosteroid therapy.
In summary, initiation of a new ED asthma care pathway distinguished by nurse initiated administration of weight based unit dosing of both beta agonists and dexamethasone was associated with significant decreases in time to corticosteroid administration, rates of vomiting, and rates of hospital admission among a population of patients with moderate to severe exacerbations treated in the ED of a large urban paediatric medical centre. The long term implications of this project are still in place today, likely due to the demonstrated improvements in patient based measures, and the ease that healthcare providers have when using this new protocol. Our standardised protocol would likely be replicable and generalisable to other ED settings, and a community based ED has already demonstrated similar results to our findings using the same protocol (Walls T et al; in press).
Acknowledgments
Not applicable.
References
Footnotes
Declaration of interests Nothing to declare
Ethical approval The Institutional Review Board at Children's National Health System approved this study.