Article Text

Abstract
There is variation in pediatric asthma management in the outpatient setting. Adherence to national asthma guidelines provides a systematic standardized approach to asthma management. There is a gap between usual and guideline-consistent asthma care in resident clinics. Practice improvement modules aimed at improving resident physician adherence to asthma care guidelines have not been consistently utilized and have not yet been studied.
Our aim was to increase guideline consistent care in our pediatric resident clinic in a twelve-month period via increasing performance on the following measures to 75%: spirometry testing; influenza immunization recommendation; level of control assessed through the use of a standardized questionnaire; appropriate medications per national guideline; and use of written asthma action plans.
A summarized pediatric-specific version of the National Heart Lung and Blood Institute National Asthma Education and Prevention Program Expert Panel Report 3 (NHLBI EPR-3) guidelines was made readily available to increase provider education. Electronic health record (EHR) enhancements included adding templates to create standardized asthma action plan, asthma control test and a pediatric asthma controller medication order-set. We also addressed the education of patients by simplifying patient instructions. We monitored our progress through the use of an online practice improvement module.
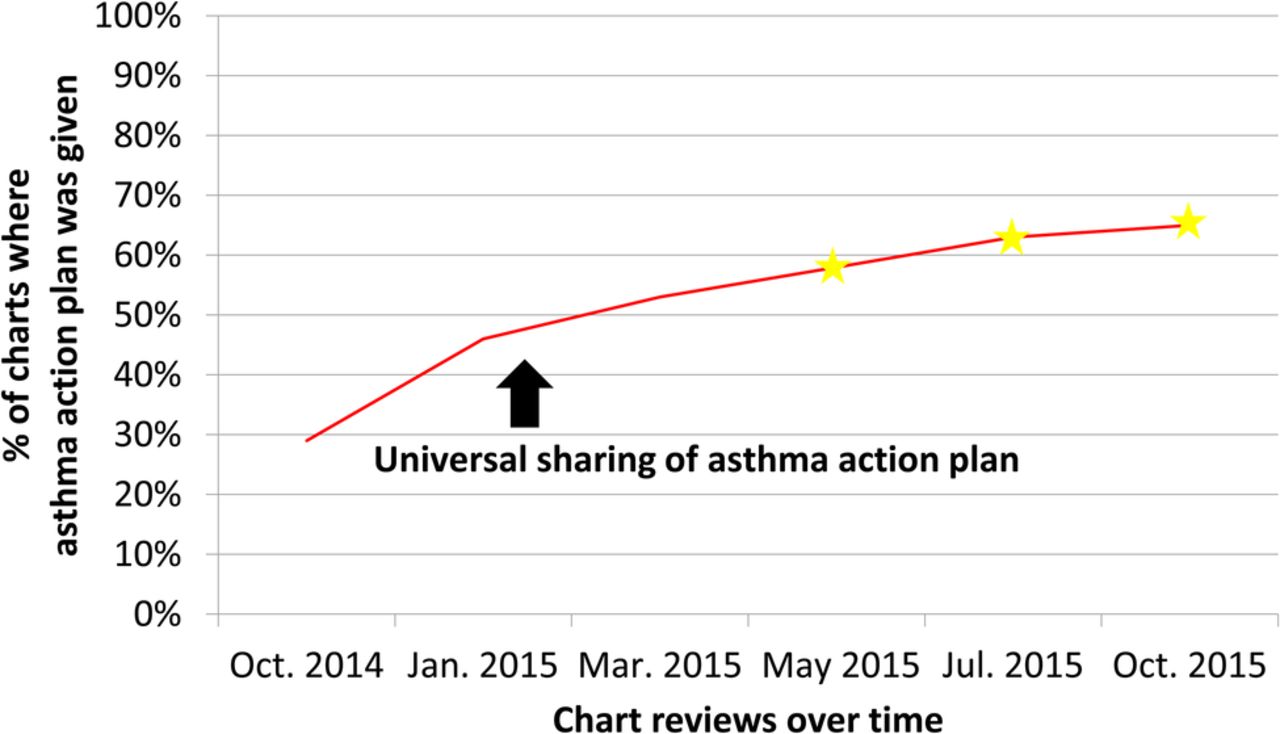
We found statistically significant increases in use of a standardized instrument to determine level of control (20% to 81%); recommendation of influenza immunization (56% to 97%); use of national medication treatment guidelines (28% to 98%); distribution of asthma action plans (29% to 65%); and provision of asthma self-management education (35% to 74%).
Standardizing the implementation of national guidelines for pediatric asthma through the use of a practice improvement module and electronic health records improved adherence to guidelines. The module allowed us to identify goals for improvement, collect and analyze our group performance data over time, assess the impact of each change, and redesign our process. Improving adherence to national pediatric asthma care guidelines is especially important in settings such as resident teaching clinics which provide care to underserved populations at higher risk for complications related to asthma.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Although the current National Heart Lung and Blood Institute National Asthma Education and Prevention Program Expert Panel Report 3 (NHLBI EPR-3) guidelines were first published in 2007, general pediatricians do not consistently adhere to them.1 Poorly controlled asthma can contribute to avoidable emergency room visits and hospitalizations. Patients with asthma seen at university-based clinics may be more likely to have increased health care utilization compared to patients with asthma seen in private practice and community based health clinics.2
Pediatric residents have been shown to not consistently adhere to national asthma care guidelines regardless of level of training.3 Our baseline data demonstrated that pediatric residents in our teaching clinic at the University of California Davis Health System (California, United States) adhered to the national asthma care guidelines 20-35% of the time in terms of obtaining relevant history to diagnose severity of asthma, recommending spirometry testing, recommending influenza vaccine, using a standardized instrument to assess level of control, referring to national asthma care guidelines for medication dosage, and providing an asthma action plan. Our aims in a 12 month period were to increase performance on the following measures to 75%: spirometry testing; influenza immunization; level of control assessed through the use of a standardized questionnaire; appropriate medications per national guideline; and use of written asthma action plans.
Our key interventions were provider education, electronic health record modifications and patient education. Our team consisted of three general pediatric faculty staff members, one bio-statistician, and one pediatric resident.
The study was conducted in a resident continuity teaching clinic that occurs four afternoons a week, ranging from five to seven patients per resident per afternoon and an average of four to five residents per afternoon. During the course of our study, there were a total of 6168 pediatric resident office visits. Of these patient encounters, any office visit which involved a patient younger than 20 years old with a new diagnosis or known diagnosis of asthma was included in our study, if the patient was seen for an annual exam or for a respiratory complaint. This resulted in 305 patients included in our study with a known diagnosis of asthma. Level of control was assessed by frequency of symptoms and level of impairment on a controller medication.
Background
Asthma is one of the most common pediatric chronic diseases with prevalence rates of 6% to 13%. Asthma is also one of the most costly pediatric diseases, with over $1 billion spent on asthma care in 2010 alone, and one out of every three children with asthma visit an emergency room because of an asthma related issue.4 Patient populations of low socioeconomic status are at higher risk for emergency room visits and hospitalizations due to poorly controlled asthma.5 Establishing a quality improvement (QI) intervention for asthma care in the outpatient pediatric resident clinic setting has been shown to result in increased use of asthma action plans, classification of asthma severity, and controller medications.6 ,7
A standardized systematic approach to implementing the use of asthma management guidelines results in increased adherence to national asthma care guidelines and decreases in medical service utilization, such as emergency department visits and hospitalizations.8 Multi-provider practices such as resident-based teaching clinics may lack the resources and procedures necessary to track progress of QI interventions. A web-based practice improvement module (PIM) provides step-by-step guidance for developing a QI intervention although assessments of the effectiveness of such modules have not been widely published.9
Baseline measurement
For this project, a practice improvement module was used every two months to assess pediatric residents providing guideline-consistent care in an outpatient clinic setting. The module provided a questionnaire to assess whether doctors were adhering to guidelines by examining electronic medical charts for documentation of spirometry ordered, influenza immunization recommendation, use of a standardized instrument such as the childhood asthma control test or asthma control test, prescription of daily asthma medication dosage based upon national asthma care guidelines, and providing written asthma action plans.
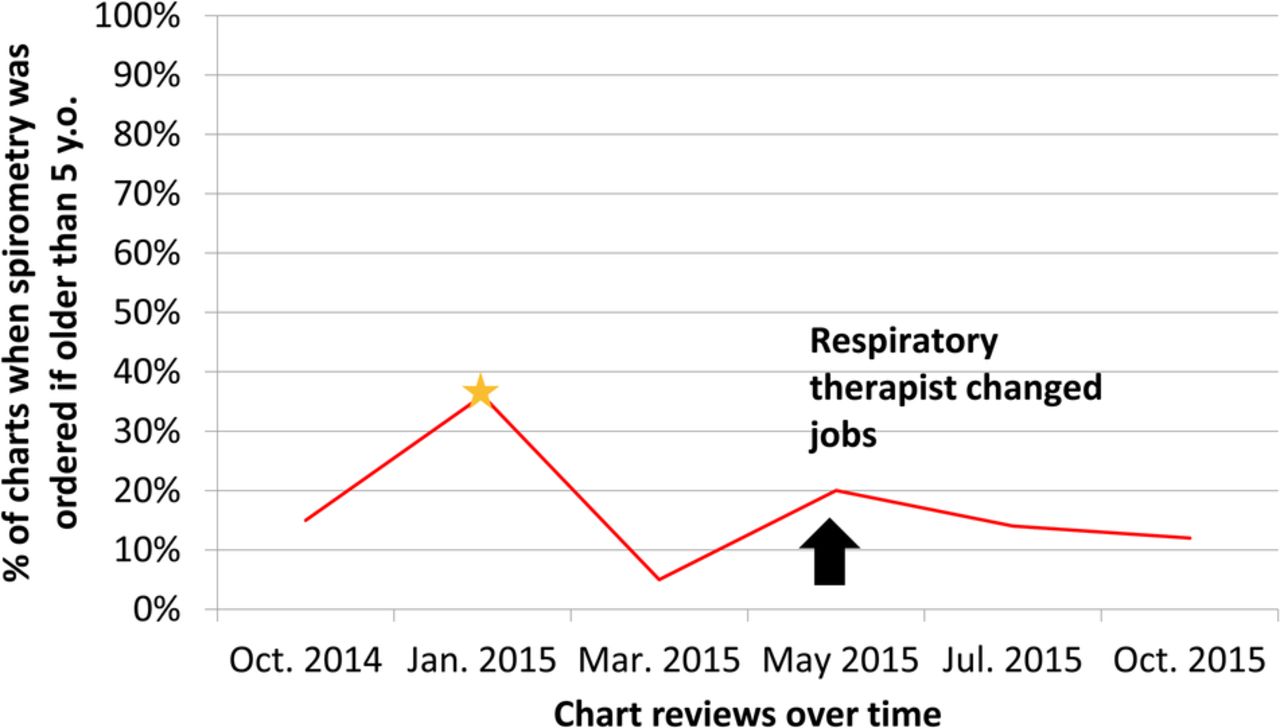
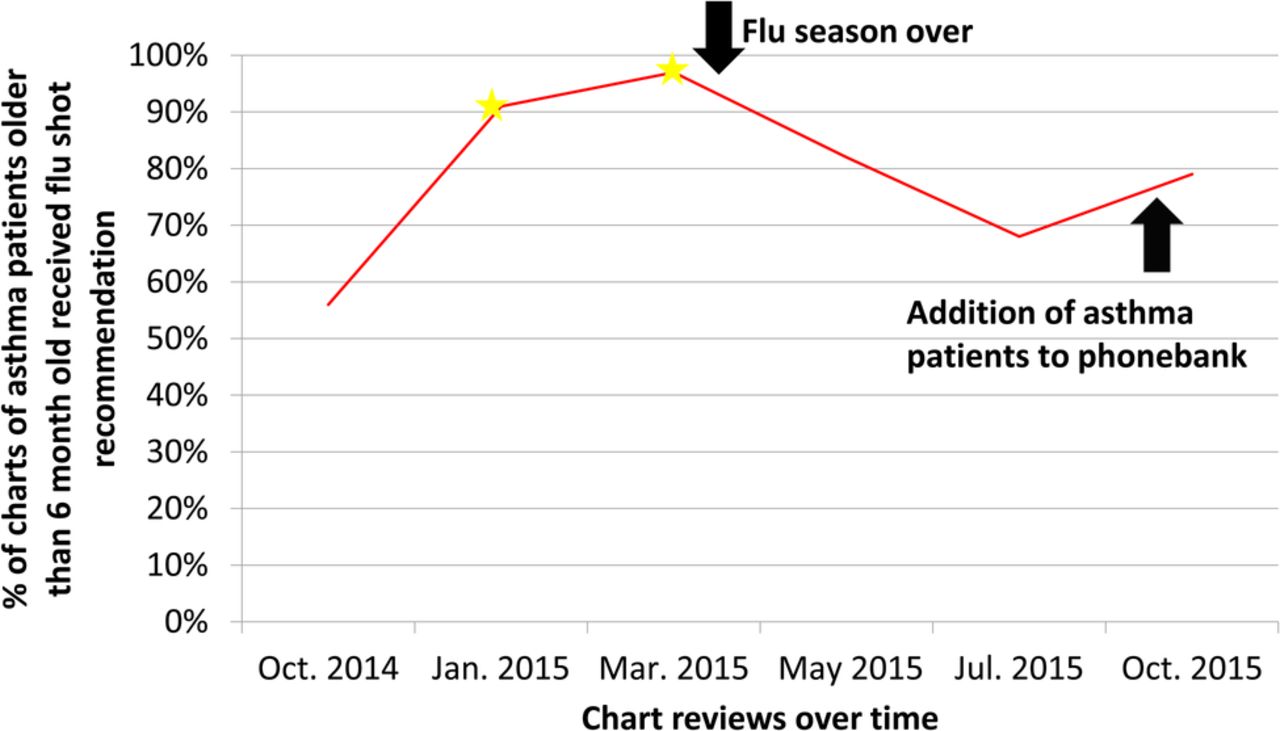
These five process measures were reviewed every two months via a practice improvement module that reviewed physician notes in patient charts based upon the questionnaires provided by the module which were filled out by the pediatric residents. Our baseline data showed that residents ordered spirometry 15% of the time, recommended the influenza immunization 56% of the time, used a standardized instrument to determine level of control 20% of the time, used the national medication treatment guideline 28% of the time, and distributed asthma action plans 29% of the time.
Design
We used the American Academy of Pediatrics' Education in Quality Improvement in Pediatric Practice (EQIPP) asthma module because the use of an established PIM would allow us to collect and review data in a standardized and reproducible manner. The PIM includes a questionnaire that evaluates measures which reflect the goals of our project including such as use of obtaining relevant history, spirometry, administration of influenza vaccination, use of a standardized instrument to assess level of control, use of NHLBI EPR3 guideline for medication dosage, and provision of written asthma action plans. Data from the questionnaire filled out by individual residents were entered into the online PIM database following each Plan-Do-Study-Act (PDSA) cycle. For all outcomes, pairwise between-time point comparisons (using baseline as the reference group) of process of care outcomes were performed in SAS Version 9.4 using logistic regression. Dunnett-Hsu confidence intervals were used to adjust for multiple pairwise comparisons.
Upon reviewing our baseline data, a root-cause analysis was performed with residents regarding reasons for variation in their group asthma practices. We additionally conducted an in-depth literature review on published interventions to improve adherence of clinical guidelines for asthma. Key focus areas included provider education on current guidelines, electronic health record (EHR) interventions and patient education. In terms of electronic health record modifications, several modifications were suggested to ease the workflow of pediatric residents in the outpatient setting such as documentation templates and medication order-sets. A needs assessment telephone survey of a sample of 50 parents of patients in our clinic was conducted to understand their perception of asthma action plans and instructions provided. This feedback was used to further develop our interventions.
Strategy
The aim for the first PDSA cycle was to educate providers the current asthma care guidelines. The change hypothesis was that if the information was made readily available, it would increase provider awareness of the guidelines and hopefully improve adherence to those guidelines. The first PDSA cycle involved educating pediatric residents, general pediatric outpatient nurses and medical assistants on key aspects of asthma diagnosis and management based on the NHLBI EPR-3 asthma care guidelines via an audiovisual three lecture series. A summarized pediatric-specific version of those guidelines was made readily available on a centralized resident resource website and an associated large poster we created as a quick reference to national guidelines was prominently displayed in the clinic. The key messages from the national guidelines that we provided via our poster included: determining asthma severity based on frequency of symptoms, ordering influenza and spirometry test if age appropriate, using a standardized instrument to assess level of control, prescribing controller medications for persistent asthma, and providing and reviewing a written asthma action plan with the family. We also initiated a process of individualized feedback to each resident on guideline consistent care that would occur in every subsequent cycle. Specifically, faculty and project staff would review resident's medical records and PIM data for that period and provide specific suggestions for improving guideline consistent care. Our PDSA cycle 1 data, collected in January 2015, showed that residents showed improvement in ordering spirometry to 36% of the time, recommending the influenza immunization to 91% of the time, using a standardized instrument to determine level of control to 34% of the time, using the national medication treatment guideline to 51% of the time, and distributing asthma action plans to 46% of the time.
The aim of the second PDSA cycle was to improve provider workflow on an electronic health record system. The change hypothesis was if several electronic health record modifications were created to enhance clinical decision support, providers would adhere to the national guidelines more often. Modifications to the electronic health record (EHR) included the creation and dissemination of standardized asthma action plan and standardized asthma history documentation templates with prompts for assessing level of asthma control, impairment, and future risk, creation of a flowsheet to document asthma control scores, and creation of a pediatric asthma controller medication order-set based on recommended doses. We additionally introduced system-level approaches to clinic workflow. These included instructing medical assistants to provide parents with the asthma history questionnaire in examination rooms, teaching nurses to administer peak flow testing prior to the physician entering the examination room, and creating a clinic registry for patients who needed a telephone reminder for influenza immunization if their visit occurred during months when the influenza vaccine for the current year was unavailable. Our PDSA cycle 2 data, collected in March 2015, showed that residents reduced ordering spirometry to 5% of the time, but showed improvement in recommending the influenza immunization to 97% of the time, in using a standardized instrument to determine level of control to 47% of the time, in using the national medication treatment guideline to 97% of the time, and in distributing asthma action plans to 53% of the time.
The aim of the third PDSA cycle was to support parental health literacy, namely a standardized asthma control questionnaire and asthma action plan. The change hypothesis was if the asthma control questionnaire and asthma action plan were more easily understood by patients, this would lead to improved sense of control of asthma disease. A telephone survey was performed on a random sample of 50 parents of patients with asthma seen in our clinic to assess their understandability of the asthma action plan used in our clinic. Our materials were revised to incorporate parent feedback to increase the understandability of the materials for patients, especially those with low health literacy and limited English proficiency. Specifically, medical terms were translated into non-medical language (in both English and Spanish), instructions were simplified, non-necessary text was removed, the font size was increased, and visuals were enlarged.
Clinicians were also instructed to review written asthma action plans, asthma triggers, and appropriate inhaler technique with patients and their parents using the refined materials and terms. Our PDSA cycle 3 data, collected in May 2015, showed that residents improved in ordering spirometry to 20% of the time, but decreased in recommending the influenza immunization to 82% of the time, in using a standardized instrument to determine level of control to 42% of the time, in using the national medication treatment guideline to 61% of the time, and improved in distributing asthma action plans to 58% of the time.
The aim of the fourth PDSA cycle was to focus on a more comprehensive, individualized in-person feedback from a faculty member involved with the project as well as instruction for residents on how to utilize the EHR modifications. The change hypothesis was if the residents understood specifically where they could improve based upon their chart reviews, then they could improve their individual adherence to the national asthma care guidelines. Our intervention was a more thorough feedback session than the previous PDSA cycle, and also provided an opportunity for residents to give the research team feedback as well such as improved methods of distributing information regarding changes in EHR. Because of this feedback, we sent residents an email with screenshots and instructions on utilizing the EHR enhancements to improve clinic workflow and adherence to national asthma care guidelines. Our PDSA cycle 4 data, collected in July 2015, showed that residents decreased in ordering spirometry to 14% of the time, in recommending the influenza immunization to 68% of the time, but improved in using a standardized instrument to determine level of control to 58% of the time, in using the national medication treatment guideline to 79% of the time, and in distributing asthma action plans to 63% of the time.
The aim of the fifth PDSA cycle was to improve upon previous interventions such as the teaching tool for national asthma care guideline and new method to remind patients of influenza vaccine. The change hypothesis was if the visual aid in the clinic workspace was more easily understood by residents, it would encourage them to adhere to national asthma care guidelines, and if patients knew when to come in to clinic for their influenza vaccine, that would also improve level of control of asthma disease. The fourth PDSA cycle feedback from residents regarding the lack of clarity of the visual aid in their workspace (national guidelines quick reference) resulted in the creation of a new visual aid placed in the clinic workspace during the fifth PDSA cycle. We also initiated an intervention for clinic receptionists to provide telephone reminders to come in for influenza vaccine to parents of patients with asthma based upon resident provided feedback with regards to how to improve influenza immunization rates from the fourth PDSA cycle. Our PDSA cycle 5 data, collected in October 2015, showed that residents decreased in ordering spirometry to 12% of the time, but improved in recommending the influenza immunization to 79% of the time, in using a standardized instrument to determine level of control to 81% of the time, in using the national medication treatment guideline to 98% of the time, and in distributing asthma action plans to 65% of the time.
During the duration of the study, medical record reviews were conducted by residents every two months at the end of each PDSA cycle.10
Results
As shown in figures 1 to 5, several key quality measures showed clinically and statistically significant improvements over the course of the interventions. The use of a standardized instrument to determine level of asthma control increased from 20% to 81%, use of national guidelines for treatment increased from 28% to 98%, providing written asthma action plans increased from 29% to 65%, and providing asthma self-management education increased from 35% to 74%. We also noted statistically significant improvement in influenza immunization recommendation during months in which patients with asthma face the highest risks for influenza.⇓⇓⇓⇓⇓
As an exploratory ancillary analysis, we investigated whether improvement in guideline consistent asthma care as a result of our interventions decreased pediatric hospitalization rates in our pediatric clinic patients. We found that hospitalization due to asthma from the pediatric resident clinic patient population was 3.05% out of total asthma hospitalizations during the year of our interventions compared to the previous year which was 3.50% of total asthma hospitalizations (Chi Square P = 0.65).
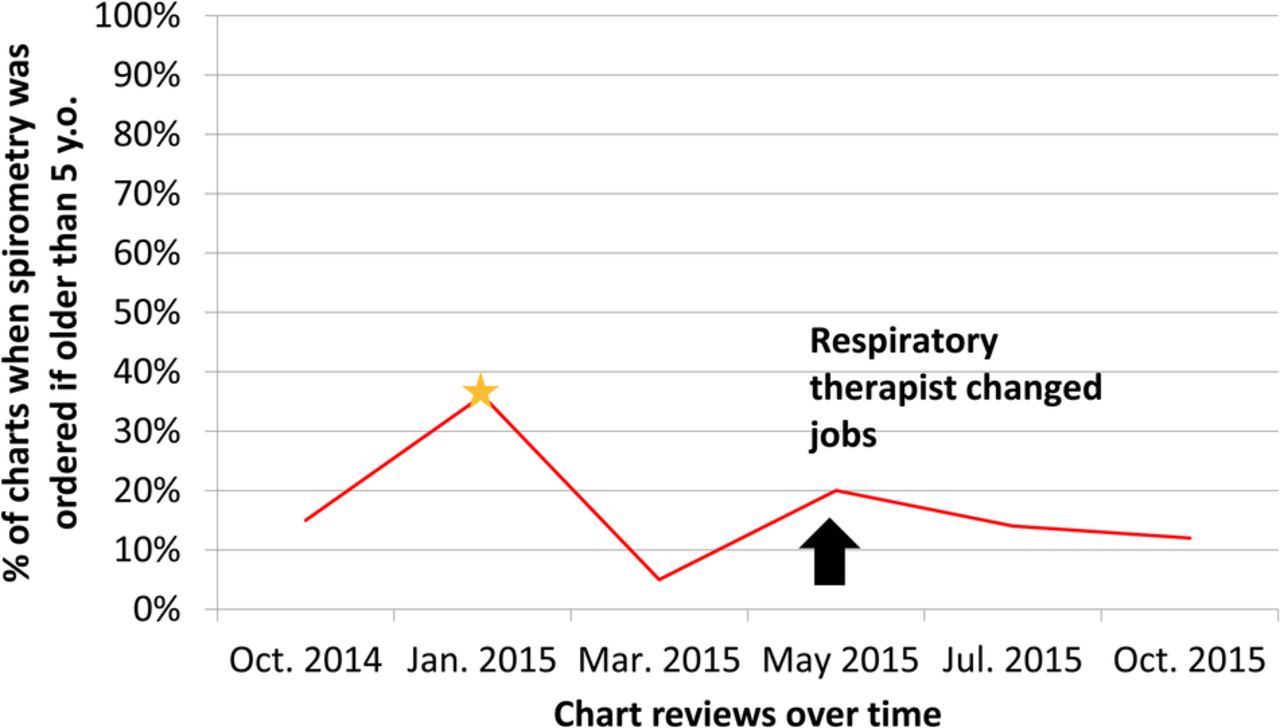
Figure 1. Run chart for use of spirometry. Stars notate any statistically significant improvements compared to baseline.
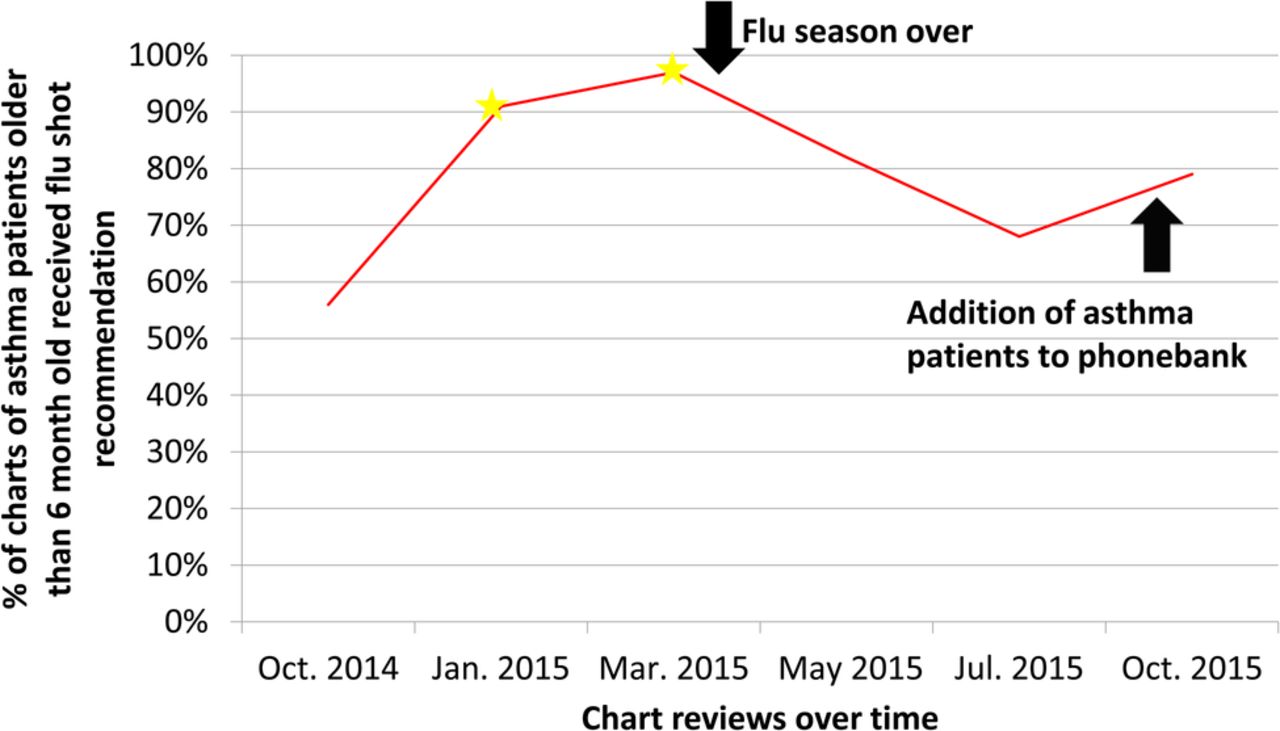
Figure 2. Run chart for influenza immunization recommendation. Stars notate any statistically significant improvements compared to baseline.
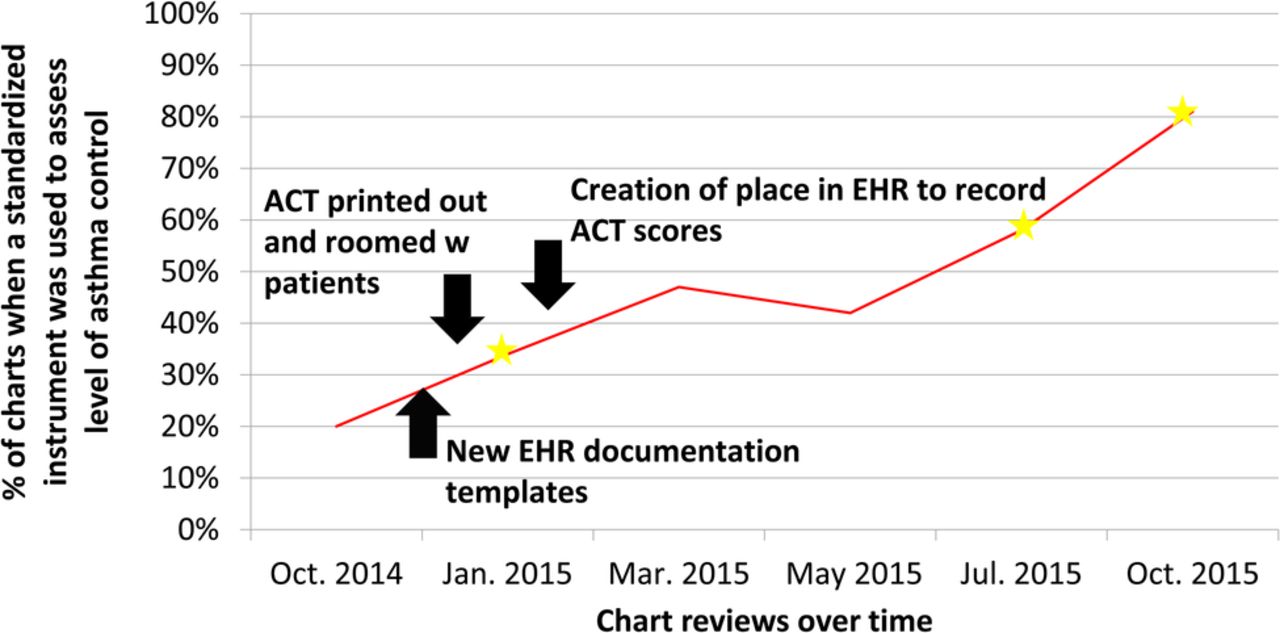
Figure 3. Run chart for use of standardized instrument to assess level of control. Stars notate any statistically significant improvements compared to baseline.
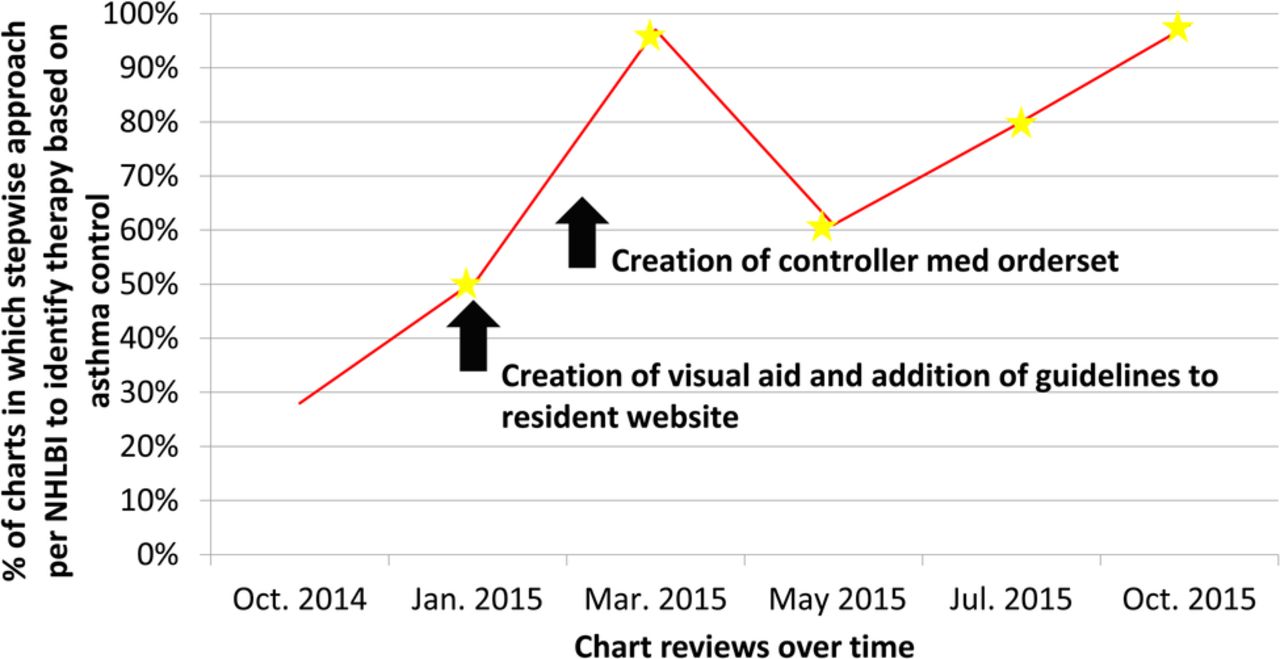
Figure 4. Run chart for medication dosage as per national asthma care guideline. Stars notate any statistically significant improvements compared to baseline.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 5. Run chart for distribution of written asthma action plan. Stars notate any statistically significant improvements compared to baseline.
Lessons and limitations
There were several barriers to implementation of EHR or clinic workflow changes and data collection during the course of our study. During the second PDSA cycle our clinic's respiratory therapist (who was the only qualified person to administer spirometry testing in our resident clinic) left for another job and a successor was not immediately hired. This accounted for some loss of gains in the ordering of spirometry. Measurement of performance was mainly based on residents' self-assessment and self-reports of their own patient records. To minimize the possibility of over-reporting and bias, resident's chart reviews were reviewed by a faculty member who was involved with the project and their answers were discussed on a bi-monthly basis.
Certain PDSA cycles had multiple interventions which may have made it difficult or overwhelmed residents to focus on improving a certain aspect of their asthma management.
Our project was sustained by another pediatric resident who took over the project with the same mentoring team in place; the previous pediatric resident on the team had graduated from the residency training program. The sustainability of our interventions was increased by the addition of standardized tools in our EHR which re-enforced adherence to the national asthma care guidelines by easing the workflow of the pediatric residents. Junior residents frequently learn practice approaches not only from senior residents, which further enhances the sustainability of our interventions. The new pediatric resident plans to continue to collect data and continue to monitor the progress of the pediatric residents and whether or not they adhere to national asthma care guidelines.
Conclusion
Our study demonstrated that the use of electronic health record tools and the AAP's EQUIPP PIM in the context of continuing quality improvement resulted in statistically significant improvement of residents' adherence to key aspects of the NHLBI asthma care guidelines. We found specific improvements in the rates of obtaining pertinent history to stratify severity of asthma, influenza vaccine recommendation, using a standardized instrument to assess level of control, selecting appropriate medications, and distribution of written asthma home management plans.
The PIM provided a standardized questionnaire for bi-monthly chart reviews and provided a centralized portal for data collection. This is an invaluable resource for quality improvement in group practices, including but not limited to resident physician practices. Although our interventions were similar study by Bunik et al 6 in Colorado, the resident physicians in our study used an online based PIM which allowed them to learn crucial QI skills and benchmark their performance over time in relation to their peers.
Our study is generalizable to other pediatric residency training centers at academic teaching hospitals with a resident clinic. Asthma is a common pediatric chronic disease and its management is a core component of pediatric residency training, but how that management is taught varies from institution to institution and could greatly benefit from a standardizing tool such as an online-based practice improvement module. The next step for this project to try to expand the electronic health record interventions to the general pediatric faculty clinic.
Acknowledgments
Special thanks to the pediatric residents at the University of California Davis Health System who participated in this project.
Footnotes
Declaration of interests This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
The authors of this paper have no conflicts of interest.
Dr. Fernandez y Garcia's work on this publication was supported by National Institute of Mental Health of the National Institutes of Health under award number K23MH101157. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical approval Our project was approved by the UC Davis Institutional Review Board as an expedited protocol not requiring informed consent because it was deemed a quality improvement study.