Article Text

Abstract
Medicines reconciliation (MR) is an essential process for patient safety, promoting safer use of medicines with effective communication at the interface, particularly when patients are admitted and discharged from hospital. Much of the work on MR has been focussed in secondary care, however, the principles are equally important in primary care. The aim of the work was to test the Scottish Patient Safety in Primary Care (SPSP-PC) MR care bundle and consider scale up and spread across all NHS Greater Glasgow and Clyde (NHS GGC) GP practices. Care bundles are a quality improvement tool which can drive improvement by standardising processes to deliver optimum care. Pilot work and testing began with 5 GP practices in 2011 and was spread to over 200 practices by 2015/16. A care bundle compliance process measure was measured monthly, with practices sampling 10 patients per month. Practices could view their run charts in real time and identify which measures resulted in “non-compliance” and PDSA cycles were promoted to test and implement improvements. Data was collated at NHS GGC level with an aim of 95% compliance with the care bundle by March 2016. MR care bundle compliance started at 40% (5 practices reporting) in 2011 with final data in March 2016 demonstrating 92% compliance (192 practices reporting). A sustained “reliability” of 92-93% across >200 practices has been observed since January 2015. In conclusion, the bundle was implemented by 97% of NHS GGC GP practices and resulted in process improvements.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Scotland has a population of approximately 5.3 million and healthcare is provided by the National Health Service and delivered across 14 territorial health boards. NHS Greater Glasgow and Clyde (NHS GGC) is the largest health board providing care to a population of ~1.2 million and has ~135,000 emergency admissions per year. There are currently 242 GP practices across NHS GGC with a primary care prescribing budget of ~£242 million. 101 million prescription items are dispensed annually and 59% of over 70 year olds receive 5 or more medicines.
The Scottish Patient Safety Programme (SPSP) is a unique national initiative that aims to improve the safety and reliability of healthcare and reduce harm, whenever care is delivered. One of the aims within SPSP is to reduce the number of adverse events causing avoidable harm to patients through safer use of medicines. Medicines reconciliation (MR) has been a focus of the Acute Adult Scottish Patient Safety Programme for several years. It was identified nationally that MR is also a key feature in primary care and a focus on the MR process in both acute and primary care has safety benefits for both and most importantly, patients. Safer medicines management across the interface is a core programme work stream to encourage development and implementation of reliable safe systems for reconciling medicines in GP practices following discharge from hospital. A robust standardised approach to MR in GP practice on discharge should improve the GP prescribing record and therefore the Emergency Care Summary (ECS) that is extracted from GP systems and used as the basis for MR on admission to hospital. Local data identified that this was only correct around 50% of the time. There was a national care bundle in development for MR which had been piloted in another Health Board but not been adopted or tested in NHS GGC GP practices. Practices acknowledged that MR is an important area of patient safety but none could demonstrate they had a standard process in place. To determine if there was a problem five practices agreed to participate in a pilot project to test and measure the MR care bundle.1 Run chart data and practice visits identified that their processes were not as robust as they had anticipated and they were not standardised across the whole practice team. The main aim of the project was to develop, test and implement at scale an MR care bundle focussing on process reliability which was defined as 95% compliance with the MR care bundle in general practice across participating NHS GGC GP practices by March 2016. Secondary aims to indicate improved outcomes were defined as an improvement in the accuracy of ECS on admission and a reduction in readmissions within 30 days for patients aged over 65.
Background
Taking a medicine is the most common intervention patients use to improve their health. Older people and those with long term conditions often take multiple medicines (polypharmacy) to treat and manage their illnesses. Evidence shows that there is a greater risk of error and potential harm from medicines when patients move between care settings, resulting in 30-70% of patients having an error or unintentional change in their medication when their care is transferred.2 Incidents of avoidable harm to patients can result in unnecessary readmissions, with an estimated 72% of adverse events after discharge due to medications3 and 38% of readmissions considered to be medicines related (61% of these preventable).4 Apart from the clear patient safety risks there are also implications for professionals with 19.3% of GP negligence claims relating to prescribing and medication (3.8% of which were due to supplying incorrect or inappropriate medication).5
Medicines reconciliation is an essential component of patient safety promoting safer use of medicines with effective communication when patients move between care settings and is particularly important when patients are admitted and discharged from hospital. There is evidence that this process does not happen reliably6 ,7 with local audits conducted in NHSGG&C reporting just over half of patients admitted in one hospital had one or more of their usual medicines unintentionally omitted from their prescription chart.8 60% of patients had medication discrepancies on discharge, specifically relating to medicines that had been started and/or stopped during the admission.9 ,10
A robust reliable process for carrying out timely medicines reconciliation in general practice post hospital discharge ensures the GP prescribing record is current and accurate. This in turn improves the accuracy of the Emergency Care Summary (ECS). The ECS is a summary of basic important information about a patient including a list of current medication which is extracted from the GP systems twice a day. The ECS is often used as a source of information used to carry out medicines reconciliation on admission to hospital. Inaccurate or incomplete medicines reconciliation in primary care will result in an inaccurate GP prescribing record and therefore a flawed ECS for any medicines reconciliation on admission with the potential for medication errors, patient harm and readmission.
The project began in 2011 at which point there was only a small amount of pilot work being carried out to test an MR care bundle in primary care. The aim of improvement work was to test a recognised SPSP care bundle at small scale for consideration of implementation and spread across a large organisation. Following testing, large scale implementation and spread was carried out in 2013, with 242 GP practices in NHS GGC participating. This is the largest scale MR programme in GP practice and was the first of it's kind in Scotland in terms of measurement and spread.
Baseline measurement
At the outset of the project it was not possible to determine how well MR was done as this data was not routinely collected as part of routine general practice. Practices anecdotally felt they had good processes in place but had no robust measurement strategy to support this. The SPSP PC MR care bundle sought to address this.
Five practices initially applied the care bundle to all their discharges and randomly sampled ten patients per month for compliance with the care bundle over 12 months - this provided baseline results. Sampling was done by identifying all patients who had been discharged that month and randomly selecting 10. From this the pilot practices could see month on month their results and it was aggregated up to give a collated overall picture for all 5 practices. The 12 month baseline data and median value of 64% can be seen in supplementary file “MR compliance baseline data”.
Supplemental material
Individual practice visits were carried out to determine if they felt the process was beneficial, establish what they had learned and what improvements they had made using PDSA. Consensus was sought in whether it was worthwhile to scale up and spread.
Design
Run chart data and practice feedback (including PDSA cycles) demonstrated there was room for improvement and using the established SPSP PC national MR care bundle was an efficient way to measure MR process reliability. Practices reported it was an effective QI tool to improve MR in the practice and it would be appropriate to consider for NHS GGC roll out. A wider stakeholder consultation took place with SPSP programme leads, clinical directors, the local medical committee (LMC) and the pharmacy and prescribing support unit (PPSU) to explore and agree options for spread. The anticipated problems at this stage were around potential funding for the work and GP acceptability for this care bundle to improve MR processes. As the care bundle was a recognised national intervention tool and had tested positively in a small number of practices, the final care bundle design was not changed, and after multiple stakeholder agreement it was planned to offer this out as an optional opt-in to all NHS GGC practices in 2013 (n = 254) as an enhanced service for 2013/14. 252 practices opted in. The aim of the work was for process reliability - 95% compliance with the care bundle by March 2014. The outcome measures were less clear but ECS accuracy and readmissions within 30 days were suggested as potential measures.
GP feedback was also gathered to assess the impact (positive and negative) of the work and to consider whether to continue for 2014–2016.
A series of evening education sessions for GPs and practice managers were undertaken in March and April 2013 to introduce QI methodology (model for improvement), the care bundle and method of data collection. The other core team members who were instrumental in supporting this work included the lead pharmacist for prescribing and our local SPSP GP clinical lead, a data analyst and the clinical governance support unit, with executive sponsorship from senior management such as the medical director and clinical governance leads.
Strategy
The overall aim of the work was to test and implement a primary care MR care bundle on a small scale to assess it's suitability and feasibility for roll out across a large scale organisation. The aim was for 95% process reliability across all participating practices. Defined outcome measures were less clear but it was decided to carry out snapshot data collection in secondary care to see if the ECS had improved following a focus on MR in primary care. For the MR work each practice was required to measure themselves monthly and using PDSA cycles make improvements to their own practice processes to achieve bundle compliance. It was not possible to collate all PDSAs undertaken per practice as these varied depending on the specific areas they needed to make improvements. Examples of improvements often included innovative ways of communicating changes in medication to patients other than just phone calls, such as notes on the repeat prescription slip and using translation services or online language sites to translate letters where English was not the patient's first language. Other examples of improvements to improve care bundle compliance included developing standard operating procedures within the practice so the MR process was agreed and standardised across all practice team members. Other practical resources were also developed such as designing recording templates in EMIS and Vision to aid better recording and thus facilitate data capture. Following successful piloting and refining our data collection methods the strategy for spread was to offer this as an enhanced service to all NHS GGC GP practices. To support the roll out, training was provided with resources and a contractual framework developed to support practices. It was stressed that the data they collected was for them to identify areas for improvement and not for judgement or remuneration. Along with MR care bundle data, practices were also asked to submit an annual reflection sheet. The main purpose of this was to determine if practices felt the MR care bundle improved patient safety, improved their practice processes and what improvements they had made. It also provided an opportunity to feedback comments on the work. Although it was not possible to collate all PDSA cycles, the practice reflection forms (n=200) indicated 68% made changes and improvements to their MR process. 85% thought carrying out the medicines reconciliation care bundle in their GP practice improved patient safety and 80% thought carrying out the medicines reconciliation care bundle in their practice had improved their practice processes. From this positive feedback the key learning was the work had been well received and evaluated positively by GP practices thus the enhanced service was continued for a further 2 years.
Results
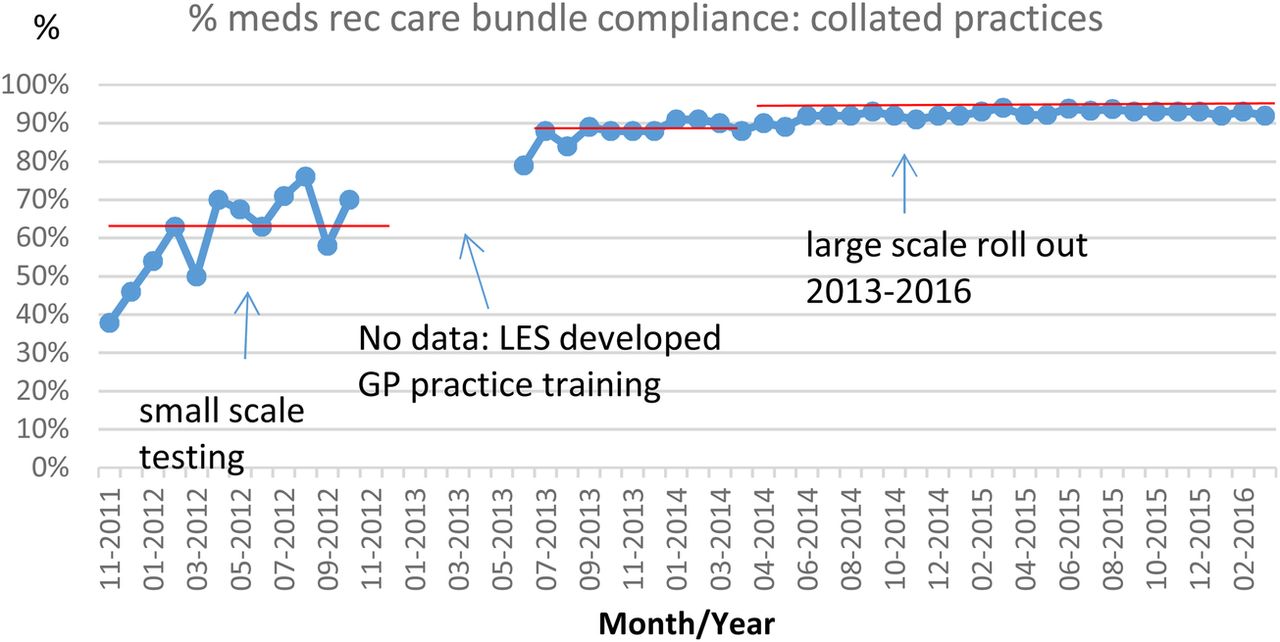
The compliance with the care bundle improved over time as demonstrated in Figure 1. From small scale testing a baseline median of 64% was observed. Following GP practice training and NHS GGC roll out, compliance increased from a median of 88% in 2013, to 92% for 2014/15 and 93% for 2015/16. An observed median of 92% was observed for 2014-2016. This demonstrated a reliable process but was short of the 95% aim.
{kind=link}
Practices measured care bundle compliance by applying the care bundle measures to a random sample of 10 patient discharges per month (in 2011/12 and 2014/15) and 5 patients per month in 2013/14 and 2015/16. Practices with large numbers of discharges a month were asked to prioritise patients over 65 years old. The variation in sample size was due to changes in the enhanced services contractual agreement over time. Practices completed an MR care bundle spreadsheet on a monthly basis which provided them with their individual data to identify areas for improvement and was also submitted centrally on a monthly basis to allow for an overall GGC collation. It is acknowledged that there may be bias in the sampling of patients, which may have been non-random to preferentially select those known to have had the process applied.
200 practices submitted reflection sheets on the MR process and care bundle - of these 85% reported the meds rec work had improved patient safety, 80% said it had improved practice processes and 68% said they had made specific improvements as a result of the work. One practice reported that undertaking the work had undoubtedly prevented a hospital readmission and early contact had made a real difference to the patient. This outcome was recorded as a patient story and can be viewed on YouTube.11 Most practices said they wished to continue the work in 2014 and 2015. The most reported negative aspect (identified as a balancing measure) was the additional time taken to undertake the process, although this was not quantified. However, many GPs reported the additional time invested offset time spent on correcting issues with discharge medicines later on. The suggested outcome measures of improved ECS accuracy was tested on a small scale in 1 hospital – this demonstrated an improved ECS accuracy from 50% to 60% however it is not possible to attribute this specifically to the medicines reconciliation care bundle work. Work is ongoing to identify any potential impact on readmission rates within 30 days.
Lessons and limitations
The main lessons learned when considering large scale roll out of MR work were to involve front line staff early in the testing and feedback on the intervention before implementation. This was invaluable when others challenged the validity of the intervention and how practical it was to use in practice. Involve key stakeholders and secure executive sponsorship early in the process to support wide spread implementation. From a practical perspective an easy way to collate the data at scale should be considered early in the process as this quickly became a large data burden when implemented over >200 practices. Robust data collection methods must be considered. Limitations within the work are mostly around limited outcome measures. Although this was always planned as a QI intervention to embed process reliability, greater consideration could have been given to measuring outcome data such as real time readmission rate within 30 days on a monthly basis rather than retrospectively. As there is no control group (as 97% of practices participated) it may not be possible now to demonstrate the proposed outcome measure. Other potential limitations may be non random sampling by practices of patients they know had had the process applied which introduces bias. In terms of QI methodology, the sample size of 10 for each individual practice may be too small to properly determine process reliability however was a compromise between workload and actual number of discharges received per month, but sufficient to signal improvement.
Practices have embedded MR processes now and the anticipation is they will continue to do this even though formal data collection has ended. Anecdotally practices report they are still doing this and although no longer an enhanced service, 10% of practices continue to submit data.
It has not been possible to determine if the intervention was cost effective as no return on investment analysis was undertaken. There are a number of perceived benefits from MR such as reduced medicines wastage and a reduction in readmission rates – these could be converted into a financial saving but as yet this analysis has not been concluded.
Conclusion
To summarise the work it was observed that the compliance with the MR care bundle improved over time. Small scale testing demonstrated MR processes were not reliable against the bundle with a baseline median of 64% observed. Following successful testing, large scale roll out across the organisation was designed and implemented across >200 GP practices where compliance increased from a median of 88% in 2013, to 92% for 2014/15 and 93% for 2015/16. This demonstrated a reliable process but was short of the original aim of 95% compliance with the MR care bundle by March 2016.
There has been extensive literature on MR within secondary care however there is less in the primary care setting. The implementation and results of an MR care bundle in primary care at such large scale has not previously been reported and this work demonstrates the results achieved at scale. Work is ongoing to determine if the intervention has reduced the rate of readmissions within 30 days of discharge for patients aged over 65. The reflections from GP practices on the benefits of the work were overwhelmingly positive and to quote one of the comments received: “There has been a significant increase in patient safety by reducing prescribing errors by doctors undertaking the meds rec. I feel this has been one of the most valuable enhanced services that we have ever been involved in.” Margaret's story which demonstrated preventing a readmission was also a very positive aspect of the work from a patient's perspective.
Although balancing measures were not routinely measured the main feedback was on the additional time taken to undertake the MR care bundle. This was not always viewed as being a negative - as another quote stated “it is more time-consuming however it is time well spent as it prevents any issues or queries further down the line which take longer to resolve”. There was also lots of comments on the time taken to contact patients however this was also reported as positive feedback on how patients had appreciated a phone call and it had improved practice/GP/patient relationships.
The results have demonstrated that the primary care MR bundle is generalizable and applicable to all GP practices in NHS GGC and although the target of 95% reliability was not achieved a sustained median of 93% was observed for the last year. This MR care bundle could be applied to any GP practice setting to promote standardisation of a robust MR process.
The next steps in this work are to design and test a joint primary and secondary care medicines reconciliation care bundle and to feedback and share learning from this with secondary care.
Acknowledgments
NHS GGC GP practices, Dr Paul Ryan, Richard Hassett, Margaret Ryan, Alasdair Buchanan, Dr Alister McLaren, Heather Thompson, Spencer Green, Clinical Governance Support Unit - all NHS GGC; Dr Andrew Martin NHS Tayside; Jill Gillies, Neil Houston (Healthcare Improvement Scotland)
Footnotes
Declaration of interests None
Ethical approval We used the following criteria for determining if improvement activities require ethics review. Policy criterion: The work is primarily intended to improve patient care and practice processes, not provide generalisable knowledge in a field of inquiry. Explanation: The work reported here meets this criterion because medicines reconciliation is a universally recommended process. We sought only to evaluate the improvements in compliance with a medicines reconciliation care bundle as a result of monthly data collection and feedback of compliance rates to relevant parties internal and external to NHS GGC.