Article Text

Abstract
Handoffs represent a critical transition point in patient care that play a key role in patient safety. Our quality improvement project was a descriptive observational study aimed at standardizing pediatric hospitalist handoffs via implementation of a handoff checklist, with the goal of improving handoff quality and physician satisfaction within six months. The handoff checklist was quickly adapted by hospitalists, with median compliance rate of 83% during the study. Handoff quality was assessed by trained observers using the validated Handoff Clinical Evaluation Exercise (CEX) tool at multiple time periods pre- and post-implementation (at 2, 6, 12, and 24 months). Handoff quality improved during our study, with a significant decrease in the percentage of "unsatisfactory" handoffs from 9% to 0% (p-value 0.004), an effect which was sustained after initial project completion. The cumulative time required for verbal handoffs for different attending physicians paralleled patient census. However, our project identified wasted down time between individual physician handoffs, and an intervention to change shift times led to a decrease in the average total handoff process time from 86 minutes to 60 minutes, p-value <0.001. An average of 7.4 patient care items was identified during handoffs. A physician perception survey revealed improved situational awareness, efficiency, patient safety, and physician satisfaction as a result of our handoff improvement project. In conclusion, implementation of a checklist and standardized handoff process for pediatric hospitalists improved handoff efficiency and quality, as well as physician satisfaction.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Prior to June 2010, pediatric hospitalists (inpatient physicians specializing in the care of hospitalized children) at Texas Children's Hospital (TCH) had no standardized handoff process for signing out patients to each other during their transitions between day shifts and night shifts. The goal of this Quality Improvement (QI) initiative was to create a standardized pediatric hospitalist attending handoff process that addressed patient care items, maintained workflow efficiency, and improved physician perceptions by utilizing a patient handoff checklist.
This study took place in a quaternary, freestanding children's hospital in Houston, Texas, United States. The pediatric hospitalist service has an average daily patient census (total number of patients) of 30-50 patients and admits to a closed 16 bed inpatient unit, as well as other acute care units (217 beds) and the Level 2 Nursery unit (55 beds). The daily patient census is divided into four to five teams composed of medical students, residents, and fellows, and led by attending physicians.
At the onset of this study, shift change times were at 6 AM, 3 PM, and 11 PM. Weekday staffing included one on-call attending holding the admissions pager, who signed out at 3 PM to the evening shift (3 PM-11 PM) attending, as well as three to four other attendings who signed out at 4 PM. The evening shift handoffs at 3 and 4 PM were chosen for this study because they represented the greatest number of patients per handoff in our transitions of providing care.
The two primary aims of our project were: (1) within six months of implementing a handoff checklist, all pediatric hospitalist evening shift handoffs would be completed within one hour using a standardized format, and (2) that 100% of observed handoffs would be rated as “Superior” (> or = 7) on the Handoff Clinical Evaluation Exercise (CEX) tool. A secondary aim was to improve physician perceptions of patient care delivery. Metrics to address these aims included process, outcome, and balance measures.
Background
Handoffs are a critical transition point in patient care, with communication consistently cited as a root cause in most sentinel events.(1) In 2006, the Joint Commission advocated implementing a standardized handoff approach in clinical settings as a National Patient Safety Goal.(2) In 2009, the Society of Hospital Medicine Task Force recommended instituting formal handoff systems at shift and service changes.(3)
Despite these recommendations, few studies have looked at the handoff process for inpatient attending physicians.(4-7) Most current literature focuses on handoffs in the resident/medical student sphere.(7-10) Additionally, checklists are being utilized for handoffs in areas such as the emergency room, but none has been previously described for hospitalist attending handoffs.(11)
Baseline measurement
Handoff quality was quantified using the 9 point CEX tool, the only validated handoff measurement tool to date.(5,6) Observations were performed by a dedicated handoff team of six members (5 hospitalists and 1 clinical nurse) who received prior training on use of the CEX tool. One evaluation was completed for each individual daytime attending involved in the evening shift handoff. Whenever possible, two observers independently rated handoffs. The number of observations was limited to a convenience sample based on the size of our hospitalist group, with approximately 100 physician handoffs observed during each of the study periods: pre-implementation (period 0), and at 2, 6, 12, and 24 months post-implementation.
For our baseline handoff quality measurements, we initially calculated the mean and median of all CEX tool observation scores. However, we quickly discovered the majority of our handoffs were scored as Superior (> or = 7), with mean and median scores of 8. We surmised that this was likely because the CEX tool was designed to measure medical student handoff quality. We felt that all attending physicians should be able to provide Superior handoffs, and thus, we decided to measure the percentage of handoffs which scored <7, representing an unsatisfactory handoff. During our pre-intervention period (period 0), this percentage was 9% of all observed handoffs.
Additional outcome, process, and balance metrics are listed in Supplementary Table 1.
Supplementary table
Design
In June 2010, pediatric hospitalists created a written electronic SBAR (Situation, Background, Assessment, Recommendation) sign-out template. Although the written sign-out template was gradually standardized within the group, the verbal handoff process remained chaotic. Handoffs were loud and held in a disruptive environment, varied in timing and details among physicians, and were not consistently given face-to-face with verbal communication.
A pediatric hospitalist handoff team was formed to improve verbal handoffs. Focus groups and surveys were held with pediatric hospitalists, and stakeholder buy-in was obtained via support from hospitalist section leaders. A QI mentor physician outside of the hospitalist section was recruited to guide development of the initiative. Several systems issues delayed the process, including a high winter census, implementation of a new electronic medical record system, and opening of a satellite hospital staffed by pediatric hospitalists, but by May 2011, a formal initiative with specific goals and metrics was in place.
Ultimately, a standardized handoff checklist was created for evening shift attendings and implemented on 23 August 2011. Checklist items included hospitalist daily census, sick patients, and patients needing follow-up or anticipatory guidance for the evening and night shifts.
Education about the importance of handoffs and checklist usage was provided during multiple section meetings between May and August 2011, with continued reminders after implementation. Hospitalists were updated regularly on checklist compliance during staff meetings. Hospitalist section leaders supported the project by mandating face-to-face handoffs at a designated time and place. The checklist was iteratively modified five times based on attending feedback and was eventually condensed to one page.
Strategy
Baseline measurement (19 July to 22 August 2011): Handoff observations performed prior to implementation of the checklist confirmed focus group opinions that handoffs were frequently chaotic and disorganized, with 15% and 11% of Setting and Organization scoring <7 on the CEX tool.
Improvement Cycle 1 (23 August 2011 to 31 January 2012): The handoff checklist (see Supplementary Figure 1) was introduced as both a tool intended for the receiving physician to utilize during their evening shift, as well as a means of collecting data about handoff times and important patient care items. Weekly reminders regarding checklist usage were made at hospitalist staff meetings, and checklist usage quickly reached 80%. During this time, several PDSA cycles were performed with different variations of the checklist, which was ultimately modified five times to enhance utility and user-friendliness based on hospitalist feedback. Handoff observations performed at 2 months post-implementation (24 October to 30 November 2011) revealed a decrease in the percentage of unsatisfactory handoffs to 4.9%.
Supplementary figure
Improvement Cycle 2 (1 February to 29 October 2012): While we were pleased with the reduction in number of unsatisfactory handoffs after implementation of our process, during our data analysis we noted that there was significant wasted time between different attending handoffs. The cumulative time that the attendings were actually giving verbal handoffs (verbal handoff time) was averaging 28 minutes, but the entire handoff process from the start of the first daytime attending handoff to the end of the last one, including any down time in between (total handoff process time) was averaging 86 minutes. This meant that the attending receiving handoffs was waiting in the office for nearly 60 additional minutes to complete the handoff process. At the time, one daytime attending carrying the admissions pager handed off at 3 PM, while the other daytime attendings handed off at 4 PM. We sought to reduce the down time between handoffs by changing the evening shift start time to 3:30 PM, with the goal of completing all daytime attending handoffs by 4:30 PM. This change in shift times was implemented on 1 February 2012, and subsequently we noticed a decrease in the total handoff process time to 60 minutes, while the average verbal handoff time remained stable at 26 minutes.
During this improvement cycle, two additional sets of handoff observations were performed at 6 months (23 February to 30 March 2012) and 12 months (24 August to 28 September 2012). Overall handoff quality continued to improve compared to baseline, with 1% and 3.8% of handoffs scored as less than satisfactory at 6 and 12 months respectively.
Improvement Cycle 3 (30 October 2012 to 30 September 2013): In-person verbal handoffs and handoff times/locations had become widely accepted and standard practice among our hospitalist group. With the handoff process firmly in place, we opted to move the checklist from paper format to an electronic version within the electronic medical record (EMR). We were already typing written sign-outs in SBAR format in the EMR, and the creation of an electronic handoff list streamlined the handoff process. Hospitalists who still desired a physical checklist were able to print the electronic handoff patient list for their personal use. Education was provided to demonstrate how to use the new EMR-based handoff checklist during our hospitalist staff meetings and via email. Since hospitalists were already familiar with typing electronic sign-outs, the transition from paper to electronic handoff lists occurred smoothly. However, we did lose the ability to track handoff times, since there was no physical location for attendings to document these times.
Our last set of handoff observations occurred at 24 months from 19 August to 30 September 2013. We were pleased to note excellent handoff quality scores (Table 1), with no handoffs scored as unsatisfactory.
Measurement of handoff quality via observations using the Handoff CEX tool. The reduction in percentage of unsatisfactory scores <7 between months was statistically significant (p<0.05) when calculated using Pearson Chi-square p-value. *Although overall p-value for Professionalism was not statistically significant, post-hoc analysis showed comparing 0 months to 24 months showed a significant difference p=0.04.
Results
Outcome metrics for our project included handoff quality, number of patient care items identified, and physician satisfaction with the handoff process.
Handoff quality was assessed at 0 months (pre-implementation) and 2, 6, 12, and 24 months post-implementation. The percentage of unsatisfactory handoffs scoring <7 showed a statistically significant decrease with each observation period, p-value <0.05 (Table 1).
“Patient care items” included any identified patients who were sicker, required follow-up, or had anticipatory guidance provided by the day team. An average of 7.4 patient care items was identified per day.
A 27-question physician perception survey was created to assess hospitalist satisfaction with the new handoff process and whether it improved situational awareness and aligned with the six Institute of Medicine (IOM) domains. Survey face validity was achieved via review of survey questions by handoff team members and two focus groups of hospitalists who were ineligible for the survey. The final survey version was distributed electronically to pediatric hospitalists who were part of the section before and after implementation of the new handoff process. Nineteen of 21 eligible pediatric hospitalists completed the survey. Nine out of the 11 before- and after- question pairings were found to be statistically significant based on the Signed Rank Test, with p-values <0.05 (see Supplementary Table 2). Survey respondents uniformly “agreed/strongly agreed” that use of the electronic SBAR sign-out and standardized verbal handoff process led to improved organization, more consistency, and reduced time to handoff patients.
Supplementary table
Process measures included compliance with the handoff checklist and “verbal handoff time,” defined as the cumulative time used by the four to five daytime attendings to complete their verbal handoffs. Compliance with the handoff checklist was defined as >80% completion of daily checklist items, and a median rate of 80% was quickly achieved during our first improvement cycle and maintained throughout our study. The average “verbal handoff time” ranged from 19 to 39 minutes during our study, and paralleled daily patient census, which was felt to be logical and appropriate.
The balance measure – “total handoff process time” – represented the time required for the entire evening shift handoff process to be completed, including any down time between different attending handoffs. While we wanted handoffs to be thorough and provide all necessary information, we did not want the process to become so time-intensive that it disrupted patient care during our busy evening shifts. After our intervention in improvement cycle 2 (changing the evening shift time to better consolidate the daytime attending handoffs), the mean total handoff process time significantly decreased from an average of 86 minutes to 60 minutes, p-value<0.001). Additionally, the change in shift time met statistical process control chart rules for a special cause, as evidenced by six points below the median (Figure 1).

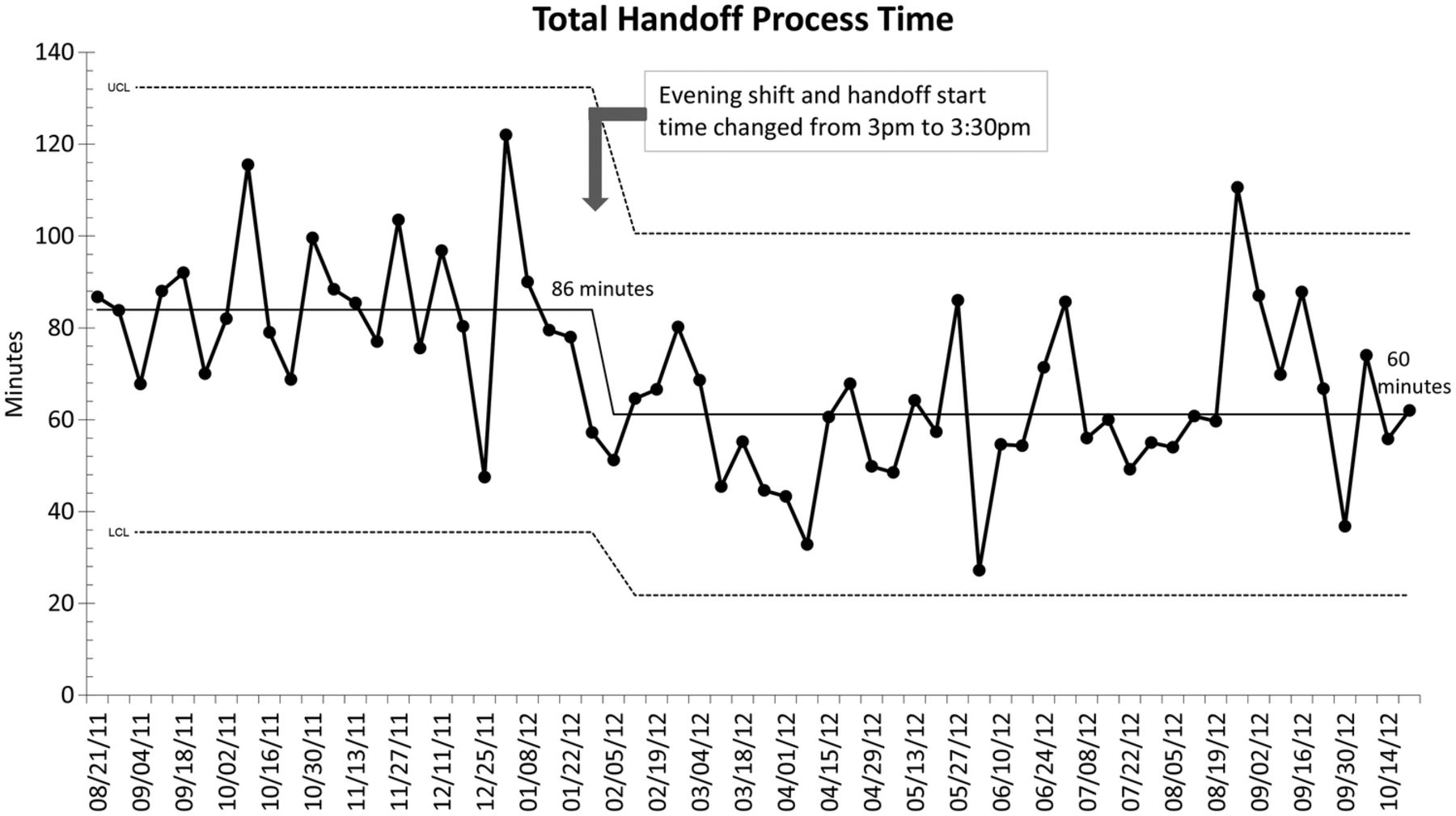{kind=link}
Total handoff process time calculated from beginning of first handoff to the end of last handoff, averaged monthly. Total handoff process time represented actual verbal handoff time plus any down time between attending handoffs. Total handoff process time statistically significantly decreased from median 84 minutes to 61 minutes after a change in evening shift times, as calculated by t-test (t(192.61) = 7.22, p-value <0.001).
Lessons and limitations
Key elements for successful, sustainable development and implementation of this handoff checklist included early buy-in and involvement from key stakeholders, feedback-based modification of the checklist, and incorporation of the checklist into an electronic format that is user-friendly. One of our main challenges was the time commitment required to perform observations at multiple time points during the study, but this metric was felt to be a critical one with regards to assessing handoff quality, and one that we felt was ultimately a strength of our study.
The main limitation of this study is the lack of robust patient outcome and safety data. Although our project aims were met and outcome measures suggested improvement, these measures served as surrogate markers for patient level outcomes. We did attempt to collect physician perceptions of error/failure on the handoff checklist (question: “Were there any surprises or unexpected events?”); however, due to the necessity of this survey section being completed at end of shift, it was often incomplete and therefore data were inadequate for inclusion in the study. Additional observations or resources for extensive chart review would be necessary to assess for these errors.
Other limitations include a single center design, use of a non-validated survey to measure physician perceptions, and dependence on individual providers to document on a paper checklist leading to incomplete data at times. Performance of the handoff observations themselves may have changed hospitalist behavior via the Hawthorne effect. Although the handoff team performing observations received training before the study and a standardized handoff tool was used, there is a possibility of observer bias. Furthermore, while we attempted to have two independent observers whenever possible, this only occurred about 20% of the time due to the time commitment required for performing observations and the handoff team's own clinical responsibilities. We considered two ratings within 2 points of each other on the 9 point CEX scale to be in agreement. Using this criteria, we had a 98% inter-rater agreement in handoff observation scoring. Finally, although the survey showed significant changes in perception, it is possible other simultaneous processes beyond the change in handoffs may have influenced responses.
Conclusion
Although we did not reach our goal of 100% compliance with handoff checklist and process, we were able to quickly achieve >80% compliance and maintain this level throughout our study. The creation of a standardized pediatric hospitalist handoff process utilizing a new electronic SBAR format and checklist constituted a significant achievement in a short time frame, especially in light of the previous absence of any formalized handoff process.
Our second aim of completing all evening handoffs within 1 hour was achieved. Actual verbal handoff time was consistently less than 60 minutes. Additionally, we were able to significantly reduce the total handoff process time from a mean of 86 to 60 minutes by changing the evening shift time and thereby minimizing down time between individual handoffs. Since this represented a decrease in “wasted” time, we felt this achievement to be a particular successful aspect of our project, and this change in shift time continues to this day.
A third aim of our study was to ensure high quality handoffs were being performed to facilitate high quality patient care. We observed a statistically significant reduction in the percentage of unsatisfactory handoffs when comparing pre-implementation to each of the subsequent post-intervention time periods. Most importantly, this change was sustained at the 24 month period, which had the smallest percentage of unsatisfactory handoffs noted during the study. Although the Handoff CEX tool is somewhat subjective in that it is dependent on observer ratings, we attempted to maximize the robustness of this metric by using a previously validated handoff evaluation tool and using only a small trained group of handoff observers. Moreover, an objective measurement of identified patient care items revealed an average of 7.4 items discussed per day during handoffs. Since these patient care items included sick patients and anticipatory guidance for potential patient events, the feedback we received from attendings indicated that knowledge of these items was critical in enhancing their situational awareness and ability to provide high quality patient care.
Our final aim of improving physician perceptions of handoffs was also achieved - specifically in 5 of the 6 IOM domains of quality patient care. The new handoff process was not felt to significantly improve the IOM domain equity of care or in preventing clinical issues or adverse events. This could be explained by the fact that multiple factors can lead to unexpected events and the delivery of equitable care, making it difficult to isolate the impact of handoffs in these areas. Physician satisfaction significantly improved. Importantly, survey respondents felt that the new handoff process improved communication between providers and helped to better identify sick patients. Additionally, physicians agreed that use of the electronic SBAR sign-out aided in improving and standardizing the handoff process, and also allowed attendings to actively listen and synthesize the information handed off without having to worry about writing patient information down.
Ultimately, the electronic handoff checklist and face-to-face handoff process has remained in place as of summer 2016, and it is now an accepted standard of practice within our group. Our study successfully achieved multiple aims including development of a standardized handoff process that is high quality, completed within 1 hour, and improved physician perceptions. Cognitive aids such as an electronic sign-out and a standardized checklist were effective tools in creating a successful, sustainable process that improved outcomes in hospitalist attending handoffs. Potential future directions would be to expand this process to other services in our institution and to hospitalist groups at other institutions.
Acknowledgments
The authors acknowledge Elena Wahmhoff, MD and Ruchi Gupta, MD for their work on the handoff observation team. The authors also acknowledge Elizabeth A. Camp, PhD for help with statistical analyses.
Footnotes
Declaration of interests All authors declare that there are no conflicts of interest.
Ethical approval This QI study was approved by the local institutional review board. All physicians in the Section of Pediatric Hospital Medicine voluntarily consented to handoff observations, and were assigned unique identifiers to preserve their privacy and confidentiality.