Article Text

Abstract
Venous thromboembolism (VTE) is one of the leading causes of maternal mortality in the UK. Therefore, timely VTE risk assessment is essential in all obstetrics patients. The Commissioning for Quality and Innovation (CQUIN) payment framework set a target for trusts to complete a VTE risk assessment within 24 hours of admission for 95% of patients. A combination of factors, including lack of integration between multiple IT systems, means that this CQUIN target is currently not being met for obstetric patients in the Hospital Birth Centre at Guys and St Thomas' NHS Trust.
This project aims to increase staff awareness of this issue and educate them regarding the correct procedure for VTE assessment. Trialled methods included reminders at staff handovers, use of magnets on the patient whiteboard, posters and stickers displayed around the unit and a loyalty card scheme as incentive to complete assessments. Initial average completion rate was 20.7%, which increased to 67.5% after the first plan, do, study, act (PDSA) cycle with a slight drop to 65.7% after the second cycle. Completion rates increased to 92.3% on the last day of the third PDSA cycle. Although we did not reach the 95% target, we have raised awareness of the importance of recording VTE assessment on electronic systems, and hope we have created sustainable change.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
This quality improvement project was undertaken at St Thomas' Hospital Birth Centre (HBC) by four fourth year medical students, under the supervision of an obstetric consultant and two junior doctors. St Thomas' is a tertiary teaching hospital in London, UK and is the base for maternity services for the Guy's and St Thomas' (GSTT) NHS Foundation Trust. With 22 beds on HBC, an average of 40 patients are admitted each day. The department has 90 staff members in total with 15 present on each shift. St Thomas' HBC patient population encompasses South-East London and annually sees approximately 6000 births.
As part of GSTT protocol, venous thromboembolism (VTE) risk assessment of women on HBC is completed on two separate computer systems. One is BadgerNet, Clevermed version 2.9.1.0, a maternity electronic record where antenatal, postnatal, and delivery details are recorded. The second system is the electronic patient record (EPR), iSOFT version 1.6. The CQUIN target is for 95% of patients to have a VTE assessment completed within 24 hours of admission. Previously women who delivered during their admission had their VTE assessment completed on BadgerNet, while those who were admitted but did not deliver were assessed on EPR. To simplify this issue, it was decided that all obstetrics patients must have their VTE risk assessed on EPR within 24 hours of admission, regardless if they had delivered or not. The significance of EPR is that it is used across all departments and is the system the trust uses to oversee VTE assessment rates. EPR is easy to monitor and extract data from and each month every department is informed of their VTE assessment completion rates Unfortunately, although monthly reports show a 98% completion rate of VTE assessments on BadgerNet, EPR VTE assessment levels are consistently low across the maternity department, and need to be improved.
Correct assessment is imperative, especially considering the implications of inadequately prescribing VTE prophylaxis. St Thomas' had two VTE cases postnatally between April 2015 and April 2016 which are currently under root cause analysis (RCA) investigation. One of the main factors contributing to the lack of assessment on EPR is the duplication across IT systems. Moreover, many staff members were unaware of the need to now complete VTE assessment on both EPR and BadgerNet.
The aim of this project was to achieve at least a 95% completion rate of VTE assessment on EPR in the HBC, including the obstetric high dependency unit (HDU), at St Thomas' by May 2016.
Background
VTE remains the leading cause of direct maternal death in the UK.1 The risk of VTE increases as pregnancy progresses (four to six fold higher than that of a non-pregnant woman), and is further increased in the postpartum period.2
However, it is important to note that some women will be at higher risk than others.2 Therefore, a form of risk stratification is imperative in ensuring women are adequately provided with appropriate prophylaxis.3 In addition to this, the threshold for prophylaxis postpartum is lower than antepartum as the risk is higher per day.4
There are known risk factors that increase the likelihood of acquiring a VTE in pregnancy and puerperium, including high body mass index (> 30), increased maternal age at delivery, prolonged labour, caesarean section, and immobility.5 ,6 VTE prophylaxis will depend on the risk stratification and most commonly includes low molecular weight heparin (LMWH).5
Prevention of VTE is a key issue in patient safety and so this area has been the subject of much research. Some authors have suggested that the best ways to encourage staff to document VTE scores are via education regarding the importance of the assessment, reminders in paper and electronic form, as well as streamlining VTE assessments into current workload.7 ,8 Furthermore, it has also been shown that simply introducing new prophylaxis guidelines without prior education of staff members does not necessarily improve levels of VTE assessment.9
Baseline measurement
In order to measure the scale of our problem, we checked whether patients on the HBC had had their VTE risk assessment recorded on EPR. All patients on the unit were checked for three consecutive days, with data collected at 5:00pm. There is minimal patient overlap day to day due to the high turnover of patients on HBC. The outcome measure was calculated as the percentage of patients whose VTE risk was assessed at that particular time.The results showed that over the first three days, a mean of only 20.7% of patients had had their assessment completed on EPR.
Design
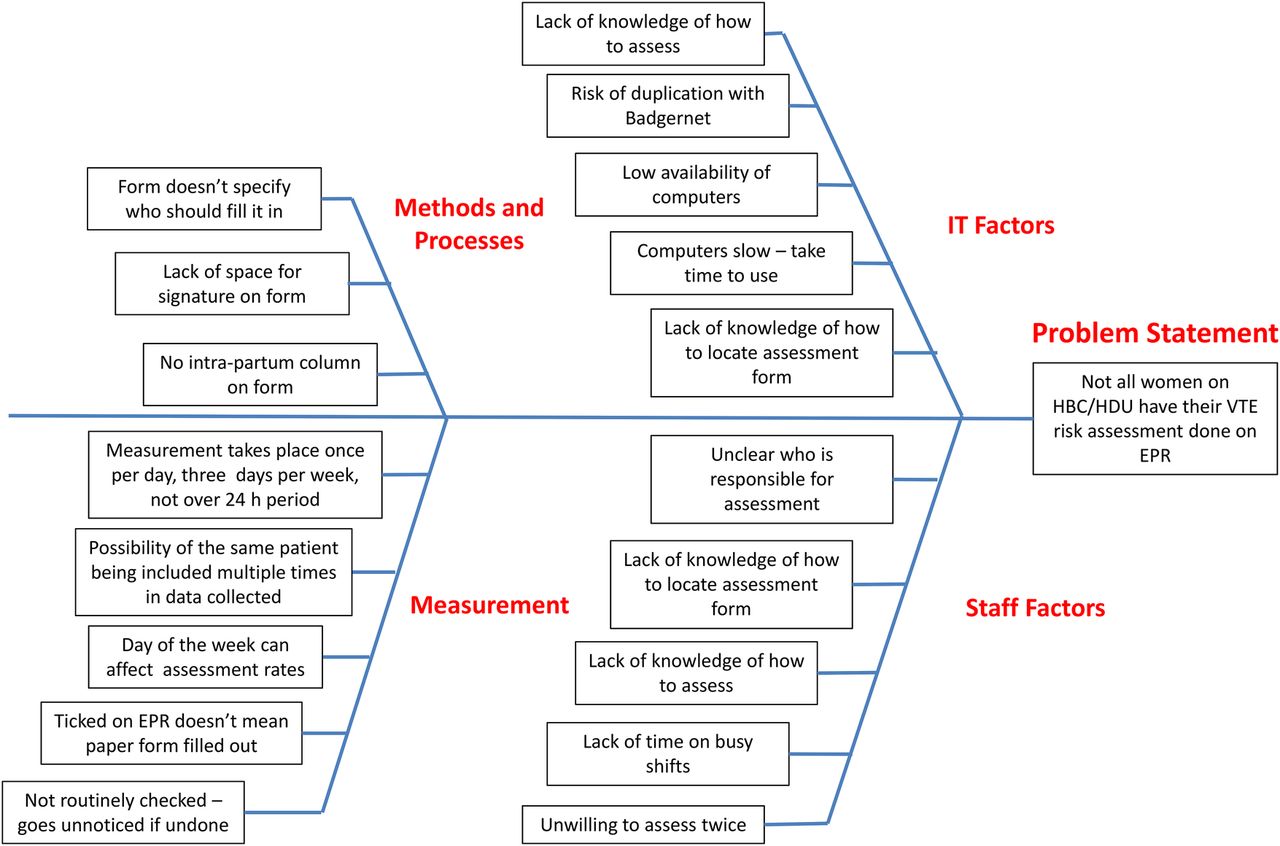
When considering how to combat this problem, we recognised that the reasons for VTE assessments not being completed on EPR were multifactorial. These included lack of awareness of how and when to fill out the assessment, time constraints during a busy shift, and IT factors such poor availability of computers on the ward and duplication with BadgerNet. Factors contributing to the problem are summarised in our fishbone diagram (figure 1).

A fishbone diagram summarising the reasons why not all patients on the HBC had their risk assessment completed on EPR
As there was little we could do about the number of ward computers and lack of time to complete the assessment, we decided to focus our project on promoting awareness of the correct procedure. At the start of our project, many of the midwives and junior doctors on the ward were unaware that trust policy dictates that the assessment must be completed on EPR as well as BadgerNet.
With this in mind, we decided that our first two interventions should focus on educating staff on the correct procedure for documenting VTE assessment, and also reminding them of the need to do it, by making alterations to the patient whiteboard and using stickers and posters throughout the department.
We anticipated that asking busy staff members to complete the assessment twice on two separate IT systems might cause problems, and so our third intervention introduced a “loyalty card” scheme of a £2 coffee voucher given after the completion of six VTE assessments.
Each of our cycles was two weeks long. Our project was interrupted by one week between cycles two and three due to the junior doctors' strike.
Although we recognise that our loyalty card scheme is not feasible to continue long term, we hope that by educating staff on the correct procedure and raising awareness of the need to complete the assessment on EPR, we will implement long term change.
Strategy
PDSA cycle 1 (28th March - 8th April 2016): The aim of this cycle was to raise awareness of the correct documentation procedure among staff as we felt that this was a major contributor to the low levels of VTE assessment on EPR.
We hypothesised that making an alteration to the HBC patient whiteboard would provide a clear visual reminder and increase VTE assessment documentation rates.
Therefore, as our first intervention, we altered the patient whiteboard to include a column for VTE assessment. Already on the whiteboard are patient details, their bed number, the clinical situation, and other relevant information. The whiteboard is referred to at midwife and doctor handover and is continually updated throughout the day. In our new column, we used coloured magnets to indicate whether or not the patient had had their VTE assessment documented on EPR (green and red dots respectively). We then attended both the midwives' and doctors' handovers and explained the VTE assessment procedure, the need for completion on EPR, and the use of the coloured dots as a reminder.
Data collection over a three day period at the end of this cycle showed this cycle showed a VTE assessment completion rate of 67.5% – a large improvement from our our baseline. The success of this cycle illustrated that the lack of awareness of EPR VTE assessment was indeed a contributing factor to the initial low VTE recordings. However, we did not meet our target of 95%, so additional interventions were required.
PDSA cycle 2 (11th - 22nd April 2016): The aim of this cycle was to reinforce the need to complete VTE assessments by continuing to remind staff of the correct procedure without our presence at handover each day, as this was not sustainable in the long run.
Encouraged by the success of our first cycle, we hypothesised that placing further visual reminders around the department would build upon the improvements that we saw at the end of the first cycle. Our second intervention was to place stickers on all ward computers and display posters in common areas.
Data collection after this cycle showed a completion rate of 65.7% – a slight drop from the previous cycle. This indicated that these reminders were not as effective as direct communication on our part with the staff at handover each morning. We also felt that these results might indicate that simple reminders were not enough to implement more change than we had already seen in the first cycle. Therefore we decided to take a different approach with our third cycle.
PDSA cycle 3 (2nd-13th May 2016): The aim of this cycle was to build on previous improvements and attempt to reach our target of 95% completion by introducing an incentive to document VTE assessments correctly.
We hypothesised that a more direct incentive for the staff would see an increase in completion rates of- which we hoped would then become habitual.
Our third intervention was to create and distribute loyalty cards to all the midwives and junior doctors on the unit, which were stamped for each completed VTE assessment. Six stamps were required to fill the card. Staff could then exchange a completed card for a >2 coffee voucher. Distribution of the cards was another opportunity for us to explain the necessary procedures, and also allowed us to discuss the project with staff members and collect feedback regarding alterations to the assessment form.
Data collection after this cycle showed an average completion rate of 65.6%. However, data collection during the final week of our cycle showed an average of 79.5%, our highest throughout the project - a rise which we anticipated to take a while due to the gradual distribution of the loyalty cards to the entire staff bank.
Results
Data was collected on 18 separate occasions by checking EPR at 5:00pm. Here we printed the list of patients on HBC (including HDU). The outcome measure was calculated as the percentage of patients whose VTE risk was assessed at that particular time.
Average of the first three measurements, on three consecutive days in the week preceding the first intervention, established the pre-intervention baseline and showed that a mean of only 20.7% of patients had had their VTE assessment completed on EPR.
Data was collected on further 15 occasions: on three consecutive days (Wednesday, Thursday, and Friday) at the end of each of the three cycles, as well as mid-cycle 2 and 3. Data was collected in this manner in order to let each cycle take effect before looking for an improvement.
Results have shown improvement in VTE completion rates on EPR which was sustained throughout the project. Figure 2 shows the trend of the VTE assessment rate on EPR throughout the project - on introduction of the magnetic dot system on the HBC whiteboard there was a sharp increase from baseline measurement. However, this increase was difficult to maintain, demonstrated by the decline on the graph, even after our second cycle of sticker and poster reminders. Finally, our third intervention of the loyalty card system took a while to implement as shown by the plateau, but once more cards had been distributed to staff members in the maternity department there was again a sharp increase in the number of VTE assessments completed on EPR.
First cycle data shows a 46.8% improvement in average VTE completion rate from 20.7% to 67.5%. Despite variations in the data on individual days this rise in the average was sustained in the second (65.5%) and third cycle (65.6%). The final week of the third cycle finished with an average completion rate of 79.5% (with the rate being 92.3% on the last day) – the highest throughout the project (figure 2).

{kind=link}
{kind=link}
A run spreadsheet shows the results of our data collection. Dashed lines indicate days on which data was not collected
Lessons and limitations
We learnt a number of lessons from carrying out this project. Firstly, we found personal interactions with HBC staff to explain our interventions to be more effective than putting up posters and sticker reminders, emphasising the importance of good staff communication in quality improvement. By attending the handovers and promoting the loyalty card scheme we were able to emphasise the importance of confirming that VTE score had been assessed on EPR and demonstrate how to do so if individuals were unsure. Moreover, by talking to staff we were able to identify their issues with the interventions and address any concerns they had.
We felt that our loyalty card scheme worked well to highlight our campaign and generate interest, without taking away what was being achieved already - the assessment of patients. Introducing the EPR system to staff who were not familiar with it and interacting with the team as a whole is an established practise for any system change in the NHS.
Through discussion with staff we found the the largest barrier to be the lack of integration between the IT systems on the HBC. Staff now had to complete VTE assessment on EPR as well as BadgerNet, so it was difficult to implement a change when it required duplication of work. To reinforce this finding, data collection and quantification of the problems surrounding VTE assessment on EPR would have improved and strengthened our project. Maintaining the effect of an intervention was also a challenge, as seen by the drops in our run chart (see figure 2). Although we promoted the magnetic dot system on the board and the loyalty cards scheme for a week, the shear breadth of the HBC staff roster inevitably meant that not all healthcare professionals were informed of the interventions happening. Over time enthusiasm wanes and it is difficult to change routine.
Although the direct impact of our interventions, particularly our reward scheme, may lessen over time, overall the project greatly raised awareness regarding VTE assessment and the importance of its correct documentation for patient safety, and we hope that this in itself will lead to sustainable improvement. Our PDSA cycles involved lots of training interventions which were well received by staff, generating discussions and providing important continuous learning. Through discussions with staff we recognised the IT issues and empathised with their frustrations, feeding back suggestions such as including an ‘intra-partum’ column on the VTE assessment form and trying to integrate the BadgerNet and EPR systems for efficiency.
In terms of sustainability, the magnets remain on the HBC whiteboard and are still being used by the midwives in-charge. The stickers and posters we placed on the department also remain in place and the loyalty card scheme will continue until all cards have been used up. All staff will continue to have education and reminders on completing VTE assessment on EPR because it remains a vital area of improvement with the 95% target not yet achieved.
Furthermore, the hospital trust is looking at implementing a system where VTE assessment on EPR will be mandatory before any prophylaxis can be prescribed. In the meantime, the three doctors who supervised this project remain in the department and are able to both oversee the continuation of our changes and continue raising awareness of the importance of correctly completing assessments.
To further enhance sustainability, we are looking into nominating an individual/group of individuals (ie, the obstetric senior house officer or midwife in-charge) to oversee and promote the interventions on their shifts. We feel that this would be particularly effective with with regards to the magnetic dot system, because during this initiative there was some confusion over whose responsibility it was to update the board. Ideally, we would like to continue to collect data in the future in order to assess the sustainability of our interventions. Alternatively, this project could be continued by a new team of medical students when they rotate into the department next year, and further interventions could be trialled to build upon our work.
We anticipate the push to improve VTE scoring on EPR to continue due to the clinical importance of VTE prevention and hope that the issues we identified with staff will be resolved. Although we did not reach our target of 95%, we have shown a vast improvement from baseline measurements.
There were a number of limitations with our project and data collection methods. Although we collected data over three consecutive dates to monitor our interventions at the end of each cycle, continuous data collection daily throughout the project would have strengthened our findings and eliminated any bias. The data would have been more representative and excluded fluctuations in normal variance over project period. Furthermore, because we always collected our data on a Wednesday, Thursday, and Friday for continuity, continuous data collection would have excluded any bias on those days and allowed us to see if our improvements were maintained over the weekend. A full week was excluded from our data analysis due to the to the junior doctors' strike - a decision influenced by the fact that we felt results would have been skewed by additional stress on the department due to reduced staffing levels. Additionally as formal statistical analysis was not undertaken, there is a possibility that our results could have been due to chance.
Another limitation of our data collection when we were recording whether the VTE score assessment was completed on EPR we only took a ‘snap-shot’ when auditing and checked at 5:00pm. However, HBC has a high patient turnover and VTE assessment needs to be completed within 24 hours; therefore, looking at one-time point may not be entirely representative and an under-estimation. This could have been improved by also recording whether VTE assessment had been completed for postnatal patients who had been admitted in that 24 hour period. However, any patient sent home within those time limits (for example spontaneous vaginal delivery in a well woman, discharged six hours later) would have been missed. We also did not check for patient overlap day to day, although the high turnover on HBC means that this should be minimal and it is unlikely to have had a significant impact on results.
In hindsight, there were many improvements we could have made, particularly to our methods of data collection, that would have strengthened our project. We also recognise that the problems we discovered regarding recording VTE assessment on EPR are intrinsic to GSTT and may not be directly applicable to other trusts. Despite this, we feel we have had a significant impact on VTE assessment documentation rates, and we hope that we, and readers of this paper, will be able to take what we have learnt from this reflection and apply it to future projects. Improving VTE assessment rates is an important issue for all trusts, and we hope that applying similar, if not identical, have an impact elsewhere. We hope in particular that our project has proved the importance of raising awareness and staff education in successful quality improvement.
Conclusion
In conclusion, prevention of VTE is a vital patient safety issue, particularly in high risk patients such as pregnant women. VTE is a major contributor to maternal mortality in the UK and the risk of a thrombotic events increases as pregnancy progresses, peaking post delivery.1 ,2 Our project re-iterates the value of educating staff on the importance of VTE assessment in improving completion rates - which is in line with the existing literature.7 Although we did not reach our aim of 95%, our results did show a vast improvement from baseline (from 20.7% to 92.3% at the end of our third PDSA cycle). The final value, 92.3%, is comparable to the national average from the most recent set of VTE assessment data (95.5% for the first quarter of 2016).10
We recognise that our loyalty card scheme is not sustainable in the long term. However, we hope that the improvements seen can be maintained due to the raised awareness among staff generated by this project. We believe that similarly structured projects, focused around education and raising awareness, could make significant impacts on VTE assessment rate in other healthcare settings. In our Trust, the next steps for this project include acting upon the feedback we received from staff about the process, and attempting to streamline the process by introducing integrated IT systems, which make VTE assessment mandatory.
Acknowledgments
We would to thank the obstetrics department at St Thomas' Hospital for their support of and cooperation with this project.
Footnotes
Declaration of interests The authors declare that they have no conflicts of interest.
Ethical approval This project was exempt from ethical approval as the work was deemed an improvement study and not a study on human subjects; local policy meant that ethical approval was not required.