Article Text

Abstract
Streptococcus pneumoniae infection is associated with high morbidity and mortality in low income countries. In Nepal, there is a high lung disease burden and incidence of pneumonia due to multiple factors including indoor air pollution, dust exposure, recurrent infections, and cigarette smoking. Despite the ready availability of effective pneumococcal vaccines (PNV), vaccine coverage rates remain suboptimal globally. Quality Improvement (QI) principles could be applied to improve compliance, but it is a virtually new technology in Nepal.
This QI study for Patan Hospital sought to introduce the concept of QI there, to measure the baseline pneumococcal vaccination rate of qualifying adult patients discharged from the medical wards and to assess reasons for non-vaccination. QI interventions were instituted to improve this rate, measuring the effectiveness of QI methods to produce the desired outcomes using the Model for Improvement, Plan-Do-Study-Change (PDSA) methodology.
In the three week baseline assessment, 2 out of 81 (2%) eligible patients recalled ever receiving a prior pneumococcal vaccine; 68 (84%) unvaccinated patients responded that they were not asked or were unaware of the PNV. After the QI interventions, the pneumococcal vaccination rate significantly increased to 42% (23/56, p<0.001). Post-intervention, the leading reason for non-vaccination was cost (20%, 11/56). Only 5 (9%) unvaccinated patients were not asked or were unaware of the PNV, a significant change in that process outcome from baseline (p<0.001).
Quality improvement measures were effective in increasing pneumococcal vaccination rates, despite the limited familiarity with QI methods at this major teaching hospital. QI techniques may be useful in this and other efforts to improve quality in resource-limited settings, without great cost.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Streptococcus pneumoniae is the most common cause of bacterial pneumonia, meningitis and bacteremia.1 Pneumonia mortality rates in adults range from 10% to 30% and pneumococcal infections are responsible for 1.6 million deaths annually by recent WHO estimates.2 ,3 In a review of pneumococcal disease rates in Asia, the most common co-morbidities included bronchopulmonary disease, cardiovascular disease, malignancy, and diabetes mellitus.3 In Nepal, lung disease is extremely prevalent; chronic obstructive pulmonary disease [COPD] alone accounts for 43% of the adult non-communicable disease burden in Nepal4 and was the most common comorbidity in a study of patients with community acquired pneumonia in a tertiary hospital in western Nepal.5 Indoor air pollution, dust exposure, recurrent infections, and high cigarette smoking rates all contribute to the high lung disease burden in Nepal.6–8
The 23-valent, non-conjugated, pneumococcal polysaccharide vaccine, which contains 23 of the most common and virulent serotypes, is recommended by the United States Center for Disease Control and Prevention, advisory committee for immunization practices (ACIP) for all adults age 65 and older or adults 19-64 years old that are considered high risk due to an underlying medical condition.9 For qualifying patients, this is considered standard of care before hospital discharge in the United States. Prior vaccination with pneumococcal vaccine has proven effective in improving survival and decreasing risks of respiratory failure and other complications.1 Despite the recommendations and the availability of an efficacious and inexpensive vaccine, vaccination rates remain suboptimal globally, especially in low income countries such as Nepal.
Background
Hospital systems in Western countries have widely implemented quality improvement (QI) initiatives to increase pneumococcal coverage rates and assess reasons for missed opportunities.10 ,11 Quality improvement is a sustainable method to improve quality of care, standardize delivery of medical services, and potentially decrease costs for patients and health systems.12–14 It is also becoming apparent that resources alone are not sufficient to improve healthcare without a concurrent commitment to quality that is locally relevant.15
Quality improvement is a relatively new concept in Nepal just recently getting traction in larger teaching hospitals. However, the principles can be applied to improve hospital discharge vaccination compliance.16 ,17 In a review of the literature, no study has formally evaluated pneumococcal vaccination rates in Nepal at the hospital level in the adult population.
Patan Hospital, located in urban Kathmandu, Nepal is one of the largest teaching hospitals in the country. The 450-bed hospital has 50 medical inpatients (non-ICU) at any given time in two public wards and one private ward, and between 1 and 15 daily discharges typically. The bed occupancy rate is >95%. Two teams of doctors, including house officers, care for patients. Patan hospital utilizes paper medical records for all inpatients (all documentation in English).
The high proportion of patients admitted for pneumonia at Patan Hospital prompted us to conduct an assessment of current pneumococcal vaccination rates and trial the first ever QI initiative to improve vaccination rates. The primary aim of this study was to increase the pneumococcal vaccination rate of medical inpatients at discharge to 60% by the end of the six-week study period rate using Plan-Do-Study-Act (PDSA) methodology. Our study team consisted of two attending internal medicine physicians who worked full time at Patan hospital and two medical students.
Baseline measurement
To assess current vaccination rate and reasons for non-vaccination, nurses were given a simple form to complete for every qualifying patient at discharge that documented the patient's age, gender, qualifying diagnosis at discharge, prior pneumococcal vaccination, and if not, the reason (Supplementary figure 1A). Given the variability of prior documentation in the paper charts, the determination of the patient's baseline vaccination status included their verbal report. Baseline vaccination data was gathered from 81 patients over a period of three weeks. During baseline data collection, nurses were informed about the study and how to accurately complete the data collection form, but doctors other than the authors were unaware of the study.
Supplementary figure 1
Design
Patients
All patients included in this study were adults discharged from the medical wards at Patan Hospital, in Kathmandu, Nepal from June-August 2014. The study was approved by the Institutional Review Board (IRB). Qualifying patients for pneumococcal vaccination had never received the vaccine previously, were not allergic to any vaccine components, and were age 65 years old or greater. Additionally high risk patients 19-64 years old were considered if they had one of the following: chronic cardiovascular, pulmonary, kidney or liver disease, diabetes, cigarette smoker, individuals with decreased immune responses or defective immune defenses (functional or anatomic asplenia, immunosuppressive conditions, post organ or bone marrow transplantation) or iatrogenic immunosuppression (on therapy with alkylating agents, anti-metabolites, or systemic corticosteroids).
Study Design
Our quality improvement initiative was designed using the Institute for Healthcare Improvement framework, model for improvement,18 which utilizes rapid PDSA cycles.19 At the beginning of this study there was no process for administering vaccinations (pneumococcal or other) at hospital discharge. Vaccinations given in the outpatient or inpatient setting were inconsistently recorded directly in the chart. No data on current pneumococcal vaccination rates of patients was available, though it was anticipated to be less than 5%. Therefore, the first step was to evaluate the current pneumococcal vaccination rate in Patan Hospital. The primary aim of this study was to increase the pneumococcal vaccination rate at discharge to 60% at the end of the six-week study period using low cost QI interventions. The overall average vaccination rate in the US is about 60%, so we chose to target the same goal. An additional process aim of this study was to assess whether QI methods targeting change to the health care system would be effective in producing the desired outcomes, given the limited familiarity with QI initiatives at Patan Hospital. After initial baseline assessment, further PDSA cycles gathered feedback and assessed the impact of QI interventions.
Strategy
The reasons for non-vaccination in the baseline assessment guided our choice of QI interventions. Interventions implemented included: provider and nurse education, a standing order issued by the chair of medicine for nurses to vaccinate eligible patients at discharge, and a new medical record form indicating whether the pneumococcal vaccine was administered and reasons if not vaccinated.
Our informal assessment suggested that providers (doctors, residents, nurses) had poor knowledge of the pneumococcal vaccine. In the first PDSA cycle, a presentation about pneumonia and the pneumococcal vaccine was presented to doctors, residents and nurses at Patan Hospital to increase awareness of the vaccine and its current low usage in the hospital. Physicians and nurses were receptive to the presentation and saw an opportunity to improve patient care. It was an important initial intervention, however we anticipated that greater changes at the system level would be needed to increase vaccination rate appreciably.
After education, a standing order was issued allowing nurses to vaccinate patients without a patient-specific order from the discharging physician as the second PDSA cycle. We anticipated that empowering nurses would be more effective than provider education alone. Standing orders have been successful in numerous western institutions, especially in vaccination campaigns. It is an easy and permanent intervention. Paper notices were placed in nursing station as a reminder of the standing order. The thought process behind the standing order and the goals of the study were discussed with all the nurses at the nursing stations in Nepali (by a physician fluent in Nepali) prior to implementation of the standing order. Again, nurses were receptive and cooperative with this intervention.
The baseline form was modified for the intervention phase to include acceptance of vaccination, or the specific reason for the refusal (Supplementary figure 1B). Nurses were required to sign and date the forms. The form was attached to the discharge summary, and itself acted as one method of intervention by reminding nurses of the standing order, providing a checklist they could utilize, as well as serving as a means of data collection. The main feedback from nurses related to the best timing to give the vaccine. Discharge time could be hectic, many inquired if they could give the vaccine earlier in the morning if a patient was presumed to be discharged that day.
All forms were collected, regardless of vaccination status but only completed forms were included in the total. Post-intervention vaccination data was gathered from 56 patients over a period of three weeks. Patient numbers were dependent on daily discharges, which fluctuated throughout the study period. Data from the forms was maintained in an excel spreadsheet. Throughout the study, demographic information missing from the forms completed at discharge (i.e., qualifying diagnosis) was found later in the patients' medical charts.
Results
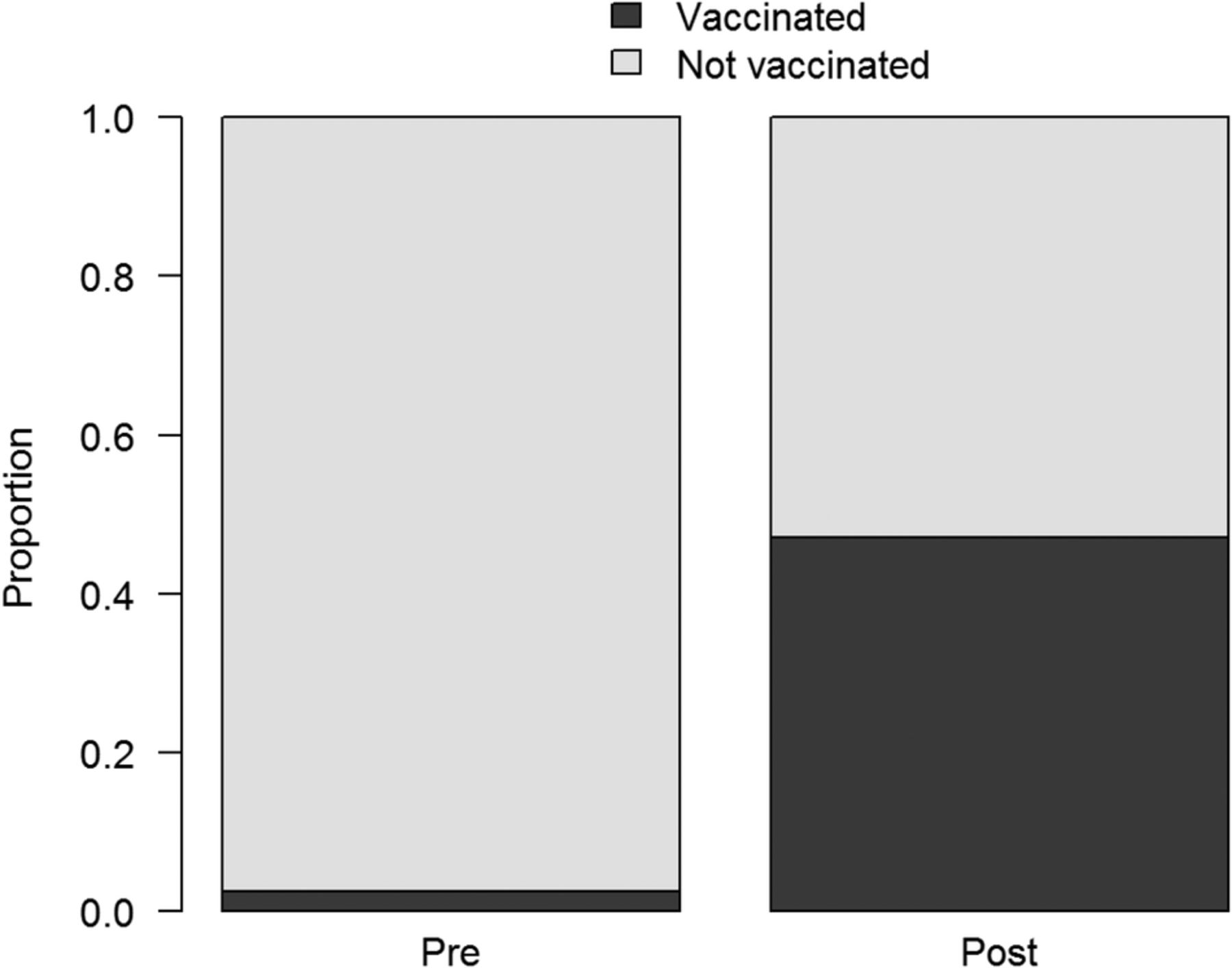
Our primary outcome was the improvement in the percentage of patients receiving the vaccination after the QI interventions. The baseline pneumococcal vaccination rate in Patan Hospital showed 2 out of 81 (2.5%) eligible patients surveyed in a three-week period reported a prior PNV (Figure 1). There was a consistent lack of daily vaccination during the baseline assessment phase. In the post-intervention phase, only one patient reported a prior PNV. After QI interventions, the pneumococcal vaccination rate at the time of discharge significantly increased to 42% (23/56, p <0.001) (Figure 1). Reasons for non-vaccination were assessed initially and post-intervention. In the initial assessment, most unvaccinated patients responded that they were not offered or were unaware of the vaccine (84%, 68/81), with other reasons, unspecified, (6.2%, 5/81) and cost (4.9%, 4/81) the next most common responses, respectively (Supplementary Figure 2). Post-intervention, the leading reason for non-vaccination was cost (19.6%, 11/56). Patient refusal for “other reasons” was given by 12.5% (7/56) of patients, followed by lack of vaccine availability in Patan Hospital at the time of discharge (10.7%, 6/56). Only five (8.9%) patients were not offered, or indicated they were unaware of the vaccine post-intervention (Supplementary figure 2). The proportion of patients offered the vaccine was significantly higher (p <0.001) post-intervention compared to baseline data, indicating an improvement in a key process outcome. Control chart analyses showed improved vaccination above baseline during the post-intervention phase (Figure 2). The improvement was gradual and fluctuated from day to day. There was a slight increase after provider education and a greater increase noted after the addition of the standing order and the form reflecting those changes. The overall vaccination rate in the first week was higher than the two subsequent weeks. As can be seen in Figure 2, vaccination slowed on the tenth day of the intervention phase when the vaccine became unavailable, followed by two days of limited availability.
Supplementary figure 2
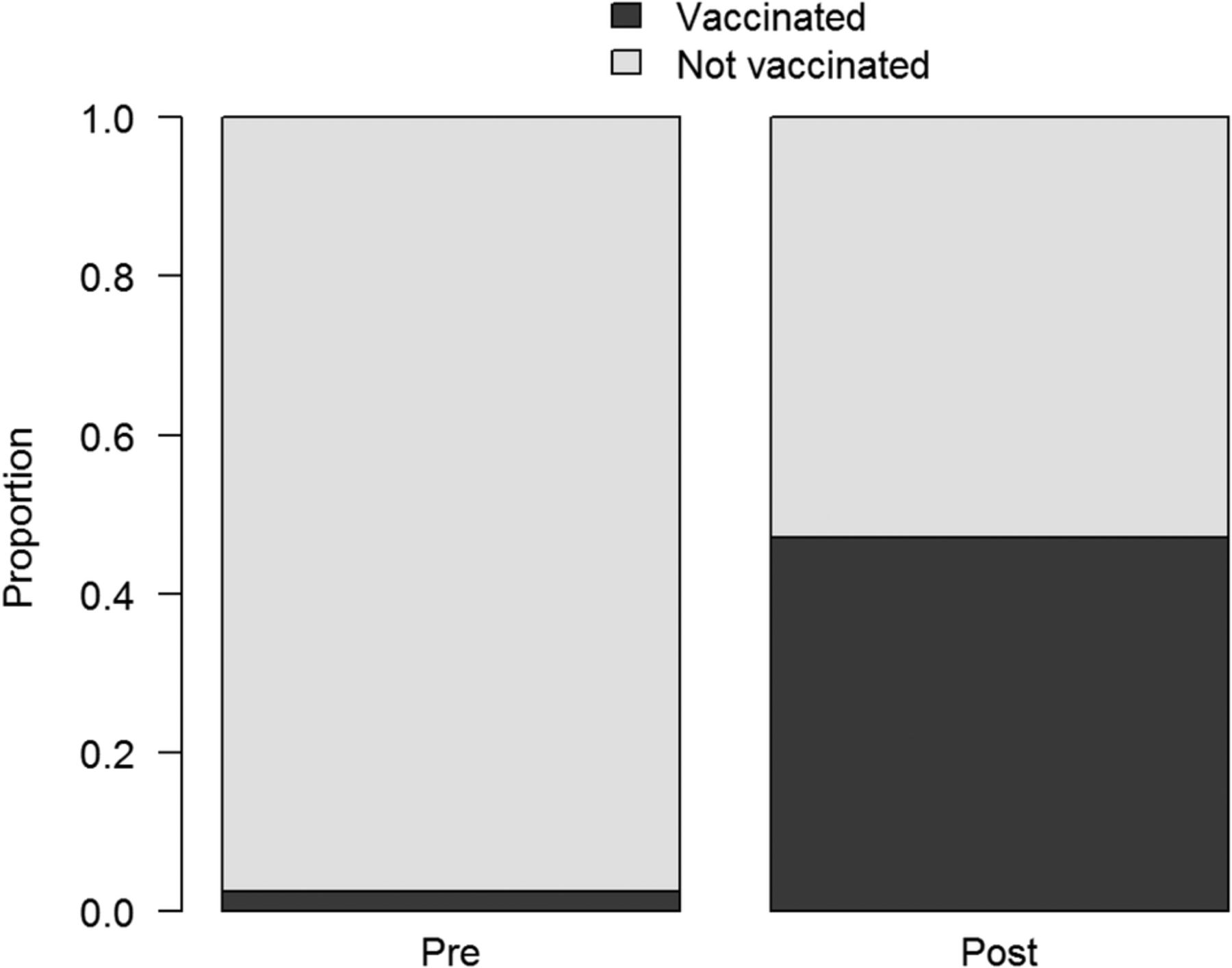
Comparison of pneumococcal vaccination pre and post-intervention. Baseline vaccination rate at Patan hospital before and after QI interventions, (2.5% vs 42%, p value <0.001). (Pre N=81, Post N=56).

{kind=link}
{kind=link}
Control chart analysis of daily vaccination rates. A) The average proportion, lower confidence limit (LCL), and upper confidence limit (UCL) were calculated using the pre-intervention (baseline) data alone. B) Percent of patients vaccinated by discharge date. The sizes of the points reflect the sample size per day (larger points indicate more discharged patients on that day). The timing of the two PDSA cycles is labeled. The blue arrow indicates when the vaccine became temporarily unavailable
Lessons and limitations
Quality improvement measures are not commonplace at Patan Hospital and therefore awareness was a barrier to initial implementation. Institutional leadership support and willingness to improve the quality of care from physicians and nurses was crucial. The initial staff feedback was quite positive, especially among the newly empowered nurses, but there were challenges. It became apparent that an enhanced tracking system was needed for recording vaccinations. Also, nurses noted the hectic nature of the discharge process caused some missed vaccination and questioned if there was a better time to do it. A shortage of the pneumococcal vaccine occurred by the second week post-intervention, followed by a decrease in vaccination momentum. Addressing the inconsistent supply of the pneumococcal vaccine is an important issue for follow up studies and crucial for sustaining a high vaccination rate long term. Sustainability will also be limited by the turnover of residents and physicians at the hospital. Provider education was a beneficial intervention in this study, but will need to be repeated to maintain long term effectiveness. The main limitations of this study were the small cohort of patients and short study period. A repeat, and longer study would be beneficial to validate the long term effectiveness of the interventions in sustaining the vaccination rate. The standing order and form at discharge are still in use. Despite these limitations, we feel these results are sustainable and predict similar low resource settings could benefit from similar QI interventions. The costs for this project were negligible. No additional staffing or resources was necessary outside of the study team.
Conclusion
These QI interventions using simple PDSA cycles significantly increased the pneumococcal vaccination rate of patients discharged from Patan Hospital's medical wards. The QI interventions aimed to increase provider awareness of the vaccine, and distribute responsibility of vaccination by allowing nurses to vaccinate every qualifying patient under a standing order.
Initially, physicians were rarely ordering the pneumococcal vaccine at discharge and the majority of patients reported they were unaware of the vaccine. There is less of an emphasis on pneumococcal and other adult vaccinations in Nepal, and in many other countries in Asia. A study in South Korea identified lack of awareness of the pneumococcal vaccine as the main barrier to vaccination in 75% of patients surveyed, with negative clinician attitude and patients' belief that they do not need the vaccine as other frequent responses.10 Therefore, provider education was chosen as a necessary and important intervention in our study, and also allowed us to clarify the other interventions-the standing order and updated discharge form reflecting this new policy. Continued education of health professionals will likely be necessary to encourage and sustain the vaccination rate. Standing orders have been successful in increasing vaccination rates in numerous hospitals, however they are often in the form of an electronically-generated prompt that appears in the EMR system during a patient encounter.11 This study issued a standing order, as Patan Hospital does not have an EMR system. This study utilized a ‘prompt’ from the discharge checklist form, which also served as our means of data collection. Nurses were receptive to this change and our results show that they were consistently offering the vaccine to patients. Patient education and empowerment is another common QI intervention that should also be employed in subsequent improvement cycles.
Following interventions at Patan Hospital, the percentage of patients offered the vaccine, by doctors or nurses, increased significantly, resulting in many more vaccinations. The main reason for non-vaccination shifted from a primarily provider and hospital factor to a patient factor. There was no formal assessment of patient's attitudes and beliefs, but from our observation, patients were generally receptive to getting the vaccine when asked. There are several patients in each room at Patan Hospital. We observed patients asking for the vaccine after they heard it being offered to another patient. Mistrust in vaccine efficacy or fear of side effects were never chosen as a reason for patient refusal on our data collection form. The main patient barrier we found post-interventions was cost.
Most medical care in Nepal is fee-for-service, with insurance generally not available. Patan sees many patients from low socioeconomic levels, and the vaccine is considered expensive (1000-1500 rupees, average monthly income is 10,230 rupees) for an average Nepalese patient. Despite this, most patients were eager to be vaccinated. There are limited studies on the economic impact of community acquired pneumonia (CAP) in Asian countries, but two cost-effectiveness analyses in Taiwan and Japan suggested a decrease in medical costs as well as a decrease in the incidence of CAP with the use of the pneumococcal vaccine, especially in older patients and those with co-morbidities.21 ,22 For most patients, the cost of the vaccine is small compared to the medical costs that would be incurred by hospitalization for CAP.
This study involved a small cohort of patients over a short period of time, designed as an initial pilot to assess the utility and feasibility of using QI measures. However, the initial results are promising and have highlighted the feasibility of making quality-driven improvements in a very low resource setting. This study has been a first step in the integration of QI with routine patient care at Patan Hospital. We plan to conduct a follow up assessment of pneumococcal vaccination rates that expands upon the results of this study. We also hope to apply similar QI techniques to other concerns in the hospital. Future studies for QI interventions in low resource hospitals should build off the implementation strategies and barriers identified in this study to develop and incorporate QI for patient care and provider capacity.
Acknowledgments
Funding support provided by Dr. Elaine Kohler Summer Academy of Global Health Research. The authors would like to thank the global health department at MCW, especially Stephen Hargarten and Tifany Frazer, for their support and mentorship. Staff at Patan Hospital for their cooperation and commitment to improving patient care.
References
Footnotes
Declaration of interests Nothing to declare.
Ethical approval The study was approved by the Institutional Review Board (IRB) at the Medical College of Wisconsin and the Institutional Review Committee (IRC) at Patan Academy of Health Sciences (PAHS).