Article Text

Abstract
Primary healthcare in Qatar uses electronic prescribing to reduce the risk of medication errors. Electronic prescribing is supported by computerized Physician Order Entry systems through Cerner (electronic medical record system). There are still prescription errors, despite electronic prescribing being in place for one year at West Bay Health Center. West Bay Health Center is a famous primary healthcare center in Qatar. It is a training center for the family medicine residency program, which is accredited by the accreditation council of general medical education international (ACGME-I). It serves a population of about 98,000 in Qatar with 35 physicians and 12 pharmacists.
The aim of this project was to decrease medication errors by 30% from baseline measurement (according to type of error) from October 2015 to March 2016. It was found that there was a discrepancy between the pharmacy medication list and the list within Cerner. A master drug index was created to eliminate the discrepancy. Training on the use of this index was provided through lectures and one to one education, with material also sent through email.
We found that there was some resistance from the physician side and therefore introduced a second intervention. We sent out a survey to find out more about these difficulties and provided more training and education.
Our results showed an decrease in the proportion of wrong dose errors from 11.8% to 10.6%, wrong name from 6.9% to 6.2%, wrong duration from 11.7% to 10.3%, and non-formulary drug errors from 2.6% to 1.6%.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Electronic prescribing was introduced to West Bay Health Center one year ago. Since then, the pharmacists noted that there were still prescription errors. Prescription errors were prevented through the pharmacist asking the attending physician to correct the order. However, this process usually increased waiting times for patients and thus impacted on patient flow.
There was therefore a need to find an alternative process/pathway to enable physicians and pharmacists to avoid these medication errors so that patient waiting times were not impacted upon.
The aim of this project was to decrease medications errors by 30% from baseline measurement (according to type of error) from October 2015 to March 2016.
Background
Medication error is an important factor which influences the quality of patient care. According to Barach et al, nearly 100 000 individuals per year in the US die of preventable medical errors.1 Medication errors have been identified as a major type of medical error. The Council of Europe2 and the British Department of Health3 defined medication errors as “any preventable event that may cause or lead to inappropriate medication use or patient harm”.
Medication errors are a common cause of malpractice claims against physicians. The Physician Insurers Association of American (PIAA) reviewed data on 117 000 claims and lawsuits and found that medication errors were the second most common cause for claims.4
Errors in medication ordering have been the primary identified source of preventable (adverse drug events) ADEs.5 Computerized physician order entry (CPOE) eliminates handwritten orders and reduces errors related to medication prescribing. Furthermore, CPOE enhances quality and efficiency by improving the completeness and legibility of orders. It offers clinical decision support and provides a means for standardizing practice.6 An epidemiological study of prescribing errors found a rate of 62.4 errors per 1000 medication orders. Of these errors, 31% were considered clinically significant and 64% were determined preventable with CPOE. In addition, 43% of prescribing errors that were previously classified as potentially harmful to the patient were determined likely to be preventable with CPOE.7
In light of these figures, it is not surprising that the Primary Health Corporation in Qatar recommends the use of electronic prescribing to reduce the risk of medication errors, Electronic prescribing is supported by a computerised physician order entry system which uses Cerner.
Baseline measurement
Baseline measurements were conducted by a senior pharmacist to study the existing medication errors in the electronic system (Cerner). The baseline data was collected using the medication error report tool which had been developed by the quality team (see Table 1). The team reviewed 635 items over a one week time period for medication errors which included: wrong name, duration and dose errors, non-formulary drugs.
Medication Error report Tool
The results showed the following pattern of medication errors; wrong name represented 6.9% of errors, wrong dose represented 11.8% of errors, wrong duration represented 11.7%, and non-formulary prescriptions represented 2.6% (see Table 2).
Types of medication errors
The team undertook a brainstorming session to discuss the most common causes of the medication errors. This revealed that there was a discrepancy between the pharmacy's medication list and the medication list on Cerner (Cerner had a hospital based formulary, not a primary health care oriented formulary).
Design
A master drug index was developed as an electronic folder which included all of the primary health care formulary medications. The aim of this intervention was to avoid mismatch between the medication list in pharma-net (for pharmacy) and power chart (for physicians). The index was developed to be included in the shared documents folder. Training of physicians on the use of this index was done through lectures and 1:1 education sessions. Materials were also sent out via email.
We noticed that there was some resistance from the physicians and pharmacists (pharmacists were not reporting errors). As a result, a survey was carried out to detect the root causes of the problem.
Physicians were given more training on using the master drug index and pharmacists were given training on the measurement of prescription errors.
Measurement of prescription errors was undertaken on a weekly basis by pharmacists and was reported to the quality committee. Data collection was undertaken using the medication error report tool. This project was undertaken from October 2015 to March 2016.
Strategy
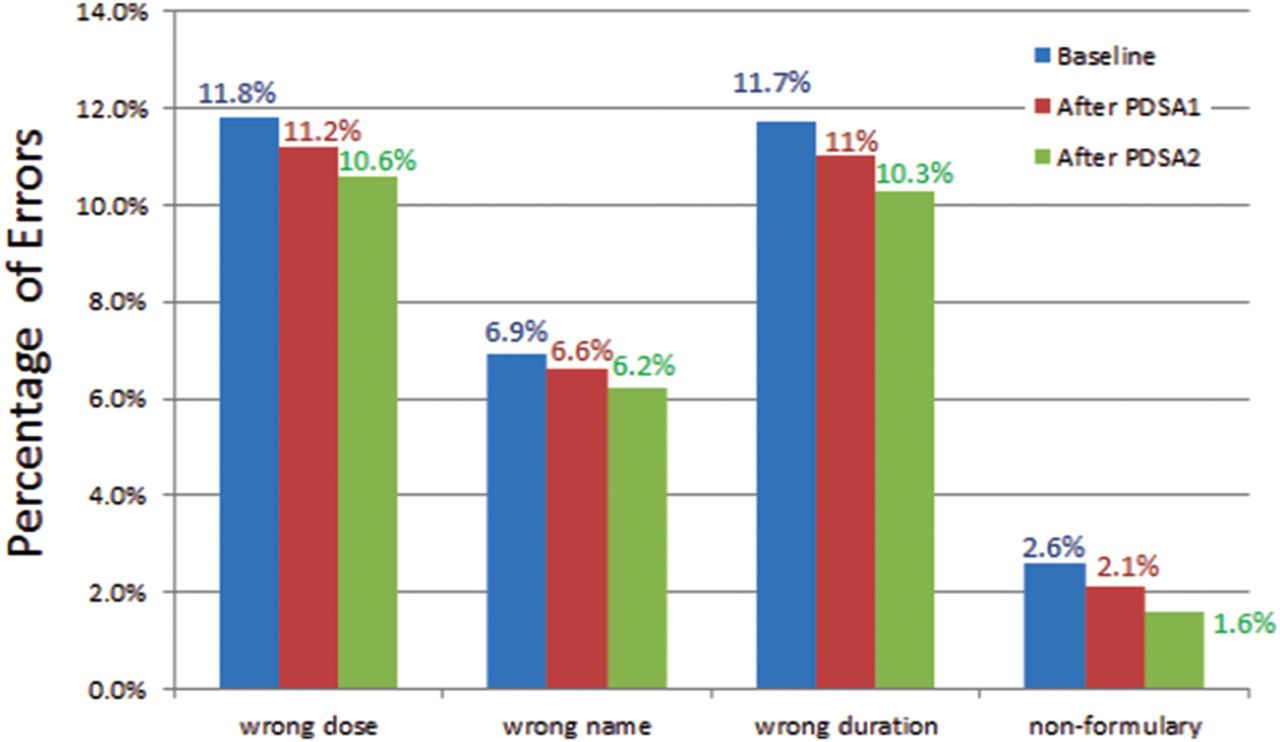
PDSA cycle 1: the aim of this cycle was to decrease medication errors by at least 50% from our target (15% from baseline measurement) by the introduction of the master drug index. Training was given to the residents and physicians on how to use the index and pharmacists were trained on how to audit the medication errors. There was a slight decrease in the medication errors: wrong dose decreased from 11.8% to 11.2%; wrong name decreased from 6.9% to 6.6%; wrong duration decreased from 11.7% to 11%; non-formulary prescriptions decreased from 2.6% to 2.1% (See figure 1).
{kind=link}
It was apparent that doctors were not using the master drug index and that pharmacists were also not recording errors on a regular basis.
PDSA cycle 2: A survey was undertaken to try to understand why the pharmacists, residents, and physicians weren't using the master drug index. We found that awareness among pharmacists was 80% and 100% among physicians. The most common cause of non-adherence to the master drug index for physicians was that they thought it was complex and difficult to use (50% of responses). The most common cause for pharmacists not recording errors was work overload in 100% of responses. As a result, we implemented more group education for physicians and assigned specific pharmacists to record medical errors on a daily basis (see attached PDSA and survey results for physicians). There was a decrease in the proportion of medication errors (wrong dose improved from 11.2% to 10.6%, wrong name decreased from 6.6% to 6.2%, wrong duration decreased from 11% to 10.3%, non-formulary prescription decreased from 2.1% to 1.6%) (See figure 1) (See supplementary - PDSA and survey).
Supplementary - PDSA and survey
Results
Figure 1 shows the proportion of medication errors by type at baseline after PDSA cycles 1 and 2. The data suggests an improvement of wrong dose error from 11.8% to 10.6%, of wrong name from 6.9% to 6.2%, of wrong duration from 11.7% to 10.3%, and of non-formulary drug errors from 2.6% to 1.6%.
This means that the intervention reduced wrong dose errors by 10% from baseline, reduced wrong name errors by 7%, reduced wrong duration errors by 12%, and reduced non-formulary errors by 38.5%.
In a landmark trial evaluating the impact on serious medication errors, the implementation of computerized physician order entry (CPOE) resulted in a 55% (10.7 vs 4.86 per 1000 patient days) reduction in the rate of serious medication errors across all stages of the medication use process.(8) The differences between our results and literature shows that we will need to undertake further interventions and monitoring to reach such international standards.
Lessons and limitations
A lot of lessons were learnt during this project. We learnt the importance of good team work between our pharmacists and physicians.
In terms of limitations, our results could have been due to chance/random fluctuations as we have only collected a small number of data points and we have not undertaken statistical testing. Continuation of our initiatives and ongoing data collection by the team is required to ensure that we are able to see a real improvement and sustainability.
Going forward, we will also need to consider the role of the organisation in training new employees on the master drug index. We feel it should be included in the training programs for physicians and pharmacists. This project could be tested in other primary care health centers in Qatar.
Conclusion
This project introduced a master drug index and, training for physicians and pharmacists. The data collected suggests a reduction in all types of medication errors when compared to baseline, however further data collection is required to show improvement.
The biggest change was seen in the non-formulary errors. Unfortunately we could not achieve our target of 30%. We plan to continue this improvement project.
Acknowledgments
We would like to acknowledge all of the West Bay Health Center staff for their kind contributions and efforts during the implementation of this improvement process.
We would like also to acknowledge family medicine residents in the Family Medicine Residency Program for their contributions and supervising faculty members.
Footnotes
Declaration of interests Nothing to declare.
Ethical approval The work was deemed an improvement study and not a study on human subjects, and local policy meant that ethical approval was not required.