Article Text

Abstract
Adults presenting to oral and maxillofacial surgery services are at high risk of psychological morbidity. Research by the Institute of Psychotrauma and the centre for oral and maxillofacial surgery trauma clinic at the Royal London hospital (2015) demonstrated nearly 40% of patients met diagnostic criteria for either depression, post traumatic stress disorder (PTSD), anxiety, alcohol misuse, or substance misuse, or were presenting with facial appearance distress. Most facial injury patients were not receiving mental health assessment or treatment, and the maxillofacial team did not have direct access to psychological services. Based on these research findings, an innovative one-year pilot psychology service was designed and implemented within the facial trauma clinic.
The project addressed this need by offering collaborative medical and psychological care for all facial injury patients. The project provided brief screening, assessment, and early psychological intervention. The medical team were trained to better recognise and respond to psychological distress.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Research at the oral and maxillofacial trauma outpatient clinic at the Royal London Hospital, London, found that patients presenting with facial injuries displayed high rates of psychological disorder in both the early phase after injury, and at follow up some months later. Depression, PTSD, anxiety, alcohol and substance use and dependence, and distress about facial appearance were prevalent at both time points. (Wilson N, Dain V, Heke S, et al. Prevalence and predictive factors of psychological morbidity following facial injury: A prospective study of patients attending a maxillofacial outpatient clinic within a major UK city, 2015. [Submitted for publication]) Thirty nine percent and 27% of patients met criteria for at least one psychiatric diagnosis at one to three months, and six to nine months after injury respectively. The psychological impact of the trauma also extended past patients to their carers and families in some cases.
There are substantial health, social, and economic costs for individuals and communities in providing health and social care associated with untreated mental health problems.1 Additionally relevant to the maxillofacial clinician is that some psychological disorders, for example chronic PTSD, are associated with noted impairments in recovery from physical injury. At the time of research in 2013, there was no psychological support present in the clinic; patients were not receiving mental health assessment or treatment, and the maxillofacial team did not have direct access to psychological services. The medics in the facial trauma clinic have little time or training to deal with the psychological needs of their patients, as the care of their physical needs takes priority, and they are usually already dealing with a backlog of patients to treat. Prior to the project, the standard route for any psychological issues identified by clinicians in the facial trauma clinic was referral to their GP. However, it does not routinely follow that informing GPs of the need for psychological follow up results in patients accessing these services. Where attendance to their GP does occur, GPs do not always identify or assess patients for conditions such as PTSD following the occurrence of a traumatic event.
Background
Patients attending oral and maxillofacial trauma services have been identified as presenting with a high risk of comorbid psychological morbidity, with between 23% and 41% of individuals presenting with symptoms of depression, anxiety disorders, and post traumatic stress disorder (PTSD), with significant morbidity even up to one year post injury.2–6
Common mental health disorders, including depression, anxiety, PTSD, and appearance related distress are treatable with evidence based psychological interventions within primary care services. However, various barriers to psychological care following facial injury have been observed, including an underestimation of patients' psychological needs, low utilisation of psychological screening tools, unclear pathways of care to mental health services, and physicians underestimating their influence on patients' psychological treatment seeking behaviour in maxillofacial trauma clinics.7 ,8 The medics simply do not have the time or expertise to systematically identify which of their patients require psychological support. At best this results in haphazard signposting to psychological services, and at worst untreated mental health difficulties that result in significant distress, disability, and economic cost. Therefore, there is growing impetus to implement effective screening for psychological difficulties within maxillofacial services. As healthcare needs become more complicated, there is increasing need for a multidisciplinary team to form coordinated pathways of care, and in particular, for mental health care needs to be integrated with physical recovery for these patients.3 ,9
Baseline measurement
Researchers at the maxillofacial trauma outpatient clinic at the Royal London Hospital, London, collected data on the prevalence of psychological conditions in patients attending the clinic between January 2012 and March 2013. (Wilson N et al [submitted for publication]) The researchers observed that at one to three months post injury, nearly 40% of patients met diagnostic criteria for either depression, PTSD, anxiety, alcohol misuse, or substance misuse, or were presenting with facial appearance distress. Nearly 30% of patients met criteria for at least one psychiatric diagnosis six to nine months after injury. See table 1 for full details of prevalence rates.
Psychiatric Diagnoses across participants at each time point 1
Design
The study concluded that a collaborative care model that placed psychologists within the medical team would be the most reliable way of identifying psychological need, and facilitating referral to appropriate and accessible services for individual patients. Funding was secured for two clinical psychologists (one project lead supervising the service, and one working in the clinic), and a research assistant.
Strategy
The 12 month pilot psychology service was provided within the maxillofacial trauma outpatient clinic at the Royal London Hospital between September 2014 and September 2015. Two clinical psychologists (band 8b, whole time equivalent (WTE) 0.1, and band 8a, 0.6 WTE) and a research assistant (band 5, 0.2wte) were recruited. The band 8b clinical psychologist was the project lead and supervisor of other staff. The band 8a clinical psychologist spent 50% of their working time in the oral and maxillofacial trauma clinic across 1.5 days per week. Their role was to administer self report screening questionnaires, interpret the questionnaires, and respond to patients who needed immediate assessment and intervention, either in clinic or within a few days. The role of the research assistant was to support in the administration and interpretation of the screening tool when clinical demand was high, and to support the evaluation of the project. A screening that took approximately five minutes to complete was devised and administered to all outpatients. This was based on already validated psychometric questionnaires, eg the hospital anxiety and depression scale (HADS), that asked about depression, anxiety, PTSD, alcohol and drug use, risk to self (suicidal ideation), and facial appearance distress. It also asked if patients wanted, and consented to psychological consultation. As the clinic was extremely busy, and a significant proportion of patients were urgent new cases that were not pre-booked, eg they had attended A&E over the weekend, systematic liaison with the reception and nursing staff was required to ensure that all patients were screened. At the point of screening, patients were also given psychoeducation about common psychological responses and helpful coping strategies following traumatic events. The surgeons also liaised with the clinical psychologist and vice-versa, in cases of particular need or risk.
All patients who scored above cut off point on any of the subscales in the screening tool were approached by the clinical psychologist, and briefly assessed to determine their psychological needs. A range of self help leaflets, eg regarding anxiety, low mood, and PTSD, were available to give to patients in clinic, and brief psychological treatment was provided for coping with common psychological difficulties. Some of these patients were also offered follow up calls, emailed, or were seen at follow up appointments in clinic so further advice could be given, and a significant number were signposted for self referral, or referred to mental health services or non-statutory organisations. A range of therapeutic models were used by patients as the needs arose, including CBT, counselling skills, and affect focused therapies.
The service was continually assessed across the one year pilot period, by means of feedback from the medical and psychological teams, and service user representatives at regular board meetings. Patient feedback was also sought at the end of therapeutic intervention with the clinical psychologist.
No significant changes were made to the service during its running, however some minor adjustments were implemented. The screening tool was amended to include patient date of birth, address, and GP, to minimise the need for cross referencing with medical notes for follow up contact. Additional self help leaflets were devised in response to patient need, eg sharing difficult information with children, and guidance for carers.
As the service evolved, the clinical psychologist noted a significant number of patients who had more complex psychological needs than those common mental health difficulties as assessed through screening. These were identified through face to face meetings or phone contact, and included risk assessment (self injury and suicidality, violence towards others, child protection issues, vulnerable adult safeguarding, injury through domestic violence, lack of appropriate psychological service at critical recovery points, eg in brain injured patients); liaison with family members who were traumatised, and/or had become carers for facially injured patients; neuropsychological assessment; and coordination of mental health care for patients with complex needs. As a result, extra time was allocated to working with these patients by both the clinical psychologist and the research assistant.
Results
Data from 642 patients from the trauma clinic were collected between September 2014 and September 2015. The data on patient demographics, source of injury, presence of psychological conditions, and level of psychological intervention are illustrated in figures 1 to ⇓⇓⇓⇓6.

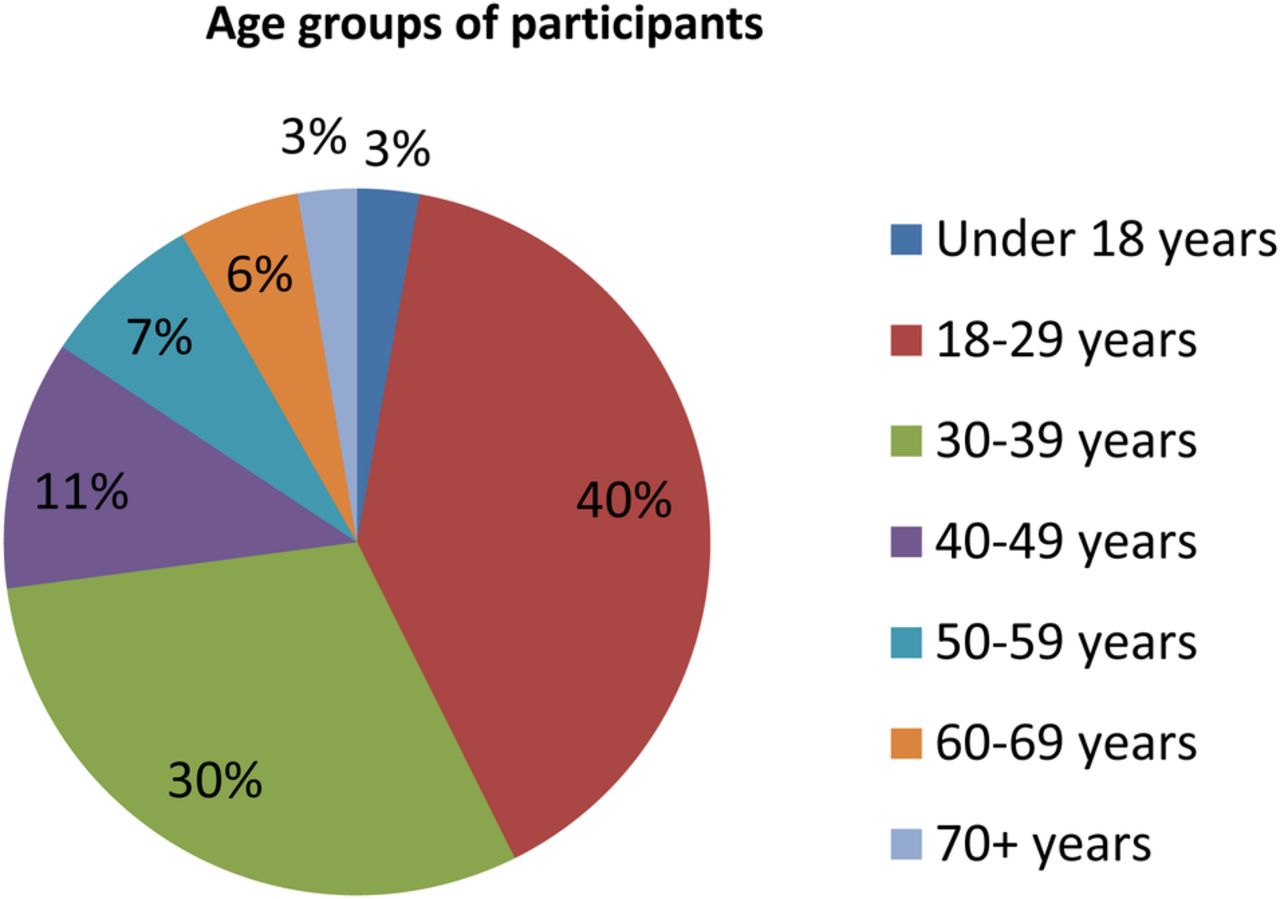
Patient Ages
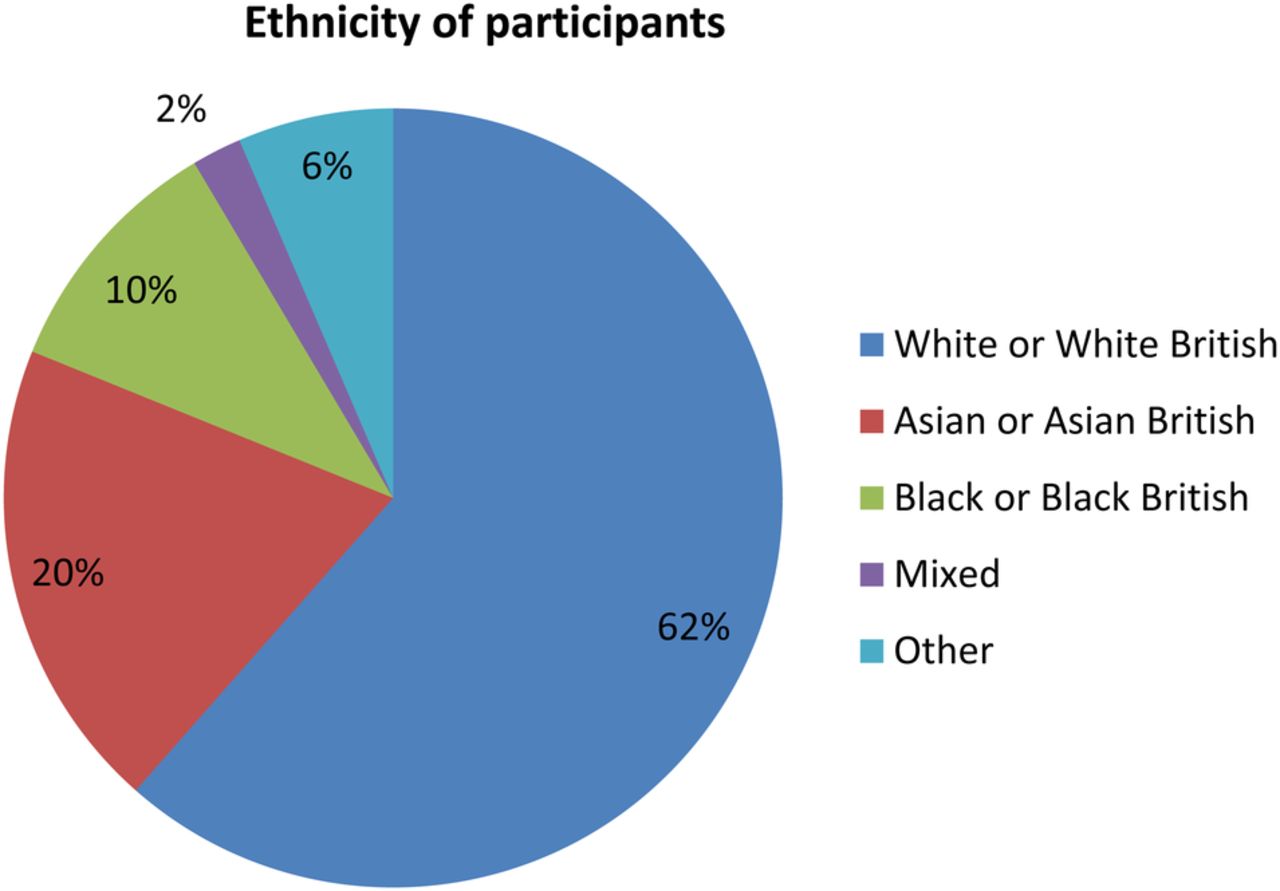
Patient ethnicity
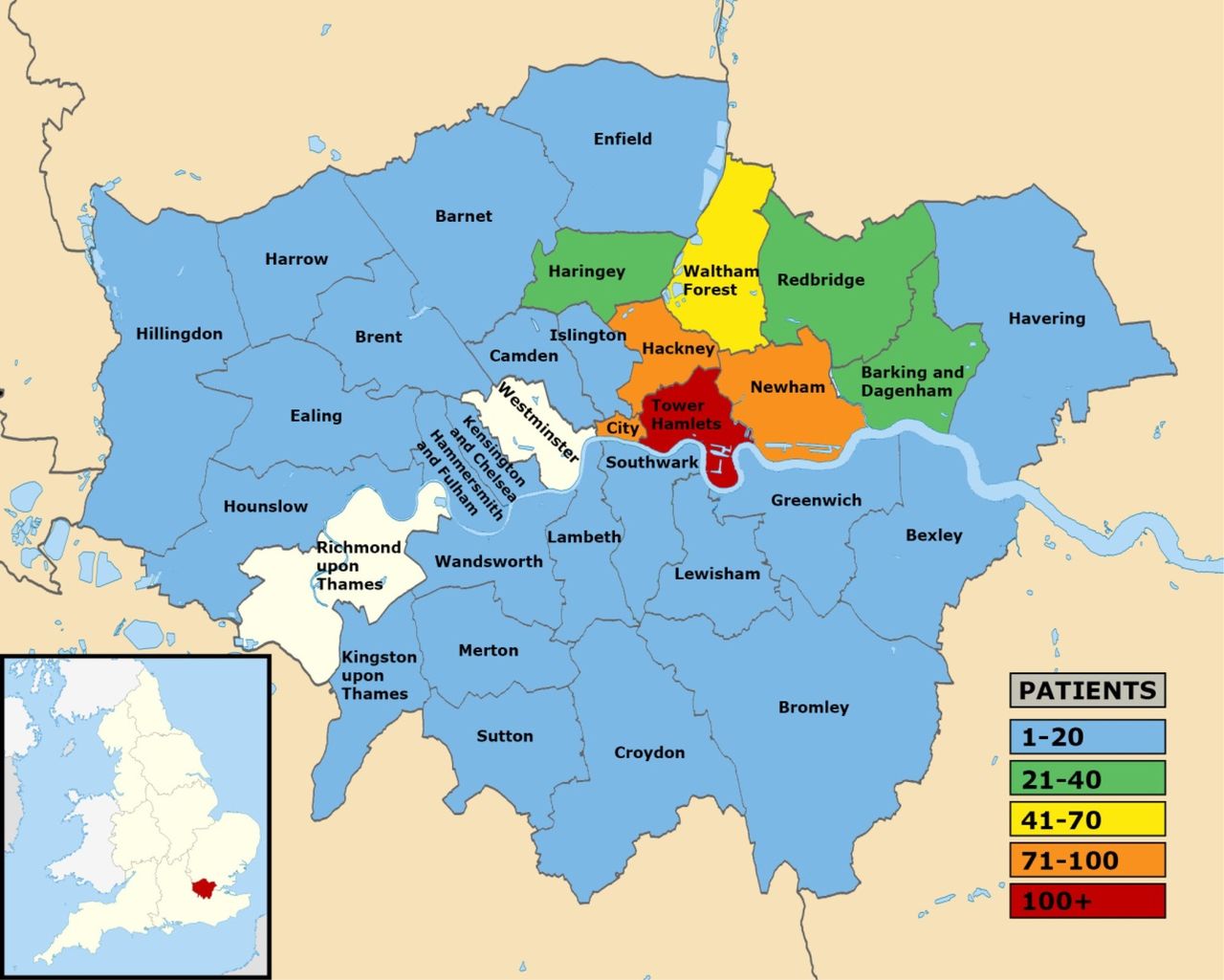
Geographical spread of Patients – With text: 85% of patients lived in a London Borough at the time of they attended the Centre.
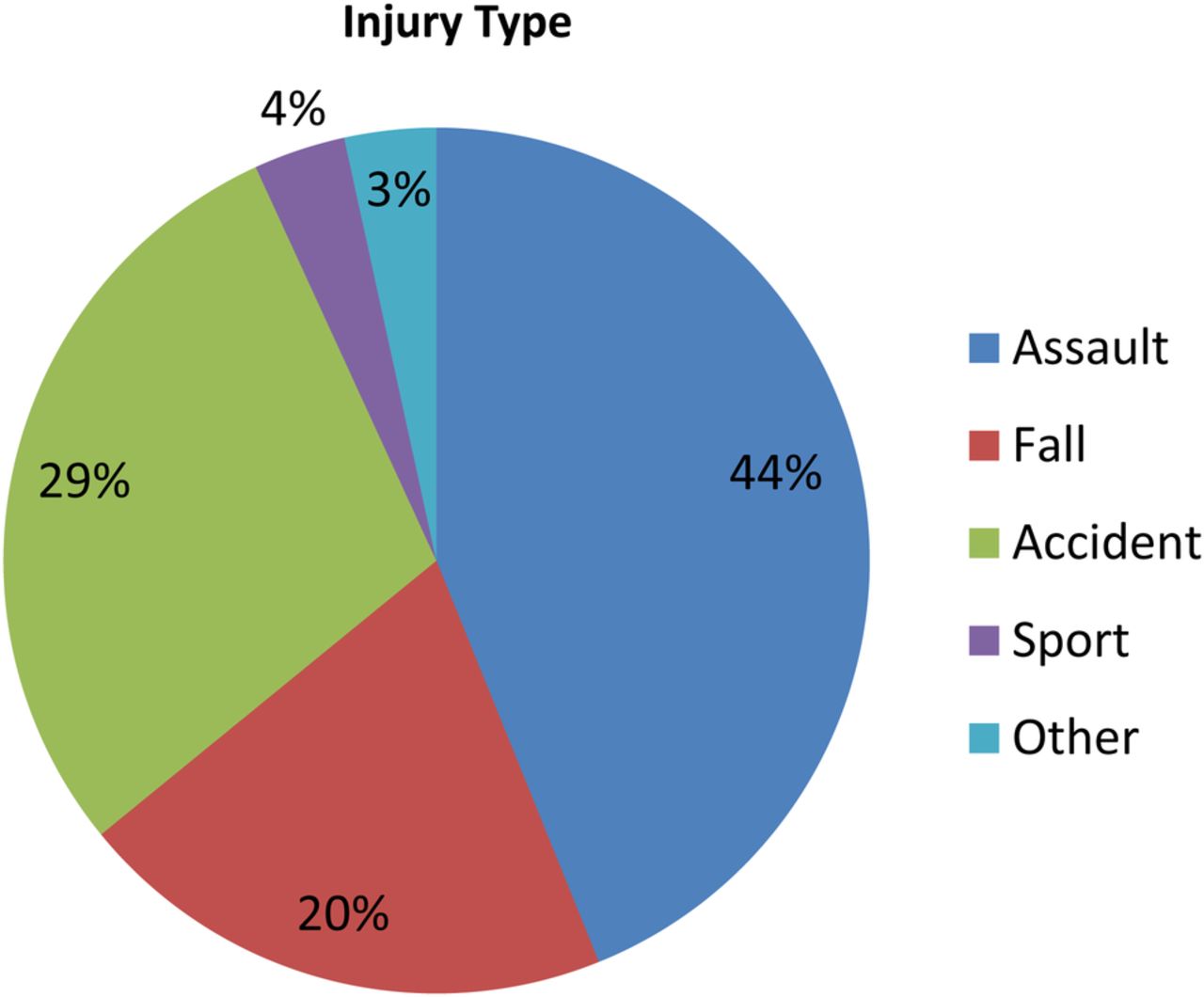
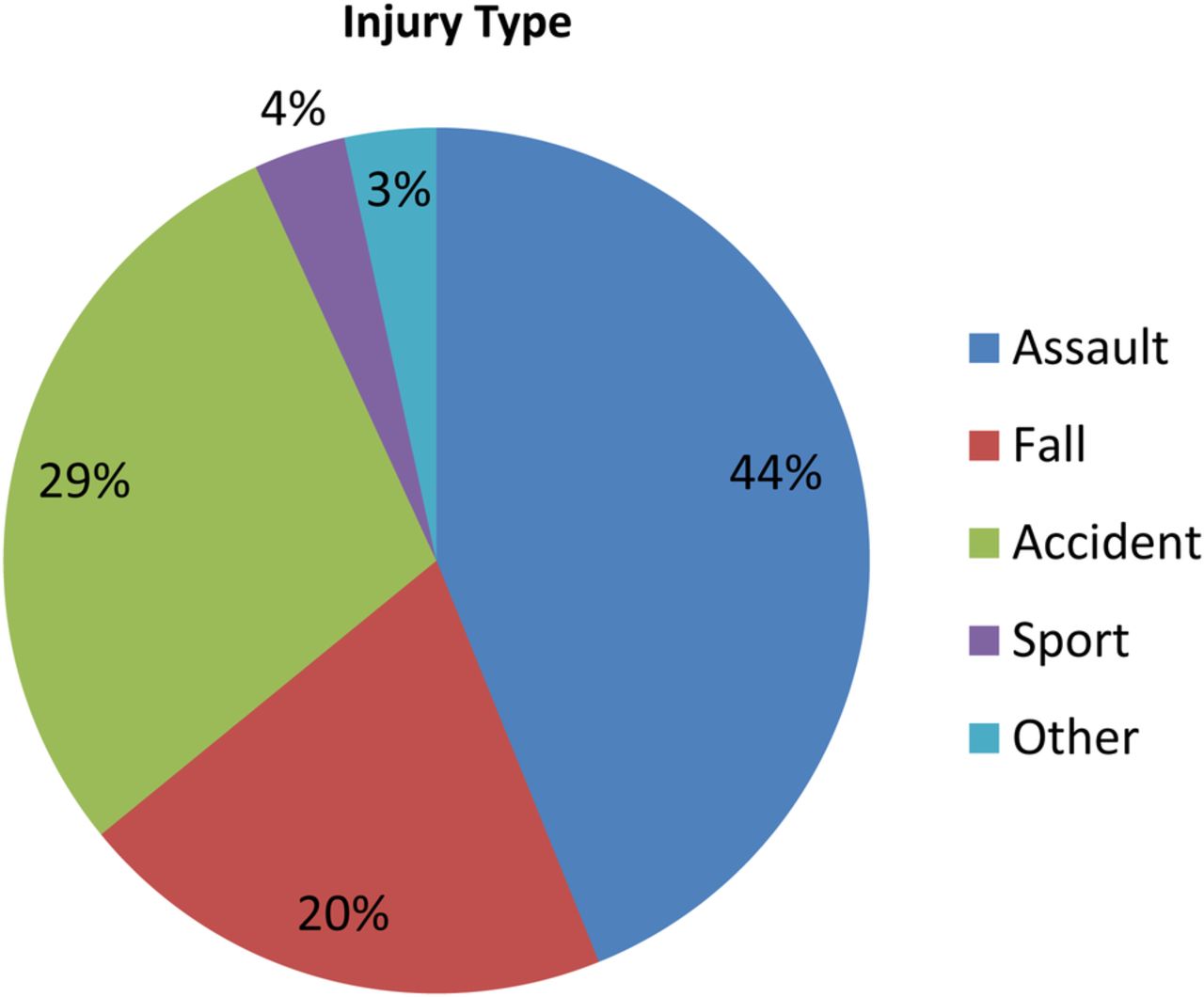
Source of Facial Injury

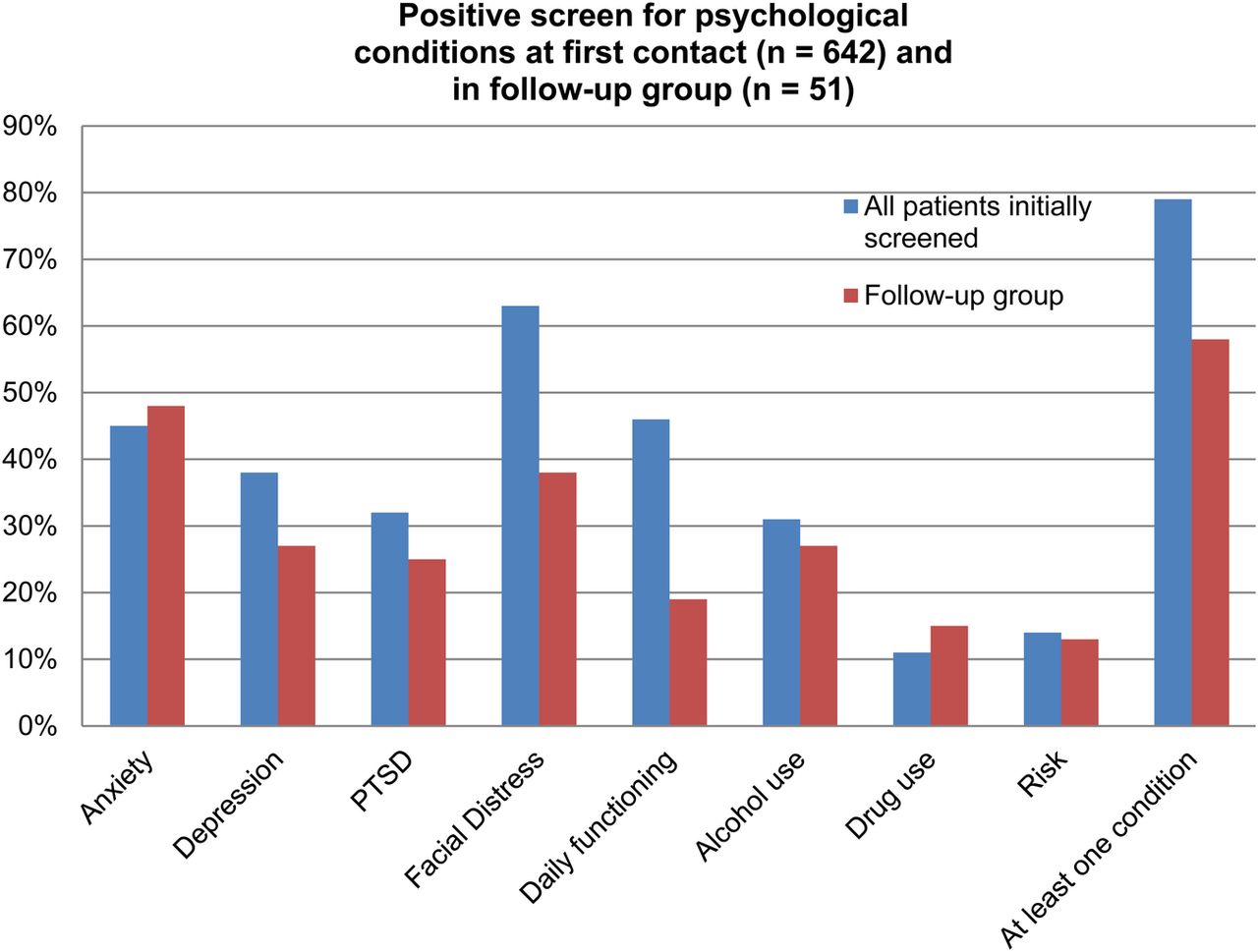
Prevalence of psychological conditions (n=642)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
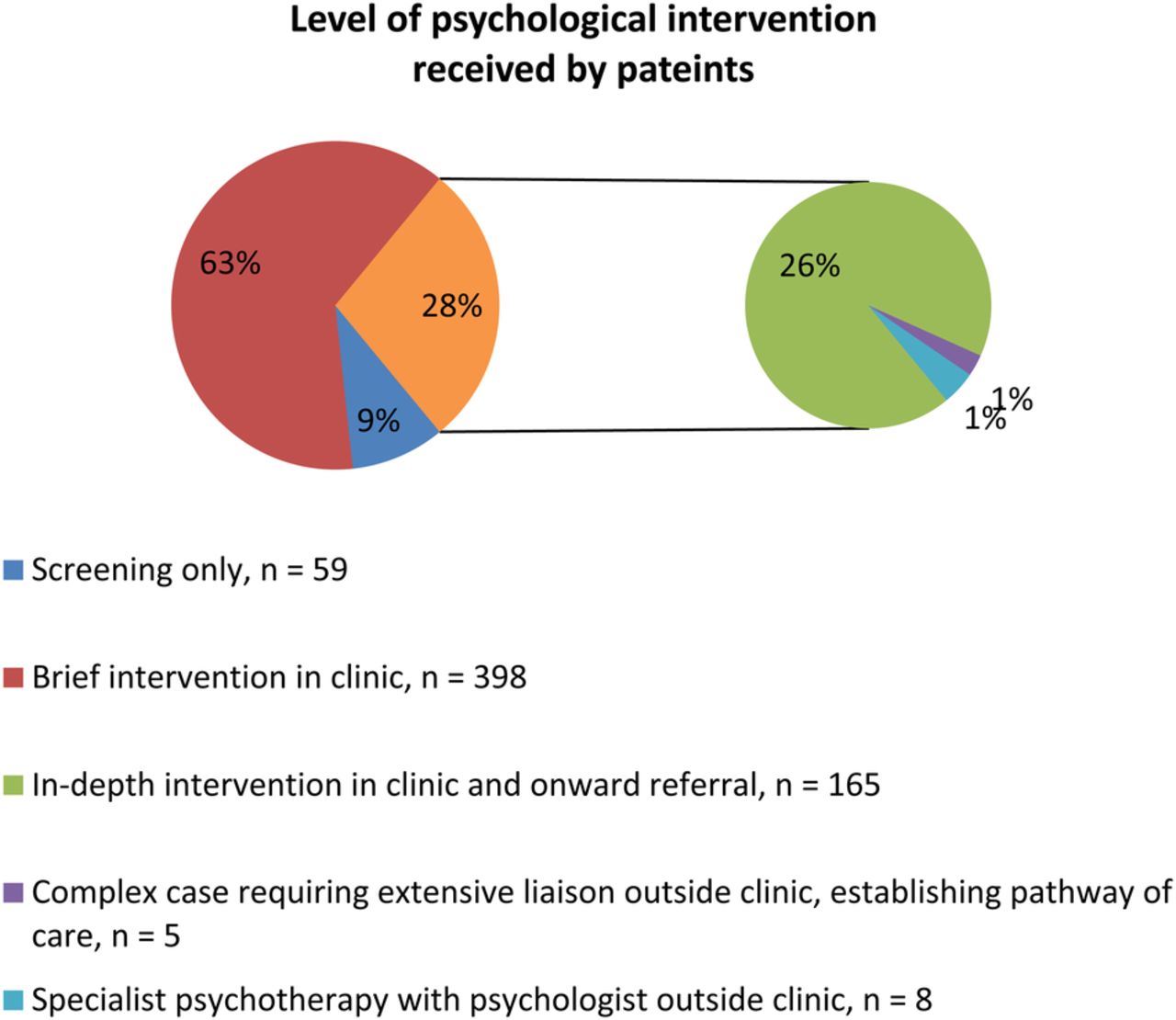
Level of psychological intervention received by patients
Seventy three percent (470) of patients screened were men, and 27% (172) were women. Almost three quarters (73%, 460) of patients were under the age of 40. The majority of patients (62%, 238) were white or white British. The highest proportion of injuries (44%, 269) were caused by assault, followed by accidents (29%, 178), and falls (20%, 124). Eighty five percent of patients lived in a London borough at the time they attended the clinic.
Fifty one patients were contacted three months after they first attended clinic to follow up on their current physical and psychological condition. While the proportions of people with each mental health condition had decreased at the second time point (see figure 5), the majority of patients interviewed (58%) still met the cut off for at least one mental health condition.
Further details of the demographics and proportions of patients with mental health conditions can be found in figures 1 to ⇑⇑⇑⇑6.
Out of the whole group of patients seen in the clinic (n=642), of those patients who received any psychological intervention, 78% said that the psychology service either slightly or significantly improved their experience of attending the maxillofacial trauma clinic.
The patients who were contacted at the three month follow up time point were also asked to give feedback on their experience of using the psychology service, in order to carry out a small scale evaluation of the service.
Core qualitative themes from patient feedback were as follows:
– Having someone to talk to about the psychological impact of their injury, being proactively approached within clinic, receiving empathy, validation, support, hope ,and having problems normalised was valued
– Patients felt the psychology service was highly relevant to their presenting needs.
– Patients had an improved understanding of psychological difficulties, and found the tools for managing psychological distress helpful
– Patients believed that their recovery would have been significantly worse without psychological input.
Core qualitative themes from a sample of physicians in the medical team were as follows:
– Rapid, flexible, integrated psychological care was beneficial to patients
– Addressing psychological issues facilitated medical recovery
– Families reported that they had also found psychological support very beneficial
– Their awareness of the psychological impact of facial injury had increased, and they would value more training in this area.
The impact of the psychology service was uniformly agreed among all stakeholders (medical team, patients, and psychologists) to be high. The introduction of comprehensive, expert, patient centred screening and psychological assessment into the clinic was a fundamental change in service delivery team.
Lessons and limitations
The key aim of this project was met; namely, to successfully introduce collaborative psychological care within an oral and maxillofacial trauma outpatient service in a busy London hospital.
However, there were some aspects of organisational culture that acted as a barrier to service implementation at times. As clinical psychology staff were employed by a local mental health trust, but working in a hospital run by an acute trust, communication and coordination was somewhat compromised by IT systems that were not interoperable, and access to useful patient data was not routinely facilitated for the clinical psychologist. This meant some replication of communication, for example medics had to receive paper copies of letters or reports about patients written by the clinical psychologist.
Securing protected, confidential, and accessible clinic space was also problematic, and both patients and medics recognised this limitation. Future service development would be dependent on this being provided.
Staff changes were a significant challenge. Both the band 8a clinical psychologist and research assistant left the project partway through the year due to maternity leave, although the project lead, who had also run the prior research project, remained in post. This ensured a basic level of continuity was retained, and the project lead oversaw recruitment, induction, and integration of new staff into the team. This resulted in an agreed break in the full psychology service for one month, and an extension to the project end date by one month. In addition to this, the evaluation of the project required additional human resources. Honorary psychology research assistants were recruited for substantial data entry tasks.
It is felt that the original ambitions were realistic given the available resources and time scales.
There were a number of specific learning points and potential areas for future improvement identified. The lack of access to private clinical space for the psychologist to meet with patients was a major challenge in the day to day running of the service. This should be a priority for any future proposals to provide psychological support in a medical environment. Careful consideration is required of the IT systems used by the organisations involved in the service. Access to electronic patient records could have been better integrated across trusts. There was a need for highly qualified staff, due to the multiple skill set required to establish the service, work autonomously, and manage the volume and complexity of work. Relationships between services and among board members were primary to success. The lack of enforced hierarchy among those delivering a collaborative service brought energy to the project, as ideas and changes were valued and welcomed from all
Substantial time was taken, on an ongoing basis, to enter the data from paper records completed by patients onto the computer system. This task was primarily taken on by honorary research assistants. Future proposals are advised to take this into consideration at the recruitment stage of service planning.
Evaluating the economic impact of the innovation was not a primary aim of the project. This was challenging to measure in an early intervention service whose aim was prevention and rapid identification of treatment needs, and where no comparison group was available to compare medium or long term outcomes between those who had received psychological input and those who had not.
Qualitative feedback from the medical team and patients consistently reported that the psychology service had positively benefited medical and psychological recovery, and that they anticipated this would have been slower, or even severely disrupted, in the absence of psychological input.
There is substantial research evidence that indicates those with long term physical health conditions also have mental health problems, which was corroborated by our clinical experience. A significant minority of oral and maxillofacial trauma patients come within this category, eg those with brain injury, chronic pain, ongoing need for reconstructive surgery (sometimes for a number of years), disability due to sight loss, or other functional loss and permanent disfigurement. A recent report by the King's Fund and Centre for Mental Health concluded the following, all of which are pertinent to the oral and maxillofacial trauma clinic patient cohort and our innovation:10
– By interacting with and exacerbating physical illness, comorbid mental health problems raise total healthcare costs by at least 45% for each patient with a long term condition and comorbid mental health problem(s), after controlling for severity of physical illness
– There is evidence that the relationship between having multiple long-term conditions and experiencing psychological distress is exacerbated by socioeconomic deprivation.
– A significant part of the explanation for poorer clinical outcomes is that comorbid mental health problems can reduce a person's ability to actively manage their physical health conditions
– Detection of comorbid mental health problems in those with long term health conditions is not done to a consistently high standard, and often goes undetected
– Innovative forms of collaborative care, as modeled within this project, demonstrate that providing support for comorbid mental health needs can reduce physical health costs in acute hospitals. Integrated treatment for mental and physical health has better outcomes than overlaying mental health interventions on top of medical treatment
– Clinical commissioning groups should prioritise integrating mental and physical health care more closely, as a key part of their strategies to improve quality and productivity in health care.
Conclusion
This project in the Centre for Oral and Maxillofacial Surgery at the Royal London Hospital screened almost 650 patients for common mental health conditions, during a one year psychology pilot service. The psychological morbidity found in patients was consistently high, with nearly 80% of patients experiencing at least one psychological condition following suffering a facial injury.
The pilot service was successful in facilitating patients in engaging with appropriate psychological services, ranging from self help resources to specialist psychological therapy and community mental health support. The pilot study has been recognised as an example of excellent innovation for improved patient care, particularly as it covers the arenas of both mental and physical health.
Acknowledgments
Naomi Wilson, Simon Holmes, Christopher Bridle, Katy Price, Sarah Heke, Melissa Pinto, Stewart Hird, Amelia Davies, Romena Toki.
Footnotes
Declaration of interests Nothing to declare.
Ethical approval According to the policy activities that constitute research at the Health Research Authority, the body that oversees research within the NHS, this work met criteria for service development and is exempt from ethics review.