Article Text

Abstract
Physical health monitoring is an integral part of caring for patients with mental health problems. It is proven that serious physical health problems are more common among patients with severe mental health illness (SMI), this monitoring can be challenging and there is a need for improvement.
The project aimed at improving the physical health monitoring among patients with SMI who are receiving antipsychotic medications. The improvement process focused on ensuring there is a good communication with general practitioners (GPs) as well as patient's education and education of care home staff. GP letters requesting physical health monitoring were updated; care home staff and patients were given more information about the value of regular physical health monitoring. There was an improvement in patients' engagement with the monitoring and the monitoring done by GPs was more adherent to local and national guidelines and was communicated with the mental health service.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
The aim of this project was to improve the physical health monitoring for patients with severe mental health illness (SMI) who are on antipsychotic medications. The patients group was under the care of Haringey Community Rehabilitation team (HCRT), they had a diagnosis of schizophrenia and were receiving antipsychotic medications for more than 12 months. HCRT is a multidisciplinary care coordination team that includes: mental health nurses, social workers, psychiatrists, psychologists, and mental health care assistants. The team supports patients with SMI in the community and all patients are residents in care homes. The care homes provide support for the patients with their daily needs, daily activities, and physical and mental health. The care home staff predominantly consists of key workers and managers who have mental health knowledge. HCRT provided care for 167 patients at the time of the project. The patients receiving clozapine and also those who were receiving long acting antipsychotic depot injections in the outpatient clinic were excluded. This was because physical health monitoring was carried out in the outpatient clinic. The patient group included (95 patients) the patients who were receiving oral antipsychotic medications as well as patients receiving long acting antipsychotic depot injections either by the GP or the care coordinator in the community.
Care Program Approach (CPA) review meeting and its preparation were identified as the best opportunity to monitor physical health. CPA review meeting is held every six months to one year for each patient. It is attended by the patient, his/her carers, and all professionals involved in the care. The meeting takes a holistic approach in discussing the care plan and making future plans. Prior to the meeting GPs are invited to update the mental health teams with physical health state, any issues that had risen as well as the most recent review of physical health as per national and local guidelines. A letter is usually sent to the GP requesting this information and inviting the GP to attend, yet GP rarely managed to attend and hence the importance of the GP response to the letter. GPs inviting the patients to have annual physical monitoring will ensure that the patients and their carers are engaging with this process. This in turn will ensure better monitoring. The response rate and quality of the response from GPs reflect both the quality of monitoring, degree of patients' engagement, and communication between GPs and secondary mental health service. The aim was to raise response rate of GP letters to at least 89-90% in CPAs review meeting held between 14 November 2014 and 31 January 2015.The aim was also to ensure that the monitoring is adherent to local and national guidelines.
Background
Evidence confirms that risk of common physical health illnesses is higher among people with severe mental illness as compared to the general population.1 Antipsychotic medications increase physical health risks2–11 as serious as sudden death12 ,13 and stroke.14 De Hart et al in 2011 concluded that the lifespan of people with severe mental illness (SMI) is shorter compared to the general population. The study believed that the excess mortality is mainly due to physical illness. It reported other factors contributing to the poor physical health among this group of patients. The main contributing factors were individual lifestyle choices, side effects of psychotropic treatment, and disparities in health care access, utilization, and provision.15 The mounting evidence of the risks makes regular physical health monitoring of great importance for early detection and management of any problem.
The National Institute for Health and Care Excellence (NICE) guidelines recommend annual physical health monitoring for patients on antipsychotic medications;16 weight, waist circumference, pulse and blood pressure, fasting blood glucose, HbA1c and blood lipid levels. In addition to the above, Maudsley Guidelines17 recommend annual Liver Function tests, Urea and Electrolytes, Full Blood Count, Prolactin. In 2014 NICE guidelines were updated to regulate the responsibility of monitoring the physical health of people with psychosis or schizophrenia. The physical health monitoring is the responsibility of the secondary care team for the first 12 months or till the patient is stable, after that the responsibility is shared with the primary care service.18 Physical health monitoring for patients with chronic enduring mental health problem although of utmost importance can be quite challenging. The pilot of the National Audit of Schizophrenia in 2012 showed that monitoring of physical health parameters was significantly below expectations.19
Baseline measurement
The measurements which were collected continuously throughout the project were percentage of patients who had physical health monitoring completed and documented as well as percentage of GP letter response rate. A baseline audit was designed to assess level of physical health monitoring for patients under the care of HCRT against local and national guidelines. The patients who were receiving oral antipsychotic medications as well as patients receiving long acting antipsychotic depot injections either by the GP or the care coordinator in the community were chosen as the patient group for the project. The group of patients that met these criteria included 95 patients. The rest of the patients under the care of HCRT were excluded as they received the physical health monitoring in the mental health community team outpatient clinic where the process is slightly different. The physical health monitoring for the excluded group was not the primary responsibility of the GP. Also the physical health monitoring done in the community mental health team outpatient clinic was more regularly audited with more satisfactory results. It was felt that a separate project could be designed to examine the physical health monitoring process in the mental health outpatient clinic.
Medical notes and GP letters response from October 2013 to October 2014 were reviewed for the 95 patients included in the project. Local blood results database was also reviewed for blood result. All 95 patients had a diagnosis of schizophrenia, were residents in care homes, and were receiving antipsychotic medications for more than 12 months. The GPs were responsible for carrying out the physical health monitoring for all 95 patients. 52.6% of patients (50 patients) had some blood workup; Liver Function tests 34% (32 patients), Urea and Electrolytes 47% (45 patients), Full Blood Count 50% (48 patients), fasting blood glucose 42% (40 patients), and blood lipid levels 25% (24 patients), done by the GP yet no record of the results was found in the notes. HbA1c (19%- 18 patients) and prolactin levels (4%-4 patients) were rarely done. 10% of patients had their blood pressure measured and documented in the GP letter response. None had their pulse or weight measured. In the patients' notes blood pressure or pulse were mentioned as part of the discussions if the patients were hypertensive or had abnormal pulse. No record of waist circumference, BMI or weight yet the weight was mentioned as part of the discussions with the patients in most records. This showed poor adherence to physical monitoring as per national and local guidelines.
The format for the CPA GP letter was studied; it requested date of last attendance to the GP surgery, date of last physical check-up, if there were any physical problems, the GP's opinion regarding the patient's mental health, whether the patient was on the SMI list, if the patient was on psychotropic medications and if they were compliant with their medications. The format collected data, which did not fully cover the required monitoring guidelines. The response rate for this format was audited for two weeks. The response rate was 10% (1 out of 10 CPA reviews).
HCRT was caring for patients residing in eight different care homes at the time of the project. No physical health monitoring was being done in any of them. Five care homes were approached and they all had access to a blood pressure and pulse measuring machines as well as scales to measure the patients' weights.
Design
The baseline data was studied and discussed in team meetings with all team members. After thorough team discussions and brainstorming; the team agreed that an improvement in the process of monitoring was needed.
The list of improvement strategies included:
-Revised GP letter format.
-Using CPA meetings and the new letter format as a reminder.
-Patients and health professionals education.
The new format for GP letters was needed to ensure physical monitoring as per guidelines was performed. This would serve as a reminder for GPs and patients since the patients are copied into the letter. Then providing education and support to the patients and care home staff would improve the patients' engagement with the physical health monitoring. Eventually the GP communicating the results of this monitoring with the mental health service would reflect the success of this process as well as the quality of communication between primary and secondary health services. It was also agreed that basic monitoring (Blood pressure, pulse, and weight) could be performed in the care homes by care home staff.
The team agreed to work towards improving the response rate for the letters sent to GPs before the patients' CPA review meetings to 89-90%, improve the percentage of patients who have physical health monitoring done before the CPA review meeting to 100%, and engage 25% of care homes in basic physical monitoring by the end of January 2015. It was agreed upon that aiming at an improvement of 100% for the GP letter response was not realistic considering the limited time (10 weeks) and complexity of the process. Therefore, a step approach was implemented since the process involved multiple parties and change in people's attitude towards the importance of physical health monitoring.
Strategy
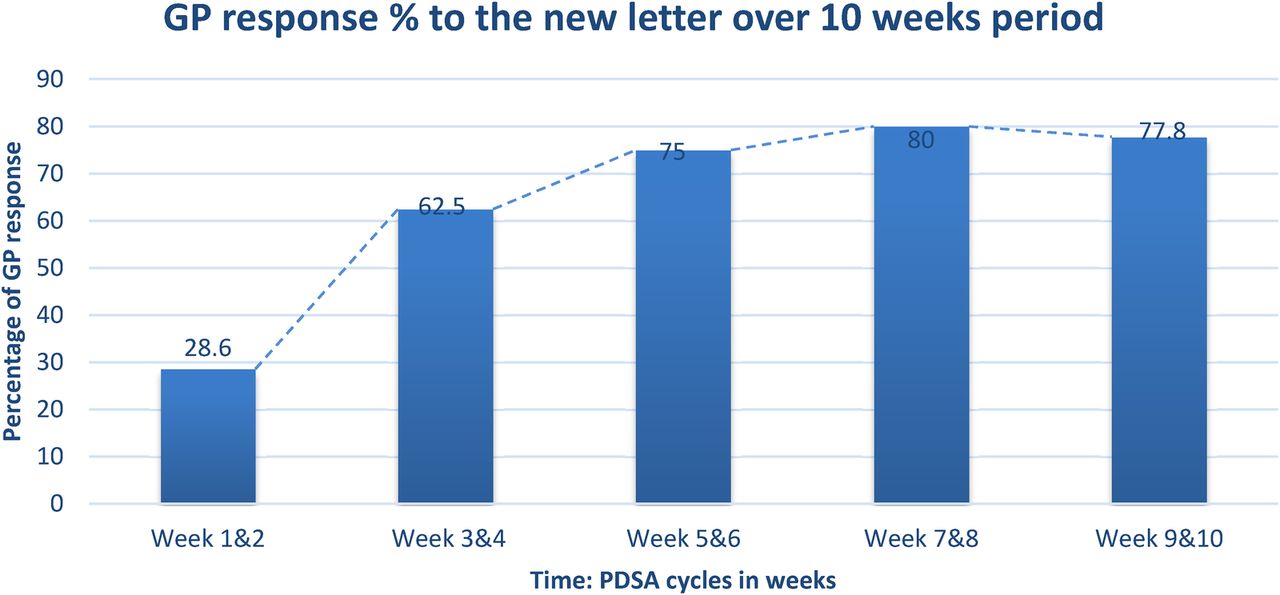
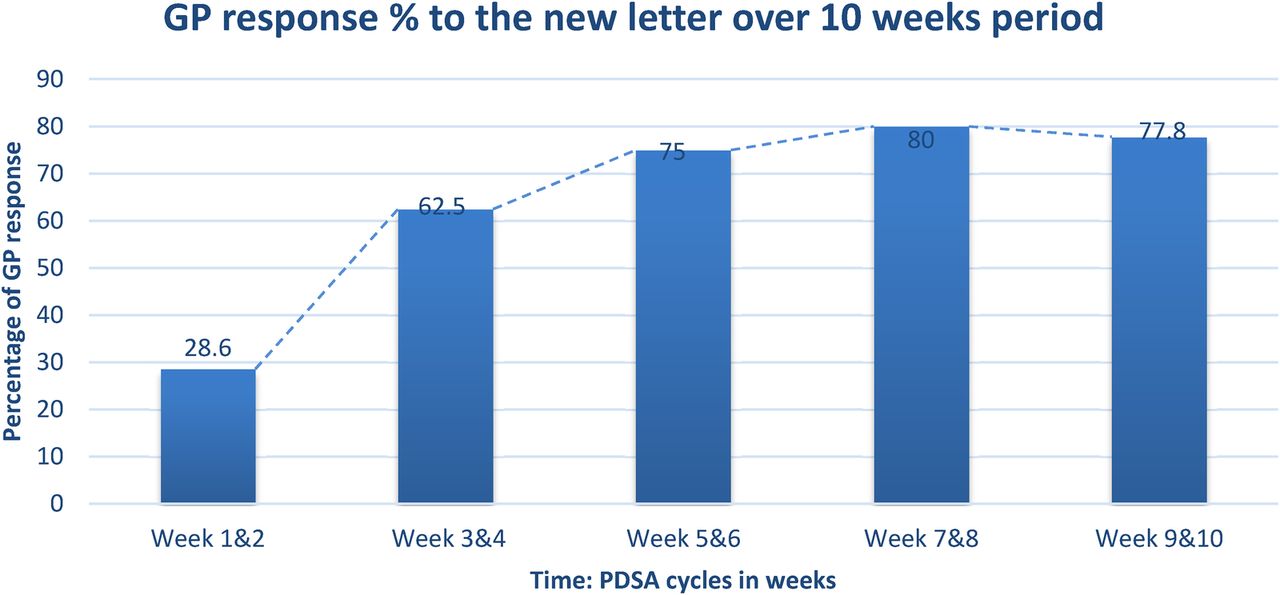
PDSA Cycle 1 (Weeks 1-2) – The new format for the GP letters before CPA review meetings was used and a feedback form was sent along. The feedback form was to assess satisfaction with the new format and encourage suggestions for improvement. The GP letter response rate was 28.6%. (Two responses for seven CPA review meetings). The completed GP response letters were reviewed and analysed (See table 1 below for detailed data).
The percentage of documented monitoring over the 10 weeks period
Local blood results database was reviewed for blood results. Urea & Electrolytes, Full Blood Count, and fasting blood glucose for all seven patients. Liver Function tests for six patients. HbA1c for four patients. Blood lipid levels for only one patient. Prolactin was not done for any of the seven patients (see table 2 below).
The percentage of patients who had bloods done (including the ones not documented)
The importance of physical health monitoring was discussed with two care home managers. One care home managed to measure blood pressure, pulse, and weight for the residents who were under the care of HCRT.
PDSA Cycle 2 (Weeks 3-4) – When the GP practices were called, it was found that sometimes those letters were missed or not among the priority letters. It was decided to call the GP practices after sending the letters to confirm receipt and stress the importance of the reply. The GP letter response rate was 62.5% (five responses for eight CPA review meetings). The completed GP response letters were reviewed and analysed (see table 1 below for detailed data).
Local blood results database was reviewed for blood results. Urea & Electrolytes, Full Blood Count, HbA1c and fasting blood glucose, and Liver Function for all eight patients. Blood lipid levels for five patients. Prolactin was done for two patients (see table 2 below).
Two more care homes were approached, one of them managed to perform the agreed basic monitoring.
PDSA Cycle 3 (Weeks 5-6) – Copies of the NICE and Maudsley guidelines were attached to the letter. The GP letter response rate was 75% (three responses for four CPA review meetings).The completed GP response letters were reviewed and analysed (see table 1 below for detailed data).
Local blood results database was reviewed for blood results. Urea & Electrolytes, Full Blood Count, HbA1c and fasting blood glucose, and Liver Function tests for all four patients. Blood lipid level for three patients. Prolactin level was done for one patient (see Table 2 below).
PDSA Cycle 4 (Weeks 7-8) – The importance of physical health monitoring was discussed with patients in service users' forum in one of the care homes. The aim of this intervention was to encourage the service users to engage with the process of physical health monitoring, attending their GP practices to have the monitoring done. This intervention was not only targeted at patients who had upcoming CPA reviews. It was difficult to keep different service users' engaged due to different levels of engagement, service users' felt other topics were higher on their priority lists and different mental health states among service users attending the meeting. The GP letter response rate was 80% (four responses for five CPA review meetings). The completed GP response letters were reviewed and analysed (see table 1 below for detailed data).
Local blood results database was reviewed for blood results. Urea & Electrolytes, Full Blood Count, and fasting blood glucose and Liver Function tests for all five patients. HbA1c for four patients. Blood lipid level for three patients. Prolactin level was done for two patients (see Table 2 below).
One care home was approached. It managed to perform the agreed basic monitoring.
PDSA Cycle 5 (Weeks 9-10) – CPA meetings and other individual meetings with patients were utilized to discuss physical health needs and the importance of monitoring symptoms. This was perceived to be more personalized and encouraged active patients' engagement with their physical health monitoring and planning. This intervention was a modification of the intervention we tried in PDSA cycle 4. We were hoping to get the service users more involved in the process of physical health monitoring, attending their GP practices and in house basic monitoring within the care homes. Similar to PDSA cycle 4, the intervention was not only targeted at patients who had upcoming CPA reviews. The GP letter response rate was 77.8% (seven responses for nine CPA review meetings). The completed GP response letters were reviewed and analysed (See table 1 below for detailed data).
Local blood results database was reviewed for blood results. Urea & Electrolytes, Full Blood Count and fasting blood glucose, HbA1c and Liver Function tests for eight patients. Blood lipid level for six patients. Prolactin level was done for five patients (see table 2).
In PDSA cycles 4 and 5, it was decided to approach a wide scale of patients; seizing all chances to engage patients with physical health monitoring regardless of the date scheduled for their CPA. This would give time for reinforcing our message more to change the attitudes and opinions of service users towards the importance of the physical health monitoring, as well as achieving the long term improvement of mortality and morbidity. (See supplementary file “Revised GP letter format”)
Results
Between 14 November 2014 and 31 January 2015, 33 patients had CPA review meetings. GP letters were not sent for two of the CPA review meetings. For the 31 CPA letters that were sent out, 21 replies were received with 67.7% response rate. Blood pressure and weight were measured in 68% of patients compared to 10% and 0 respectively in the baseline measurement. 55% of patients had their pulse measured compared to 0 in the baseline measurement. 68% had their bloods done and documented in the GP reply letters compared to 0 in the baseline measurement. Local blood results database showed that 97% (32 patients) had bloods done compared to 52.6% in the baseline measurement; Liver Function tests 94% (31 patients), Urea and Electrolytes 94% (31 patients), Full Blood Count 97% (32 patients), fasting blood glucose 97% (32 patients), HbA1c 85% (28 patients), blood lipid levels 55% (18 patients), and prolactin levels 30% (10 patients). Reviewing the local blood results database showed improvement in physical health monitoring in terms of investigations as well as the need for more efforts to improve communication with GPs. This was because some physical health monitoring was done yet not communicated by the GP and hence was not documented. The feedback questionnaire was completed by 17 GPs; 15 rated it 6 or more out of 10 on a Likert scale of 1 to 10 (1 is poor and 10 is very good). Three care homes managed to measure vital observations and weight for residents under the care of HCRT. Those care homes also agreed to send repeat this basic monitoring regularly. For each care home a care coordinator was identified as responsible for approaching this care home regularly for physical health monitoring.
There was some improvement in physical health monitoring; our project managed to encouraged more patients and GP practices to engage with physical health monitoring. This monitoring was done in accordance with the national monitoring guidelines. Long term improvement in morbidity and mortality among this group of patients can be achieved if more efforts were made to achieve further progress and maintain the progress already achieved. Engaging care homes in basic physical health monitoring (Blood pressure, pulse, and weight) is a step in a long journey towards engaging the care homes in basic physical health monitoring and establishing a culture in care homes by which physical health care is closely integrated in the care of patients with mental health problems.⇓
{kind=link}
Lessons and limitations
The duration of the project was limited to 10 weeks. The positive health outcomes for physical health monitoring among this group of patients are long term ones. Physical monitoring helps early detection of physical health problems which in turn improves morbidity and mortality. Throughout the time we worked on this project, team discussions and getting stakeholders involved proved to be invaluable. These discussions helped to develop the suggested changes and enriched the spirit of ownership among team members, patients, and care home staff. This sense of ownership is important to sustain the change developed and even pave the road to future changes. We learnt how difficult it is to make a change yet small changes help set the scene and create a culture open for bigger future changes. We learnt that more efforts are needed to improve communication with GP practices. We appreciated that GP practices can be quite busy and adding a form to fill in can be challenging. We also had to consider our team's workload to fit in extra duties to maintain the GP practices and care homes engagement.
The process involved multiple parties; patients, carers, care home staff, care coordinators, GPs, and administration staff at GP practices. The improvement plan was difficult and the team had to make an effort to maintain the clarity of vision. We tried to simplify the process in order to start the improvement and then take a step approach towards more achievements. Some interventions were considered but it was decided not to use them to avoid over complicating the process. Some of those interventions were, visiting GP practices to discuss the process, making some basic measurement equipment available for HCRT and train the members to use them. There was some resistance to some changes; chasing GP letter response was a step difficult to allocate, also changing the attitude of patients and the care home staff as well as some of the team members proved to be difficult.
Our intervention was only tested on a small number of patients who had CPAs over a 10 week period. PDSA cycles 3 and 4 showed very small number of CPA reviews. These two cycles corresponded to holiday season when there were long breaks and fewer CPA reviews being held. There is a need to test these interventions on more patients and to collect more data to show sustainability over time.
PDSA cycle 4 and 5 the interventions was not targeted only at patients who had upcoming CPA reviews. The effect of these interventions was not expected to directly affect the results but we predicted that they might improve results in the future.
In PDSA cycles 4 and 5, the interventions did not target only the patient group included in the results. This caused the results of the project to be skewed since the outcomes of the interventions were not completely measured in the limited time of the project. The outcomes were long term because attitudes and opinions take time to change so with more reinforcement more engagement will be achieved, also some patients would not be included in the results since their CPA date was scheduled at times after the termination of the project. We predicted that these interventions would improve the future results.
The team discussed measures to ensure sustainability of the project. Contacting GP practices to follow up the letters sent was the most challenging. It was agreed by the team that this task would be part of the role of the SHO (junior doctor). The team secretary would provide the SHO regularly with a list of patients who had their GP letters sent. It was also planned for the team consultant and SHO to continue approaching care homes to get more care homes involved in the project. The discussion of physical care monitoring with the patients was a responsibility of the team consultant, SHO, and the patients' care coordinators.
Conclusion
The project started to establish a culture within the care homes where staff and patients would actively participate in physical health monitoring. This was achieved by using the GP letters sent to GPs prior to CPA review meeting as a reminder. The letters were meant to ensure physical monitoring was done in accordance with national and local guidelines. Patients' and care home staff were supported to acknowledge the value of physical health monitoring.
Previous efforts have been made to improve physical health monitoring among patients receiving antipsychotic medications. A project by Dr Catherine Rowlands (ST4 psychiatry, SEPT) aimed at improving physical health monitoring among patients receiving long acting antipsychotic depot injections. The interventions developed were aiming at undertaking recommended monitoring yearly in the nurse led outpatient clinic setting, and then signposting/referring to other services as required. A second intervention was to develop a “Health and Wellbeing Booklet” for patients. The project also highlighted the importance of communication of between services and health information . This shows that the process may be slightly different for different services yet the key points for change are similar; education and communication between services.
The changes adopted in the project can be replicated and adapted to different services and teams. The future plan is to continue with the interventions adopted in this project to ensure all care homes, GP practices, and patients under the care of the team are involved. Also there is a plan to replicate the project and extend it to patients under the care of the outpatient clinic.
Acknowledgments
Dr Khaver Bashir, Consultant Psychiatrist, Haringey Community Rehabilitation Team. EQuIP course team in Great Ormond Street Hospital. Haringey Community Rehabilitation team especially Victor Mabena, Richard Carroll and Sue Sharpe.
References
Footnotes
Declaration of interests There is no conflict of interest to declare.
Ethical approval Ethical approval was not required since it was an improvement project to an existing process. It was not a study on human subjects.