Article Text

Abstract
Significant delays occur in providing adequate pain relief for patients who present to the emergency department (ED) with extremity fractures. The median time to pain medication administration for patients presenting to our ED with extremity fractures was 72.5 minutes. We used a multidisciplinary approach to implement three improvement cycles with the goal of reducing the median time to pain medication by 15% over an eight month time period. First, we redesigned nursing triage and treatment processes. Second, we improved nursing documentation standardization to ensure accurate tracking of patients who declined pain medication. Third, through consensus building within our physician group, we implemented a department-wide standard of care to provide early pain relief for extremity fractures. Median time to pain medication for patients with an extremity fracture reduced significantly between the pre-and post-intervention periods (p=0.009). The average monthly median time to medication was 72.5 minutes (95% CI: 57.1 to 88.0) before the intervention (Jan 2013-Oct 2014) and 49.8 minutes (95% CI: 42.7 to 56.9) after the intervention (November 2014 to June 2016). In other words, monthly median time was 31% faster (22.7 minute difference) in the post intervention period. Implementing three key interventions reduced the time to pain medication for patients with extremity injuries. Since June 2016 the reductions in median time to medication have continued to improve.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Providing timely pain relief for patients who present to the emergency department (ED) with extremity fractures is a challenge. Many of these patients arrive by private vehicle and are triaged at a lower level of acuity. Our ED is an academic, tertiary care, level 1 trauma center with approximately 50,000 patient visits per year. Our pediatric and adult patients with extremity fractures were waiting a long time before receiving pain relief. The problem came to our attention through patient complaints, internal observation of wait times, and comparison of our wait times to those in other EDs through the public reporting of this measure by the Centers for Medicare and Medicaid Services (CMS).
Background
In 2012, CMS added as a core measure “median time from ED arrival to time of initial oral, intranasal or parenteral pain medication administration for ED patients with a principal diagnosis of long bone fracture” (OP-21: ED- Median Time to Pain Management for Long Bone Fracture).1
The Joint Commission implemented assessment and management of pain as a quality standard for hospitals in 2001. CMS cited a key study that investigated whether the implementation of that quality standard had improved pain medication wait time for patients presenting with long bone fractures.2 The study demonstrated that, even after implementation of the quality standard, only 76% of patients with long bone fractures received any pain medication during their ED visit.3 ,4
Timeliness of pain relief is a part of timeliness of treatment, one of the Institute of Medicine's six aims to improve quality.5 Furthermore, timeliness and patient-centeredness are key components of improving patient experience, one arm of the Triple Aim advanced by the Institute for Healthcare Improvement.6
Baseline measurement
We analyzed the ED time to pain medication administration in accordance with the CMS core measure for both adult and pediatric patients. As part of the core measure, for patients with a diagnosis of long bone fracture, we collected time of arrival of patient to the ED and the time the patient received any analgesic medications. Our hospital's core measure abstractor collected and reported this data as part of the hospital reporting requirement for CMS. Baseline data had already been collected due to this reporting requirement. We chose to use this data because it was available and will continue to be collected by our hospital's quality department. The median time to pain medication administration for patients presenting to our ED with extremity fractures was 72.5 minutes.
Design
We established reducing wait time to pain medication for patients with traumatic extremity injuries as one of our quality goals for the year. We discussed root causes and key elements for change in our monthly ED continuous quality improvement committee meetings. The cause and effect diagram in Figure 1 outlines our initial discussion of root causes to our problem that informed our first two improvement cycles. Nursing and physician management and ED staff participated in these meetings. Our team consisted of the adult ED nurse manager, pediatric ED nurse manager, ED assistant nurse manager, two staff nurses, ED clinical director, ED quality director, two administrative staff members and the manager of ED registration. The committee mapped the current and desired future state, set a goal of 15% reduction in time, and identified key stakeholders.
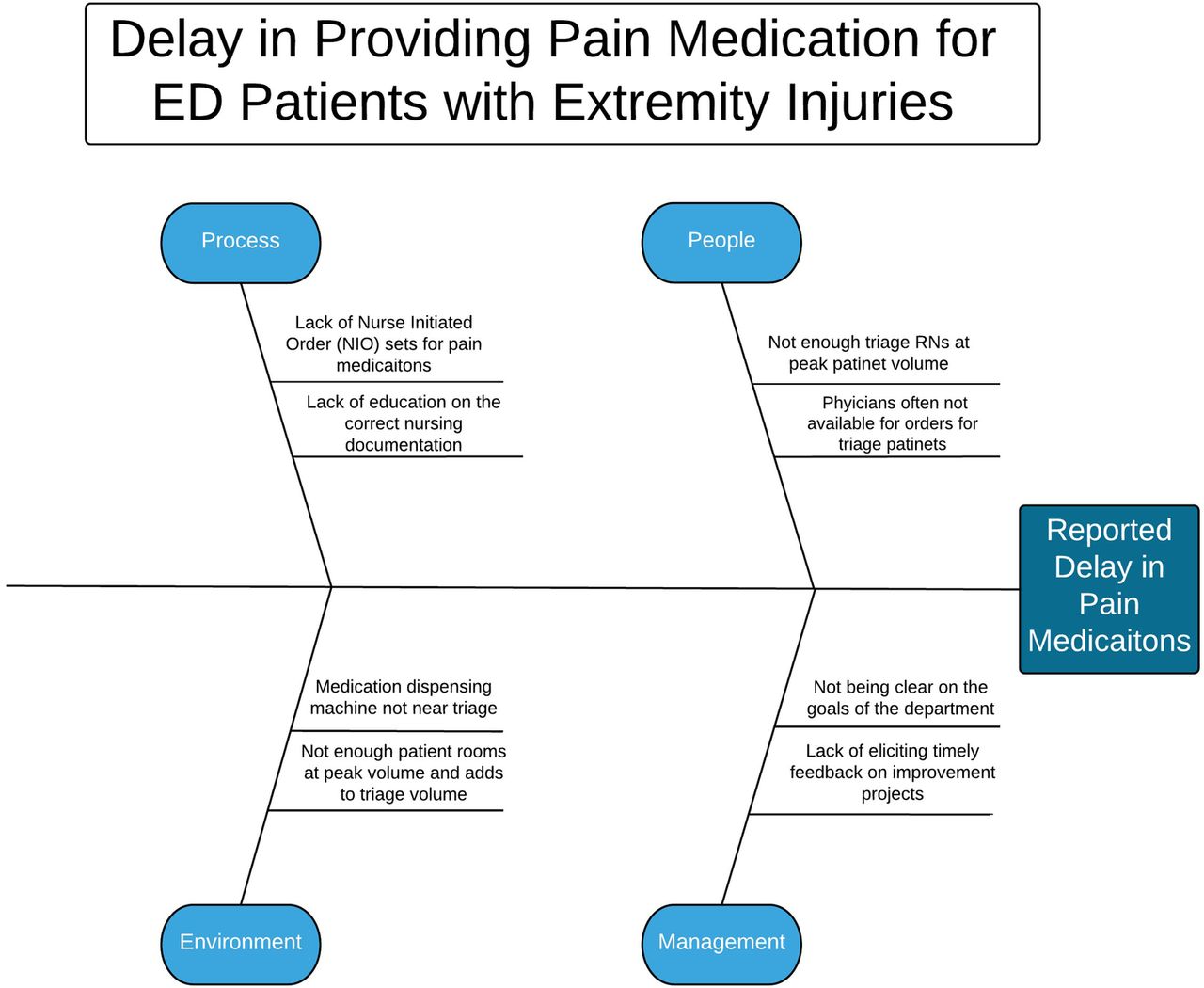
Cause & Effect Diagram for Delay in Pain Medications
Strategy
Improvement cycle 1 (November, 2014): Our aim for this cycle was to allow better access for nursing staff to order and administer analgesic medication to patients with extremity injuries. The change hypothesis reasoned that if nurses did not have to communicate with providers in real time about analgesic medication the patients would receive this medication with less delay. We amended the pre-existing Nurse Initiated Orders (NIO) protocol to (1) direct the triaging nurse to always offer pain medications to patients presenting with likely fractures and (2) enable the triage nurse to order acetaminophen or ibuprofen for adult and pediatric patients. We elicited feedback from ED triage nurses on a weekly basis to collect qualitative data and also continued to collect and review data from the quality department on a monthly basis. We learned that by amending the NIO protocol and educating staff nurses on this protocol helped to reduce time to pain medication administration for our patients. However, we also identified nurse documentation as being another opportunity through eliciting weekly feedback on this improvement cycle.
Improvement cycle 2 (December, 2014): Our aim was to improve documentation to better reflect what we were actually doing in the ED. Our change hypothesis was we were offering analgesic medication to patients, but not correctly documenting when we did or when the patient declined the medication. The first improvement cycle revealed inconsistency and errors of omission in nursing documentation. We reviewed several patient charts with the hospital core measure abstractor to identify opportunities for improvement. We discovered that nursing staff were not routinely documenting patient refusal of pain medication, which should have removed this population of patients from the denominator of the core measure. As a result, the average pain medication wait time was artificially inflated. We standardized documentation of pain medication refusal to address this issue and developed standard work. Nurses were trained on the standardized documentation through daily readiness huddles, monthly triage meeting, monthly ED nursing meetings and by email. A job aid was developed and posted in the triage area. We elicited feedback from ED nurses on a weekly basis to collect qualitative data and continued to collect and review data from the quality department on a monthly basis. From the first two improvement cycles, a cultural belief was identified that some nursing staff felt they could not provide oral pain medications to patients in the event the patient required sedation for fracture reduction and therefore needed to be nil per os.
Improvement cycle 3 (January, 2015): On our final improvement cycle we aimed to build provider consensus on the use of oral medication for patients that may need a procedural sedation during their ED visit. The change hypothesis was that by building a departmental best practice agreement in the physician group there would no longer be mixed practice patterns by individual providers in our ED regarding the safety to perform a procedural sedation after a patient received oral medications. This in turn would remove any nursing barriers or hesitation for providing oral analgesics. The ED quality medical director sent an email survey to eight faculty members to assess their clinical recommendations on this issue. The ED physician leadership and senior faculty members all agreed that nurses could safely provide oral pain medication at triage, on the grounds that risk of aspiration with procedural sedation after consuming a small amount of water and pain medication was minimal. We then educated providers and nurses using this new standard of care. We communicated the physician group decision through email and at faculty meetings. In January 2015, we finalized the standard work and job aids for nursing. Through consensus building within our physician group, we implemented a department-wide standard of care to provide early pain relief for extremity fractures.
An important management strategy that we applied during this project was weekly stand-up meetings in our adult and pediatric emergency departments. The weekly stand-up meetings started September 2014, two months before we implemented our first improvement cycle. Our emergency department operations leadership was struggling with how to move departmental quality goals forward on a consistent basis. Equipment, staffing, and process problems were also not being resolved in a timely fashion. The quality director of the ED initiated the weekly meetings and initially led the weekly meetings to gain support from the rest of the team. Members of the team include physicians, nurses, registration, social workers and administrative support staff. Rounds occur at 7:30am, every Tuesday, and last 20 minutes. We use a standard presentation format and team members have assigned roles in advance. The assigned leader guides the discussion and the scribe documents progress on the project tracker. We use a standard process by having the team leader use a prompting card each week to review one quality project by using the PSDA methodology. The card asks 5 questions that prompt the group to discuss the last PDSA cycle process in a clear and direct fashion. We have measured the success of the stand-up meetings by consistent attendance during the past two year period, completion of 152 “quick hits” (equipment, staffing, and process issues) and the successful outcomes of several more complicated process improvements including this project. Challenges have included developing processes to update our data weekly for our quality project metrics, making sustained progress on departmental goals that involve services outside our emergency department, and engaging staff physicians and nurses in the quality rounding process.
Results
Median time to pain medication for patients with an extremity fracture was significantly different between the pre-and post-intervention periods (p=0.009). The average monthly median time to medication was 72.5 minutes (95% CI: 57.1 to 88.0) before the intervention (Jan 2013-Oct 2014) and 49.8 minutes (95% CI: 42.7 to 56.9) after the intervention (November 2014 to June 2016). Expressed in a different way, monthly median time to medication reduced by 22.7 minutes (95% CI: 6.1 to 39.4) in the post intervention period.
A limitation of our data is that we reviewed a relatively low number of patient charts that met criteria each month. On average 10 patient charts were reviewed each month that met criteria for this core measure. The relatively low number of patient charts reviewed each month contributed to the variability in the data from month to month.
The ED continuous quality improvement committee set a goal to reduce time to pain medication administration by 15% by June 30, 2015. We implemented the first improvement cycle in November 2014 and the second improvement cycle in December 2014. We executed the third and final improvement cycle in January 2015. Figure 2 is a run chart with the improvement cycles identified to describe the temporal relationship between improvement cycles and median time to medication administration. After conducting the first improvement cycle, median time decreased from 67 minutes in November to 47 minutes in December. June 30, 2015 concluded with a year-to-date median time of 48.5 minutes. This change has been sustained through June 2016.

{kind=link}
{kind=link}
Run chart of monthly median time for administration of pain medication for ED patients diagnosed with long bone fractures.
Through consecutive rapid improvement cycles, we were able to meet our stated goal by the proposed deadline. Figure 2 demonstrates that over time the interventions implemented have continued to reduce time to pain medication administration for ED patients, even after the conclusion of the initial study period. Processes and interventions such as these serve to optimize the patient experience, a key component of the Triple Aim. Through continued efforts to improve timeliness of pain medication administration and, in turn, expedite pain relief, we are striving to optimize patient experience, one of the key components of the Triple Aim of health care.
Lessons and limitations
Lessons Learned
An unexpected but significant barrier that prevented nurses from providing pain medication in triage was the perception that patients should not be given oral medication. During daily nursing huddle meetings and in the ED triage meeting, it emerged that many nurses believed that administration of oral pain medications would render patients ineligible for surgery or procedural sedation. This perhaps should have been anticipated, as it is general practice to require patients to abstain from consuming food or drink for a prolonged period prior to procedures requiring sedation. We resolved this concern by obtaining a clinical policy statement from ED physician group, which we disseminated in the ED triage meeting and reinforced in daily nursing huddles.
We also spent time with our hospital quality department and specifically the CMS core measure abstractor at our hospital to better understand how to clearly document that we provided pain medication or the patient declined to have pain medication after we offered it. Improved documentation contributed to a more accurate reflection of our practice and improved our reported times to providing pain medications.
The implementation of the weekly stand-up quality meetings created a cadence of reviewing our progress and this most likely contributed to our success in improving as a department on this project. Having ED leadership presence every week at the stand-up meetings helped to hold other members, and the ED leadership team, accountable to making progress on the quality goal. These meetings helped to keep our group action focused by making progress each week on the to dos associated with each quality project. As a multidisciplinary group the identification of the barriers for why items are not being completed is important. It was in this setting that we first identified that the nursing-physician cultural barrier was a significant barrier to not providing oral pain medications to patients in the triage area of the ED.
Limitations
We conducted our intervention at a single academic ED; the culture among providers, patient population, and barriers to change may be different in other settings and may limit the effectiveness of the particular interventions here employed. Our data is affected by some variability due to low number of patient charts being reviewed each month. This study was not blinded or randomized and could be subject to bias. Since we used improvement cycles that adapted to opportunities of the changing local circumstances, rather than a Plan-Do-Study-Act (PDSA) cycle approach, it is difficult to determine which of the three improvement cycles were responsible for the changes and how much each improvement cycle influenced the results.
Conclusion
By implementing three key improvement cycles, we reduced our time to pain medication for patients with extremity injuries by 31%. The effects of the interventions have persisted after we completed the final intervention. Our experience may be instructive for Emergency Departments seeking to reduce time to administration of analgesics in patients with long bone fractures. We plan to continue to monitor our data and reinforce standard work to continue to sustain the improvement we achieved.
Acknowledgments
Denise Langley, Janie Johnson, Starr Edge, Alan Lines, Chelsea Smart, Karoly McDonald
Footnotes
Declaration of interests Nothing to declare
Ethical approval Our Institutional Review Board reviewed our project and deemed it was an improvement study and not a human subjects study. They provided exemption status and permission to externally publish the results of this improvement process.