Article Text

Abstract
Assessment of mental capacity provides an ethical and legal framework for care which values patients' autonomy whilst recognising the instances where it is appropriate to act in patients' best interests.
Existing medical literature indicates that mental capacity is poorly documented in psychiatric inpatient settings. The aim of the project was to examine the frequency of capacity and consent to treatment documentation with a view to creating changes in practice by raising awareness about the importance of assessing and documenting mental capacity.
A multi-centre quality improvement project was conducted in September 2014 across all general adult psychiatric inpatient wards in the North Central London Training Scheme. The frequency of documentation of capacity and consent to treatment for all adult psychiatric inpatient wards across North Central London was measured.
Electronic patient notes were audited retrospectively to ascertain whether capacity and consent to treatment on admission, and within the preceding seven days of data collection, was recorded. Data was collected across three successive time points during a 12 month period following the implementation of changes. A total of 232 patients were included in the baseline measurements. The results highlighted a deficiency in the recording of capacity and consent to treatment for adult psychiatric inpatients. The results showed that, of the patients audited, 49.8% had their capacity and consent to treatment assessed on admission, 61.9% had a capacity assessment in the previous 7 days and 60.5% had consent recorded in the previous 7 days. These findings were presented at local hospital teaching sessions at each of the audited sites. These sessions also gave teaching on mental capacity. Audit cycle 1 was conducted 6 months later, this included 213 patients and showed a 30% improvement in the frequency of documentation across all measures. The results showed that 77% of patients audited had their capacity and consent assessed on admission to the ward, 87.3% had a capacity assessment in the previous 7 days and 85.5% had consent recorded in the previous 7 days. After feedback from the teaching sessions, a clerking proforma was produced that had a prompt to assess to capacity. Audit cycle 2 was conducted 12 months after the initial baseline measurements, had a sample size of 229 patients and a sustained improvement in documentation of 26% from baseline was demonstrated across all measures.
This project demonstrated that capacity and consent to treatment was not routinely recorded but that the frequency of recording improved through the use of teaching sessions on mental capacity and the introduction of admission clerking proformas with capacity prompts.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Existing medical literature indicate poor levels of capacity documentation amongst psychiatric in-patient settings.1 A recent large retrospective cohort study of psychiatric inpatients found that only 9.8% had a capacity assessment recorded in their notes.1
Due to the nature of mental illness, patients can lack the capacity to make decisions in relation to their treatment, rendering them unable to give informed consent to medication and treatments that they receive. In psychiatric inpatients, the proportion of patients lacking capacity to make treatment decisions ranges between 40-60%.2 ,3 A large cohort study of 350 psychiatric inpatients found that 86% of patients detained under the Mental Health Act (MHA) 1983 lacked capacity and 39% of patients who were not detained (‘informal’ patients) lacked capacity3. However, mental health professionals can also incorrectly assume that unwell patients lack capacity to understand and make decisions about their treatment. This can disempower patients, depriving them of their right to be involved in decisions in their treatment and recovery. The Care Quality Commission (CQC) raised concerns that making false assumptions about a patient's capacity to consent to treatment, could lead to their unlawful detention under the Mental Health Act (MHA) 1983.4 As well as acting as a legal safeguard, the process of assessing capacity generates discussion about management options with patients, thereby giving them the opportunity to be more involved in decisions around their treatment. Furthermore, a patient's capacity to consent to treatment can fluctuate during admission and as their illness is treated, making repeated capacity assessments useful, particularly as capacity is time and decision specific. The CQC guidance and the Mental Health Code of Practice recommend that mental capacity should be regularly assessed during psychiatric admissions.5
This project examined the frequency of capacity and consent to treatment recording in adult psychiatric in-patients across North Central London.
Background
Mental capacity is a key principle when providing care for patients in a mental health setting, and explanatory documentation is valuable for both clinical and medical legal purposes.
The Mental Capacity Act (2005) in England and Wales offers important guidance on the assessment of a patient's mental capacity and informs subsequent management. The Act marked a change in attitudes that recognised the importance of autonomous decision making in patient care.6 Whilst the Mental Capacity Act (MCA) guidance relates to England and Wales, the principles that underlie the rational for a robust system that assesses capacity are universally relevant. The details and procedures of testing capacity vary across these regions but all employ similar central concepts. However, there is a lack of evidence in the medical literature demonstrating the frequency of mental capacity and consent recording worldwide.
Whilst the MCA is concerned with patients that lack capacity, the MHA provides a legal framework for detaining and treating patients suffering from a mental illness, irrespective of whether they have the capacity to consent to treatment. However, the MHA Code of Practice explains that health professionals are still required to determine whether a patient has the capacity to consent to treatment.7
The Mental Capacity Act Deprivation of Liberty Safeguards (DOLS) were included as an addition to the 2005 Mental Capacity Act to give guidance about the specific situations in which it is permissible for people who lack mental capacity to be deprived of their liberty.7 The Supreme Court judgement in March 2014 broadened the definition of deprivation of liberty to encompass anyone who is subject to ‘continuous supervision and control and is not free to leave’.8 Following this ruling it became even more important to assess patients' capacity to consent to hospital admission, particularly for patients that were not admitted under the MHA, to ensure that their admission did not amount to unlawful deprivation of their liberty. The Care Quality Commission (CQC) recommends that capacity to consent to treatment is recorded at the start of every informal psychiatric admission and assessed routinely during admission.9
The documentation of consent and capacity to treatment is monitored by the Care Quality Commission (CQC) across healthcare services. The CQC and The Mental Health Code of Practice recommend that when capacity assessments are recorded, they should include evidence of the discussions that determined the outcome of the assessment.4 ,5 Therefore, clinicians are encouraged to justify the outcome of their assessment and record the thinking processes that led to their decision.
Baseline measurement
Patient notes in the RiO electronic care record system were audited for the recording of capacity and consent to treatment on admission, and over the preceding 7 days prior to data collection in August of 2014.
The keywords searched were ‘capacity’ and ‘consent.’ Patients were excluded from the analysis if they had been admitted to hospital less than 7 days prior to the date of the data collection, or if patients were absent from the ward at the time of the data collection.There were 279 patients in the initial sample population of which 47 were excluded according to the exclusion criteria.
The results revealed that 49.8% of patients audited, had their capacity and consent recorded on the electronic notes on admission to the ward. 61.9% had their capacity recorded in the previous 7 days and 60.5% had consent recorded in previous 7 days.
Design
The aim of this project was to improve the frequency of capacity and consent to treatment recording in psychiatric inpatients. Our aim was to achieve an increase of over 20% across all measures in comparison to the baseline levels, over a 12 month period.
This project was conducted by 4 core psychiatry trainee doctors working across the different hospital sites during the period of the project, and was supervised by a consultant psychiatrist.
During the baseline measurements and each audit cycle electronic patient records were analysed for the recording of capacity and consent to treatment on admission and within the preceding 7 days of data collection. The ‘Progress Note’ and ‘Capacity and Consent’ sections of RiO electronic patient records were audited. The electronic notes were audited for the keywords ‘capacity’ and ‘consent’. Exclusion criteria included patients who were admitted within 7 days of data collection and those that were absent from the ward at the time of data collection.
Meetings with trust managers and senior clinicians were organised to establish the current practices around capacity and consent recording and to determine where improvements could be made. During these consultations it became clear that there was insufficient teaching for clinicians on the clinical standards for the assessment and documentation of capacity and consent.
This topic was not being routinely taught during local induction programmes and consequently there was a lack of awareness among front-line staff such as junior doctors who were new to their trusts. Furthermore, it was felt that clinical pressures of admitting acutely unwell psychiatric patients meant that capacity and consent could be overlooked. Consequently, this project aimed to create new strategies that would improve awareness around the importance of assessing and documenting mental capacity and consent to treatment in psychiatric inpatients.
A series of presentations on capacity and consent recording were given at each of the hospital's local induction programme and local academic meetings. In addition, during this time, a new section was added to the electronic patient record system (RiO) specifically designed to record information about a patient's mental capacity and consent.
Strategy
Audit Cycle 1: Audit cycle 1 occurred over a 6 month period. During this time we planned to implement teaching sessions to educate staff about mental capacity and the results of our baseline measurements. We hoped that by improving understanding of the complexities involved in mental capacity and the degree of the problem identified from our baseline measurements, documentation would improve. The results of the initial baseline measurements were presented at local trust academic sessions, in addition to guidance on the Mental Capacity Act and how to assess patients' capacity to consent to treatment. The new changes to RiO were discussed and clinicians were made aware of the importance of recording the capacity of patients using the new section on RiO. The feedback from the sessions was that whilst a one-off teaching session may temporarily raise awareness amongst existing clinicians, any improvement may be lost with successive rotations of new junior doctors. Therefore, we modified our strategy by requesting that a regular teaching session on capacity and consent be added to the local induction programme for new doctors every 6 months, and we produced a clerking proforma for junior doctors that included a section on mental capacity. This proforma was incorporated into the induction handbook for each junior doctor when they started each rotation. After exclusions, a total of 213 patient records were analysed after the changes made in Audit Cycle 1.
Audit Cycle 2: Audit Cycle 2 occurred over a period of 6 months. During this period we planned to assess the impact of the clerking proforma and the inclusion of capacity and consent teaching in the local induction. We recognised the importance of gaining feedback on the teaching and clerking proforma to ensure that it was useful and succinct. This feedback was gathered through teaching feedback questionnaires that are routinely completed after the teaching sessions. The issue of capacity and consent recording was also discussed at local junior doctors forums held at each hospital site in order to gather feedback from doctors. From the feedback gathered we modified the clerking proforma in order to improve its clarity and we created an online version in order to improve its accessibility for doctors. The results demonstrated a sustained improvement in capacity documentation during this 6 month period. After exclusions, a total of 229 patients were included in the analysis during audit cycle 2.
Results
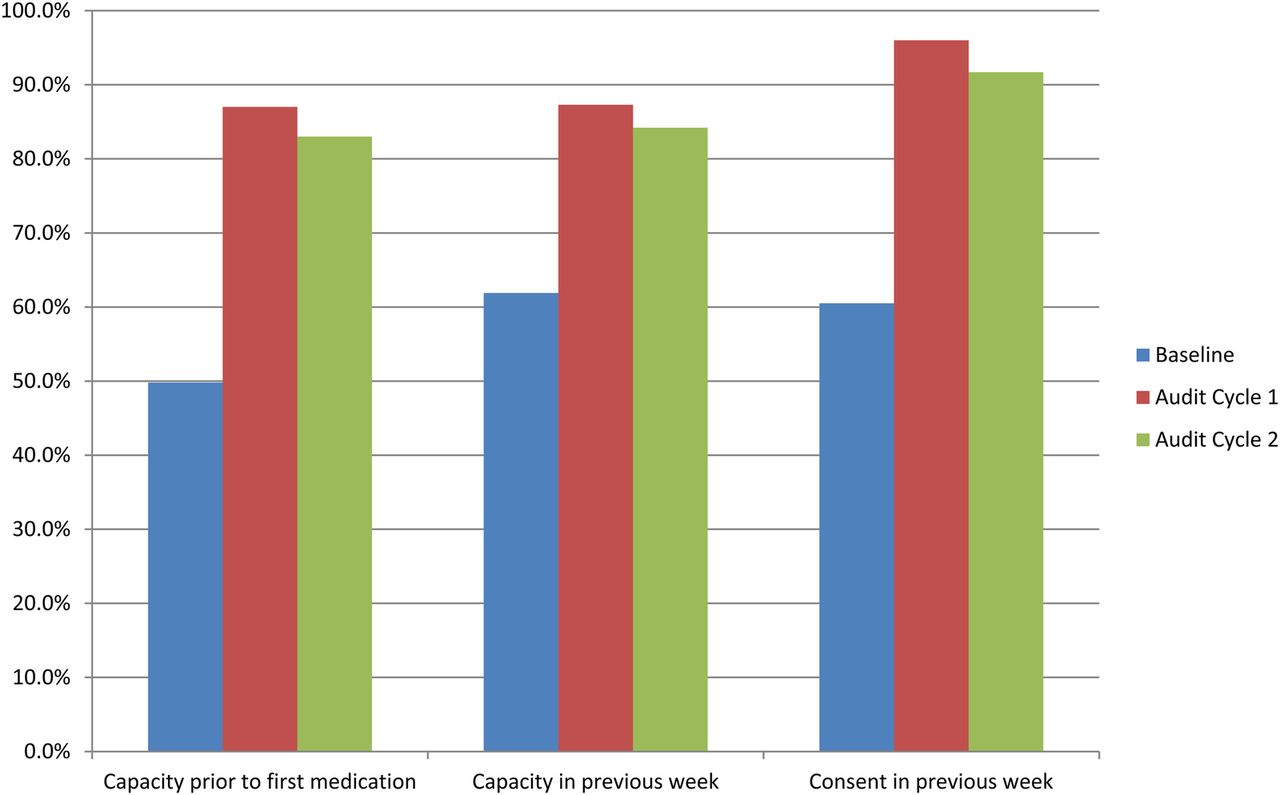
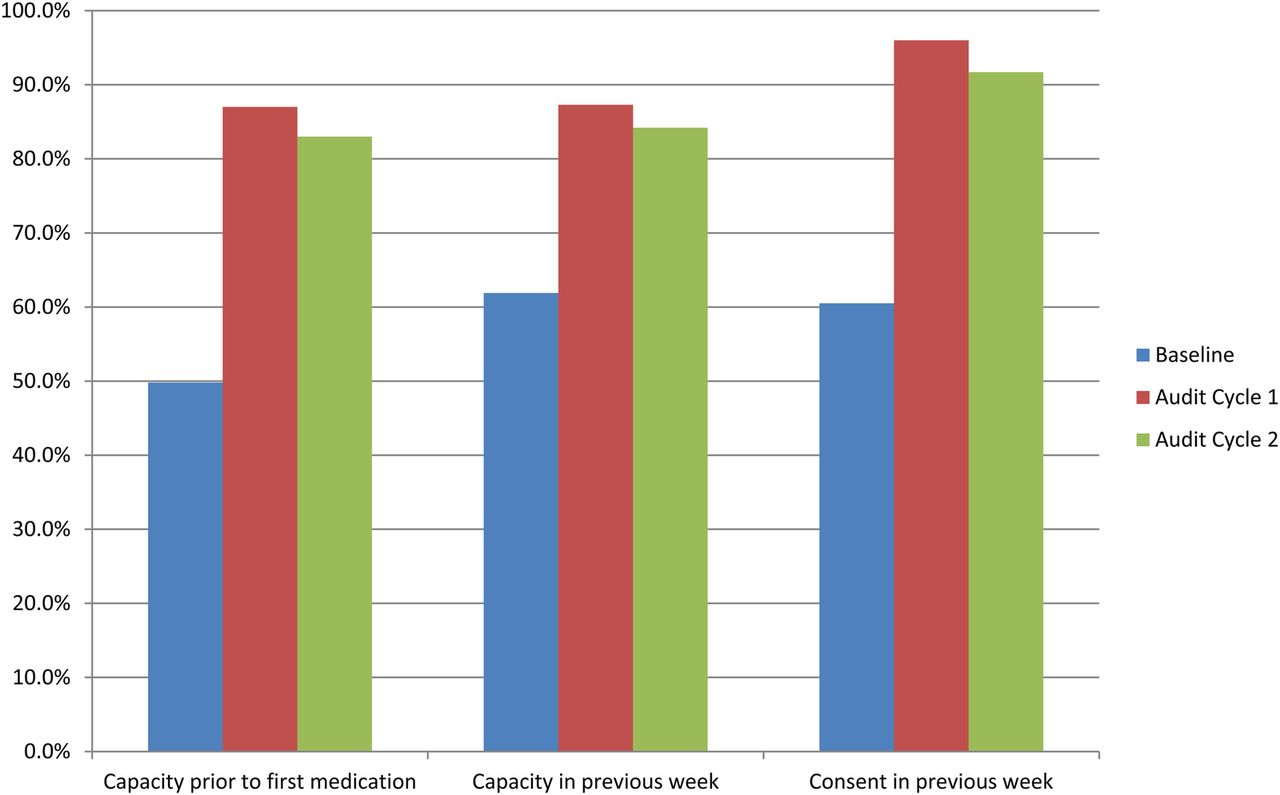
At baseline, a total of 232 electronic patient records were audited for the recording of capacity and consent to treatment on admission and within the preceding 7 days of data collection. The results revealed that 49.8% of patients had their capacity and consent to treatment recorded on the electronic notes on admission to the ward, 61.9% had their capacity recorded in the previous 7 days and 60.5% had consent recorded in the previous 7 days.
The electronic records of 213 patients were analysed during audit cycle 1. After the changes were implemented, the audit demonstrated an improvement of over 30% across all measures. The results showed that 87% of patients had their capacity and consent assessed on admission; 87.3% had capacity assessed within the preceding 7 days and 96% had consent recorded within the preceding 7 days.
During audit cycle 2 a final re-audit was conducted to assess the frequency of recording of capacity and consent in the electronic notes in order to ascertain whether the improvements in documentation seen in audit cycle 1 had been sustained. Audit cycle 2 was conducted 1 month after the new intake of junior doctors and 12 months from the time of the initial data collection. The results of audit cycle 2 demonstrated an improvement of 26% amongst all measures in comparison to the initial baseline measurements. The results showed that 83% of patients audited had their capacity and consent assessed on admission to the ward, 84.2% had capacity assessed in the preceding seven days and 91.7% had consent recorded in the preceding seven days. See figure 1 for a summary of results.
{kind=link}
Summary of Results
Lessons and limitations
This quality improvement project assumed that if capacity and consent to treatment was not recorded in the electronic notes, the assessment did not take place. However, it is possible that capacity and consent to treatment was performed but not documented, or was documented elsewhere. This project searched for capacity assessments by performing a keyword search in the electronic notes for the words ‘capacity’ or ‘consent’. Therefore, it is possible that capacity assessments took place but that alternative terminology was used.
The data was collected over three distinct time periods. The frequency of capacity documentation may have differed if the sample size was larger or the data was collected over a different time period. Whilst the data was collected over 3 cycles across 12 months, and demonstrated some sustained improvement, there was a reduction in capacity and consent recording of 4% between Audit cycle 1 and 2. Whilst this may be a small fluctuation around a sustained level of change, it is also possible that with a longer period of testing there would be a gradual decline in the levels of improvements seen in comparison to the baseline measurements.
Whilst the auditing produced results that indicate and improvement in capacity and consent recording during the time period of the study. Due to the small sample size and the infrequent sampling method across only 3 points, it is also possible that the improvements measured could be as a result of chance.
An improvement to the methodology of the project could be achieved through more frequent data sampling and the use of a larger sample size as our current results could have been due to chance. Another limitation is that there were multiple interventions made during each audit cycle. This meant that we are not able to determine exactly which interventions related to the improvements measured. We could have improved the methodology by testing our each intervention on a small scale prior to utilising them in the audit. This would have been more consistent with the PDSA cycle methodology and may have improved the efficiency of the project in avoiding large scale implementation of strategies that may not be effective.
This project demonstrates that simple measures such as presenting data collection results and producing clerking proformas with prompts, can generate dramatic changes in practice. Another important lesson was recognising the need to ensure that any observe improvements were sustained over time. By introducing a new clerking proforma that was given out at junior doctor induction and regular teaching sessions on capacity and consent, this project was able to demonstrate a persistent improvement over a year after the baseline measurements.
Conclusion
This project highlighted that capacity and consent to treatment in adult psychiatric inpatients was not being routinely recorded. After the introduction of teaching sessions and a clerking proforma with a capacity assessment prompt, the repeat data collections showed an improvement in all measures, and achieved the intial aim of improving all recording measures by at least 20%. This project analysed data from 5 psychiatric hospitals located in two NHS trusts. Therefore, the multi-site design offers some ability to generalise and replicate these results across other inpatient settings in different NHS trusts. There are some limitations to the generalisability of this project, due to differences in local trust protocols and their modality of recording patient information. There are also limitations of the study due to low frequency of measures and limited sample sizes. Our results compare favourably to a recent large retrospective cohort study which showed that capacity assessments were documented in only 9.8% of psychiatric admissions.1
Promoting routine assessment of capacity and consent helps clinicians operate within a legal and ethical framework for their patients, and enhances the collaboration of patient and clinician in decision making. We plan to expand our teaching sessions on mental capacity and to gain further feedback on how the clerking proformas could be improved.
Acknowledgments
We would like to express our gratitude to Dr Jonathan Greensides and all of the ward staff at Dorset Ward in Chase Farm Hospital.
Footnotes
Declaration of interests No conflict of interests.
Ethical approval This project was a retrospective audit of electronic records where all patient information was anonymised. It was therefore exempt from ethical approval.