Article Text

Abstract
Blood tests are a seemingly basic investigation, but are often a vital part of directing patient management. Despite the importance of this everyday process, we indentified the potential for improvement of the current phlebotomy service in our hospital, as both junior doctors and phlebotomists reported a lack of communication and standardised practice across the wards. Resulting delays in obtaining blood test results can impact detrimentally on patient safety and management.
We designed a survey which highlighted inefficient handovers and discrepancies between wards as driving factors behind this. We therefore aimed to improve communication between phlebotomists and doctors, as well as the overall organisation of the service. This took the form of the “Phlebotomy Box,” a box file system offering a set location for blood stickers to be situated. The box concept was optimised on a series of medical and surgical wards, incorporating multidisciplinary feedback from relevant teams. We measured how many untaken bloods were handed over to medical staff continuously, both pre- and post implementation of the phlebotomy box.
Our baseline ward demonstrated poor handover rates of untaken bloods, ranging from 0% to 40%. This increased to a consistent 100% following introduction of the Phlebotomy Box and ongoing staff education. Once optimised, the box was trialled on a further two medical wards and one surgical ward, achieving 100% handover from an initial 0% to 67%. Quantitative improvement was also reflected qualitatively in widespread staff surveys, with overwhelmingly positive support and acceptance.
In summary, the Phlebotomy Box innovation has led to 100% of untaken bloods being effectively handed over. We have demonstrated a significant improvement in communication and efficiency within the phlebotomy service, with tangible benefits to patient care, as minimising time lags can prevent delays in clinical decisions. The phlebotomy box represents a simplistic, sustainable intervention that could be easily replicated in other Trusts.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Blood tests are a seemingly basic investigation, but are often a vital part of directing patient management. The inpatient phlebotomy service at the Royal United Hospital (RUH), Bath, UK, is a daily service which relies on effective communication between the phlebotomy team and ward-based healthcare professionals. The service currently covers approximately twenty separate hospital wards, and serves a proportion of the Royal United Hospitals Bath NHS Foundation Trust's patient capacity of 565 beds.
Blood stickers for patients who require blood to be taken are typically printed out in the afternoons, predominantly by junior doctors but also by nursing staff. These stickers are then left out for phlebotomist collection the following morning, with collected blood samples being sent to the laboratory for processing. Ideally the results are available by the early afternoon, allowing decisions regarding patient management to be made by their team within working hours.
Despite the importance of this everyday process, we identified long standing issues with the service. This was reinforced at the Foundation Doctors' Quality Improvement Panel early in the academic year, with several doctors new to the Trust raising the need to improve synergy between the teams (from both sides). Particular problems included the fact that blood stickers were often misplaced on the ward, with no ward having a predetermined location for them to be left for collection, or conversely to be returned to, if blood samples could not be taken (e.g. if patients were unavailable). Although each ward was familiar with their own system, this became an issue during evening and weekend shifts when teams overlap and cover numerous wards.
Ideally if a blood sample is not taken, the phlebotomy team need to hand over this information so that a doctor or nurse can reattempt as soon as possible, to prevent delays in results. However, we found that this handover of untaken bloods rarely took place, with healthcare professionals typically discovering untaken blood stickers late in the day, or only recognising that samples had not been taken when they found themselves waiting for non-existent results. In this case, once the blood samples were eventually taken, the task of reviewing the results then became the responsibility of the “on call” evening team. Not only was this adding to the burden on the limited evening staff, but it also meant that doctors who were less familiar with the patients were left making arguably less well informed clinical decisions.
Even if delayed results become available within working hours, there may be significant consequences for patient safety. Certain blood results are “time critical” (e.g. delayed pre-operative blood results postponing surgery), and unknown derangements (e.g. electrolytes such as potassium) can be life threatening if not promptly treated. Finally, timely patient discharges are essential, both from a financial perspective and to facilitate bed flow, enabling new admissions. As blood results are often a prerequisite to confirming a patient medically fit for discharge, pending blood results can delay this process.
Given the importance of an effective phlebotomy system, our aim was to improve the handover rates of untaken blood results across all wards covered by the phlebotomy service to consistently greater than 90% within a 12 month period.
Background
Following the “snapshot” feedback from the 36 junior doctors at the Foundation Doctors' Quality Improvement Panel, we designed two surveys aimed at both teams (one for junior doctors, and one for phlebotomists) to gain further insight into the issues facing the current service.
Thirty one feedback responses were received from the 82 junior doctors invited to participate. The survey revealed that although 38.7% (12 of 31) found the existing service satisfactory, almost a fifth (19.4%; 6 of 31) felt it was substandard. This was attributed to many factors. Firstly, although 87.1% (27 of 31) stated their ward had a designated location where blood stickers are left, untaken stickers were only returned to this same location by the phlebotomists in 32.2% (10 of 31) of cases. In this situation, blood stickers were reportedly found elsewhere on the ward (for example on a desk and by patients' bedsides). Thirty five point five percent of doctors felt this happened “often,” but of more concern, for 22.6% of doctors (seven of 31) this “always” occurred. Many felt that inconsistent communication resulted in a lack of formal “handover,” with over three quarters of doctors (24 of 31) reporting that a verbal handover did not routinely take place, and the remaining 22.6% (seven of 31) “never” receiving any form of handover.
The above data was wholly supported by the qualitative feedback collected during a junior doctor focus group, which included:
- “Usually good, but very dependent on the phlebotomist themselves”
- “Generally good but areas to improve are being told if bloods haven't been done so we know we need to do them, rather than having to find out later on”
- “…problems with communication at the weekend…”
- “The main issue is communication - if bloods aren't taken for whatever reason it is so much more helpful if we are notified so that we can do them ourselves rather than finding them as surprises halfway through the afternoon! Could be put back in one place?”
- “Finding bloods that are not taken is frustrating…”
In summary, the general consensus was that poor communication and the lack of standardisation were the main drivers behind the service's inefficiency. Several individuals highlighted the knock on effects this had for ward management, namely delayed results hindering their clinical decision making within working hours.
Interestingly, there was little correlation with the feedback from the eight phlebotomists contributing to this project (out of the 18 invited to participate), highlighting the lack of synchronisation between the two teams. In general, 100% (eight of eight) believed that blood stickers were always left out (and returned to) a set location on each ward, and if untaken, 75% (six of eight) felt that they “always” gave a verbal handover to ward staff.
In a wider context, we found that many of these drawbacks to the existing service were not unique to the RUH. Previous similar projects, both locally in Bristol and nationally in London, had identified similar “frustrations” with their current services.[1, 2, 3] Throughout all the projects the issue of effective communication appeared to lie at the root of the problem. Indeed, Brown et al reported that 96% of junior doctors felt more could be done to improve phlebotomy/doctor communication, although it was not stated how many doctors were included in this survey, and no feedback was sought from the phlebotomy staff. In contrast, by shadowing phlebotomists “in the field”, Pitchforth identified that success of their paediatric phlebotomy service relied too heavily on convoluted verbal communication with nursing staff and medical teams. Varied interventions had been adopted in these cases, with mixed success. Shoul et al found that the initial concept of diaries as a communication point was too expensive and impractical, instead developing the idea of ringbinders over three PDSA (Plan, Do, Study, Act) cycles to achieve 100% handover rates. Alternatively, clipboards and a bleep system have also been employed in the other hospitals. Advancing on these previous projects, we sought to find a novel and sustainable intervention that was tailored to the issues we had identified at the RUH.
Baseline measurement
Initial data collections focused on an elderly care ward during a single working week period (four days) to gain a “snapshot” of the problem. A proforma was used, measuring the number of blood stickers left out by the ward staff, the number which were untaken, and the proportion of these untaken bloods that were verbally handed over (as documented by the ward's doctors, who kindly agreed to assist with data collection). In addition to this, we focused on where the untaken blood stickers were left, ie if there was a set location in place. Finally, to quantify the burden of delayed blood results, we measured the number of pending results handed over to on call evening junior doctors.
Of the total 29 blood stickers left out, fifteen were untaken. Of these untaken bloods only three quarters were left in a set location, meaning that over a quarter were “lost” on the ward. In terms of handover, only 13% (two of 15) were verbally handed over. Overall, 13% of pending bloods needed to be handed to the evening on call team.
In order to meet our project aim of improving the handover rates of untaken blood results across the wards covered by the phlebotomy service, we planned on continuing to measure the handover process using this same proforma, but to gradually expand to all applicable wards (following optimisation of our intervention).
Design
The project team consisted of the two authors as representatives of the junior doctor cohort, with the perspectives of key figures within the phlebotomy team and ward teams consulted as the PDSA cycles evolved. We recognised that this was crucial in ensuring a concept that was universally preferred by the multidisciplinary teams. Our concept focused on creating a standardised location where bloods could be safely deposited and returned to if required. After consideration of different forms (ie diaries, clipboards, etc.), we settled on a box file, mainly as it seemed the most effective way to protect patient confidentiality, and would allow scope for organisation within the box itself. From a practical perspective, the box file is more robust in terms of durability on the wards, as well as being a secure structure.
We devised the idea of a “Phlebotomy Box”: a brightly coloured box file unique to the phlebotomy service that could be replicated across the wards, and easily identified by all teams. Key features of the box included:
Being placed in a standard location on all wards
Individual plastic wallets within the box labelled for each day of the week
Blood stickers being left within the corresponding wallet
Untaken blood stickers to be returned to this same location.
We used process mapping to demonstrate how the phlebotomy box could streamline the existing service, as shown by diagram 1 and diagram 2 (see “supplementary material”). By reducing the time phlebotomists waste looking for blood stickers and locating clinicians if they need to be verbally handed over, the process can be made more efficient, and similarly eliminates the need for doctors to search for untaken blood stickers. In this way, the phlebotomy box acts as a communication point between the two teams, removing the need for a verbal handover. Diagram 3 and diagram 4 demonstrate the difference between the two systems in practical terms (see “supplementary material”).
Supplemental material
Strategy
PDSA 1:
We started implementing changes on a single ward in order to optimise our prototype box. For continuity we primarily focused on our baseline ward (Ward 1), where issues had already been identified. Once we had selected an appropriate box file, the first aim was to identify an optimal location for the box to be placed. Initially we hypothesised that placing it on the ward's main desk would be best, and throughout the course of the week we trialled a series of locations (the main desk, the doctors' hub, and by the equipment trolley). However, feedback from the phlebotomy team suggested a more appropriate location to be where the blood samples themselves are deposited and collected.
We then focused on the organisation within the box as an additional intervention, introducing separate plastic wallets for each day of the week (with weekend wallets in alternate colours for clarification, as depicted in Diagram 4 (see “supplementary material”). These were well received by both teams, with no further amendments required.
PDSA 2:
Following optimisation, we met with the phlebotomy team and their manager to determine if any further amendments were required, aiming to ensure joint input from both teams. They emphasised the differing approaches each ward had when using the phlebotomy service, and the overriding theme arising from their focus group was the concept of “set rules” that both they and doctors could abide by to achieve a coordinated system.
We wanted to try and establish these set rules, which we predicted would help as a guide to the new phlebotomy service and usage of the phlebotomy box. As such, we trialled a novel set of instructions for wards to follow, which were placed on the inner surface of the box lid. This was welcomed by both ward staff and the phlebotomy team, and therefore a laminated version of the instructions was integrated into every box. Group working in this way highlighted the value of feedback in the development process, thus informing our next cycle.
As a further intervention, we arranged to attend the monthly meetings of both the ward clerks and ward matrons to present our “optimal” Phlebotomy Box. The main purpose was to introduce the concept to the fixed staff members on the wards, as they would be responsible for the phlebotomy box's upkeep and informing new staff on how to use it, thus helping to achieve a sustainable change. The idea was met with enthusiasm, and no further amendments suggested.
PDSA 3:
We therefore expanded the trial to a busier medical ward (Ward 2), and a surgical ward (Ward 3). The aim was to ensure the concept was universally suitable. The intervention first involved installation of phlebotomy boxes only. As hypothesised, the new system was largely successful in terms of handover, however on the surgical ward adherence was not meeting the 90% handover standard. This was attributed to the fact that the ward is staffed by multiple teams. In order to overcome this, the intervention was developed to include an additional education programme, which entailed individualised one to one teaching with ward staff. This represented the end of our PDSA cycles.
We then compared baseline handover rates pre-phlebotomy box on a final medical ward (Ward 4) to handover rates following its implementation, aiming to demonstrate a quantitative improvement following intervention. The improvement data confirmed the phlebotomy box was ready to be implemented throughout all hospital wards, supported by a funding grant secured following a successful application to the RUH “Innovation Panel” scheme.
This step was supported with an extensive education programme, including an oral presentation at all junior doctor teaching, hospital wide emails, and informative posters in core areas. The Phlebotomy Box was also publicised in the monthly hospital newspaper. A phlebotomy box was installed on all specified wards on the same day, to ensure a clear transition to the new system. Ward staff were consulted during the process to allow for clarification and questions.
Nine months after the establishment of the phlebotomy box system, a completing survey was sent to all junior doctors. Both quantitative and qualitative feedback was collected to determine the success and reception of the improvement, which are discussed in the results section.
Results
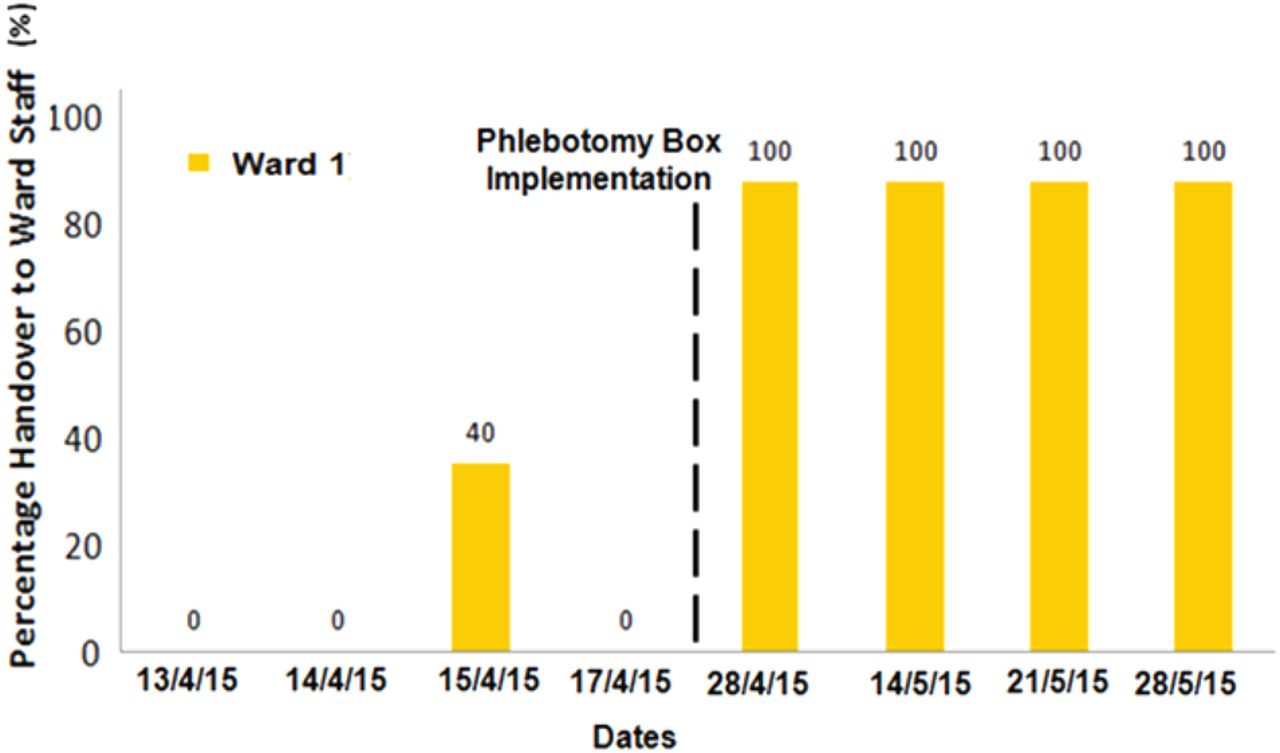
To put our results into context, up to 15 blood stickers might be put out daily on Ward 1. As demonstrated by Graph 1, the handover rate of untaken blood stickers to ward staff was mostly nonexistent on Ward 1 when baseline measurements were taken. However, implementation of the phlebotomy box system resulted in a 100% handover rate that was shown to be sustained over the course of a full month of monitoring.

Handover rates to ward staff on Ward 1, pre- and post-Phlebotomy Box
When the phlebotomy box was then trialled on Wards 2 and 3 (larger wards where up to twenty blood stickers might be put out each day), some variation in success was demonstrated. Ward 2 is a busy medical ward, and from the outset the box system achieved 100% handover rates, meaning that ward staff were consistently informed of all untaken blood stickers over the trialled months. Initially a similar pattern was seen on Ward 3, a busy surgical ward, but after four months the handover rate had become less consistent, with only 50% of untaken blood stickers being communicated. This was attributed to the fact that surgical teams have patients based on several wards, and so were not as familiar with the box system. However, after further focused staff education for the surgical teams, the Ward 3 handover rates once again returned to 100% (Graph 2).

Handover rates to ward staff on Wards 2 and 3 post-Phlebotomy Box
To gain further quantitative data we trialled the phlebotomy box on a final ward (Ward 4), after collecting baseline handover rates when the traditional phlebotomy system was still in place. Again, this is a large medical ward where around twenty blood stickers are printed in a typical day. From low handover rates ranging between 0% to 67%, a 100% handover was routinely demonstrated in the two weeks following its installation on the ward (Graph 3). Graph 4 represents these aforementioned stages in a run chart format, giving an indication of the prolonged timescale of data collection over four months.

Handover rates to ward staff on Ward 4, pre- and post-Phlebotomy Box

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Timeline of handover rates pre- and post-Phlebotomy Box on all four wards
Nine months after the hospital wide transition to the Phlebotomy Box system, we re-surveyed all junior doctors to gauge its reception and subjective success. Fifty five responses were received in total (from 92 respondents surveyed). Overall, 38% (21 of 55) found the service excellent, and 42% felt it was good, with only 20% (11 of 55) rating it satisfactory, and no doctors delivering a rating lower than that. This is in comparison to 6% (2of 31) of the first cohort finding the original system excellent, half finding it only satisfactory, and almost a fifth (6 of 31) deeming the original system substandard. The phlebotomy box represented a designated location for blood stickers for over 98% (54 of 55) doctors, an 11% increase from before, and untaken blood stickers were returned to it the majority of the time for 84% of staff, as opposed to 58% before it was introduced.
Most significantly, however, 91% (40 of 44) of doctors who were working at the RUH both pre- and post implementation of the Phlebotomy Box stated that they preferred the new system. This sentiment was echoed in the qualitative feedback collected, which included:
- “Convenient and safer than previous (fewer lost stickers!)”
- “The box makes things much more efficient and our blood stickers aren't going missing anymore. Much easier at the weekend as well as on unfamiliar wards you know where to look for blood stickers”
- “Great idea, has made a big difference and makes the day run more efficiently. thanks!”
- “I think it is a great project, especially for the weekend. It's nice and bright to look out for, especially for busy on-call docs!”
Lessons and limitations
The project aim was to improve the communication between the phlebotomy team and junior doctors, with the key focus of implementing a sustainable solution rather than a short term intervention. For this to be achieved, a system needed to be designed that would suit various ward environments. Building on previous ideas, we also wanted a system that offered a more secure place for blood stickers to be stored and collected. A key lesson learnt during the process was the importance of PDSA cycles, which helped to ensure that at each stage the model was optimised before full distribution across the hospital.
As enhancing multidisciplinary communication lay at the essence of the task, we ensured that all parties (doctors, ward nurses, clerks, and phlebotomy) were involved throughout the process by attending team meetings, collecting written feedback, and by individual discussion. Including their input during the planning helped to increase their support for a sustainable new system. However, despite this initial enthusiasm, we did identify certain teething problems on the more challenging wards when monitoring the new system, which we attributed to the fact that it was not possible to meet with the whole phlebotomist cohort when we attended their meetings, as not everyone was able to be present due to their shift allocation. In hindsight, assigning one of the phlebotomists the role of “lead,” and including them in the project team may have overcome this.
The project highlighted the barrier of convincing long term staff to embrace a novel system, and demonstrated that even a positive change can take time to establish in the face of deep rooted routines. Putting this learning point into practice, we timed the hospital wide installation of the phlebotomy boxes prior to the arrival of the new cohort of junior doctors. Establishing these before they could become accustomed to the old system allowed for a more a fluid transition.
In terms of limitations, while the qualitative feedback from staff nine months post-implementation was largely very encouraging, it would have been beneficial to quantitatively re-audit ward handovers to ensure a sustained change. Indeed, a minority of the qualitative feedback submitted suggests that further training for new phlebotomists is needed to keep standards up. To help achieve this, we identified that responsibility for staff education (as well as general box upkeep) would need to be handed over to a key figure who would oversee the phlebotomy box system in the long term. At the RUH this role was assigned the phlebotomy manager, who had been a source of enthusiasm throughout the project.
In terms of the data itself, as we escalated our optimised Phlebotomy Box from Ward 1 straight to Wards 2 and 3 to determine if the system would still work in busier settings, we did not collect any baseline data for the latter wards, which is a limitation. There was also the potential for the results to be affected by positive confounding bias, for example due to the change in doctors on each ward every four months, and the hiring of new phlebotomists throughout the year (both of which may have positively impacted the phlebotomy system, independent of our intervention). Finally, we have not explored the possibility that our results may have been affected by natural process variation. It was not realistic to monitor the handover rate of every untaken blood sample daily throughout the whole hospital; therefore, we have drawn our conclusions based on a limited number of our observations, yet have not performed any statistical tests to prove that these results are a product of chance. In order to overcome this, ideally more data would need to be collected (i.e. including more wards, and over a longer time period), and statistical tests would need to be employed.
Although the new system of the Phlebotomy Box has substantially helped to improve handover and communication between the phlebotomy team and doctors, while we continue to rely on physical blood stickers and forms there will always be the risk of them being mislaid, and hence the risk for communication failure. For this to be improved further, a future project should look into designing an electronic system between the two teams, thus removing the need for a physical handover point. We ceased data collection upon moving rotations to different hospital sites, but this is an avenue we hope to hand over to remaining junior doctors to explore in the coming academic year.
Conclusion
In summary, it was unanimously identified that lack of structured communication from both sides of the medical and phlebotomy teams represented a fundamental flaw in the pre-existing phlebotomy service in our hospital. The consequent delays in the availability of blood test results had the potential to compromise patient safety by impeding everyday management decisions. In a wider context, the financial impact of discharges delayed by pending blood results on the NHS must also be considered. However, by achieving 100% handover rates of untaken blood stickers, our innovative Phlebotomy Box has evidently resolved this issue. This appears congruent with the existing literature, the results of which support the introduction of standardised communication points.1–3
A significant improvement in communication and efficiency within the phlebotomy service has been demonstrated, with tangible benefits to care. Given its affordability and simplistic design, the Phlebotomy Box represents an easily sustainable intervention which could easily be replicated in other Trusts, particularly when supported by long term managerial staff.
Acknowledgments
We would like to acknowledge the contributions of the RUH phlebotomists alongside Dr Lesley Jordan, Dr Emily Hotton, Sarah Cook, Lisa Lewis, Mandy Budds and Dr Alexandra Ward. Without their support this project would not have been possible.
Footnotes
Declaration of interests Nothing to declare.
Ethical approval Formal ethical approval was not indicated for this project.