Article Text

Abstract
Traumatic brain injury (TBI) in the polytrauma situation is a phenomenon often seen at UK hospitals. Without immediate access to dedicated neurocritical care facilities, the potential for under-treatment of the underlying brain injury and serious neurological sequalae is high, especially if staff on the general intensive care units on which these patients are treated lack confidence in this area of practice, a reality confirmed by our baseline study.
We found that by engaging staff by implementing a regular simulation-based team training programme, we were able to boost the skills, knowledge, and ultimately confidence levels in treating TBI amongst these groups of staff. "Buy-in" by those concerned was high, and we found that self-reported scores for the attributes described above were improved considerably and consistently by our intervention. This quality improvement project has been rolled out through several iterations to become sustainable, has significant cost-saving potential, and will hopefully lead to proven improved clinical outcomes for this group of patients.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Our problem:
We identified that general intensive care (GITU) nurses felt under-confident of their understanding of the differing strategies employed in the management of the head-injured patient compared to the standard GITU case-mix.
Our context:
Traumatic Brain Injury (TBI) is very common in the UK, carrying significant morbidity and mortality. The treatment of TBI revolves around prevention of secondary brain injury by rapid access to neurosurgical intervention if indicated and prevention of further physiological insult by specialised medical management and high-quality neurocritical care.
This poses a potential problem for multiply injured patients who have also suffered TBI. Typically they are nursed in our (GITU) due to the compound nature of their injuries, and may potentially miss out on important neuro-critical care principles. For example, numerous studies confirm an association between even a single epidose of systemic hypotension (and consequent reduction in cerebral perfusion) occurring at any point after injury and poor neurological outcome[1]. This therefore leads to a different emphasis on arterial pressure maintenance on neuro-intensive care units. Similar differences in approach involve artificial ventilation strategy, glycaemic control, and treatments such as osmotherapy, cooling, and of course operative neurosurgery itself[2].
Our solution:
We sought to design a structured, simulation-based learning course for GITU nurses run by neurocritical care staff with set learning objectives to increase their confidence and familiarity with brain injury, the 'neurosurgical approach' and associated bedside equipment, and their ability to deal with various neurological crises, in the hope that this would lead to better care for TBI patients on the GITU.
Background
In order to set defined learning objectives for the course, we examined what we felt to be the most important variances between general and 'specialised' critical care knowledge and skills.
Various risk factors have been identified as correlating with poor outcome in TBI. Those occurring at or closely after the time of injury include the injurious mechanism, increasing age, abnormal pupillary size, low Glasgow Coma Score; and CT findings on arrival at the emergency department. These are associated with the primary injury and are essentially fixed at the time of injury[3], and we felt it was important that GITU nurses had an understanding of the above.
Other, crucial learning objectives to neurocritical patient care that we wished to teach are the so called 'secondary insults' which are known to be associated with poor outcome, but which are amenable to treatment, notably hypoxia, hypotension, hypo-and-hypercapnia, and hyperglycaemia[3]. In tandem with this, the high incidence of associated C-spine injuries was felt worthy of exploration, the hazards of patient transfer, the types and degrees of surgical intervention with demonstration of equipment such as the 'external ventricular drain', the importance of intra-cranial pressure (ICP) measurement, specialised medical management of high ICP, and what to expect when trying to wean and wake TBI patients from the ventilator and off sedation, respectively.
We decided on using a simulation-based course as this type of training has been widely shown to improve knowledge retention, teamwork and crisis management in various groups of hospital staff, including nurses. It allows the use of teaching methods that provide valuable and timely feedback and allow for repetitive practice in a safe environment conducive to adult learning. It also allows educators to measure outcomes related to specific learning objectives.
Simulation allows us to understand potential risks to patient safety and the rationale behind unfamiliar interventions in an integrative fashion [4]. There is a growing body of evidence that it can lead to error and cost reduction, and increased patient safety in high-risk circumstances. Therefore, we felt the effective use of simulation training as an intervention to improve both clinical and non-technical skills and knowledge would likely result in enhanced patient safety.
Baseline Measurement
We sent 10 course delegates a pre-course questionnaire (attached) which used a 5-point Likert-type scale (where a score of 5 = strongly agree, a score of 3 is neutral, and a score of 1 = strongly disagree) to explore candidate expectations and current knowledge and experience dealing with TBI patients using the following questions:
*I am looking forward to the course (mean score 4.44)
*I feel it will be relevant to my work (mean score 4.67)
*I understand the concepts of raised ICP (mean score 3.33)
*I understand ICP monitoring equipment (mean score 2.78)
*I know how to assess the brain-injured patient (mean score 3.00)
*I understand the role of the neurosurgeons (mean score 3.22)
*I am familiar with using (our) ICP protocol (mean score 2.89)
*I know how the C-spine is cleared safely (mean score 3.44)
*I am aware of all the risks of patient transfer (mean score 3.78)
*I know what to expect when waking up a patient (mean score 3.33)
*I feel confident in managing a crisis (mean score 3.33)
*I think this course will help improve patient safety (mean score 4.67)
See supplementary file: ds3304.pdf - “Pre-and post course Likert-scale questionnaires distributed to candidates”
Design
The specific intervention is a short day/half-day course for general intensive care unit (GITU) staff involving didactic teaching, interactive group sessions, workshop-style demonstration of unfamiliar equipment, and high-fidelity simulation. We called the course "NeuroSIM for Critical Care". Primarily aimed at nurses of all seniority, it was also open to Operating Department and ITU Technicians, physiotherapists, and other healthcare workers involved in the care of neurosurgical and head-injured trauma patients.
The proposal for the programme as a whole was devised by a core team of a consultant neurointensivist and an senior anaesthetic registrar with a subspecialty interest in neuroanaesthesia and whom had completed a simulation fellowship. It would be preceded by a pilot course at a local simulation centre; and devised such that the core team could run it themselves following the pilot course with solely a mobile, wireless high-fidelity simulation manikin to meet defined clinical and human factors-based learning objectives using relatively little resource reliance.
This gave us the potential for long-term sustainability. Following a suitable number of subsequent 'in-situ' courses, requiring only the attendance of small groups of nurses, staff trained under our proposal (coupled with standardised teaching materials) could then go on to cascade the teaching, piecemeal, to the learning needs of their own staff, reducing on-going costs. There is a constant outflow of enthusiastic trainees from the local simulation centre who have undertaken similar fellowships and who are already engaged with the project. From the data gathered after the pilot course, 92% of attendees thought that the orientation course should be re-run every one-to two years to refresh and update the objectives of the programme, resulting in a cyclical process of cost reduction following these specific courses.
Strategy
PDSA Cycle 1: A course was run at the local simulation suite. Pre-course and post-course questionnaires confirmed success in meeting learning objectives. Buy-in was confirmed by invitation afterwards by senior staff to provide in-situ simulation at the delegates' normal place of work. Results of post-course questionnaires (described later) confirmed that global improvements were reported in all pre-defined learning objectives, both immediately post-course and one month post-intervention. Free-text comments were invited, and encouraged to be constructive in nature, and we used them to help further refine future courses. For example, one comment suggested that some staff found it difficult to get to the course centre. We were therefore delighted to be invited to the GITU itself by senior staff to deliver further teaching. This gave us the ideal opportunity to test our course in an ‘in situ’ location – a simulation technique held in the actual workplace of the delegates. This has been shown to further enhance experiential learning, and can expose system-based latent risks to patient safety. We were interested to see how this might change the results of the data gathered during the next course.
PDSA Cycle 2: Taking into account feedback from the questionnaires, the simulation course was delivered again, only this time in-situ on the general intensive care unit (see attachment). The same scenario as the original course was used to teach the core principles we intended to impart. As the nature of in-situ simulation involves the participants being at work on a normal work day, this necessitated smaller numbers (but also reduced cost) as less staff could be released from duty at one time, and could return to work if clinical need demanded. This course was run by the original 'core' team of two. Questionnaires were again distributed which showed a very comparable level of improvement across the spectrum of our learning objectives compared to the first course. On the basis of this we decided not to alter the structure or content of future courses, but to run one more PDSA cycle to confirm that the in-situ environment continued to meet our objectives.
PDSA Cycle 3: Using a different set of learners to the last cycle, this PDSA process validated for us that the course we had designed was doing the job we had intended it to do. We made no changes to the course content and subsequent courses continue to run along the same structure and delivery mechanism. We do however continue to distribute questionnaires so that as staff become more confident we can identify any changes in their perceived learning needs, or respond to feedback; making changes to the course as and when they become necessary to address these.
See supplementary file: ds3305.docx - “The 3 PDSA cycles completed during the development of our course”
Post-measurement
The results of the post-course questionnaires were as follows:
*The course was enjoyable (mean score 4.8, 7% improvement)
*I feel it will be relevant to my work (mean score 4.67, no change)
*I understand the concepts of raised ICP (mean score 4.6, 25% improvement)
*I understand ICP monitoring equipment (mean score 4.4, 32.4% improvement)
*I know how to assess the brain-injured patient (mean score 4.3, 26% improvement)
*I understand the role of the neurosurgeons (mean score 4.5, 26% improvement)
*I am familiar with using (our) ICP protocol (mean score 4.3, 28% improvement)
*I know how the C-spine is cleared safely (mean score 4.1, 13.2% improvement)
*I am aware of all the risks of patient transfer (mean score 4.4, 12.4% improvement)
*I know what to expect when waking up a patient (mean score 4.4, 22% improvement)
*I feel confident in managing a crisis (mean score 4.2, 14% improvement)
*I think this course will help improve patient safety (mean score 4.8, 12% improvement)
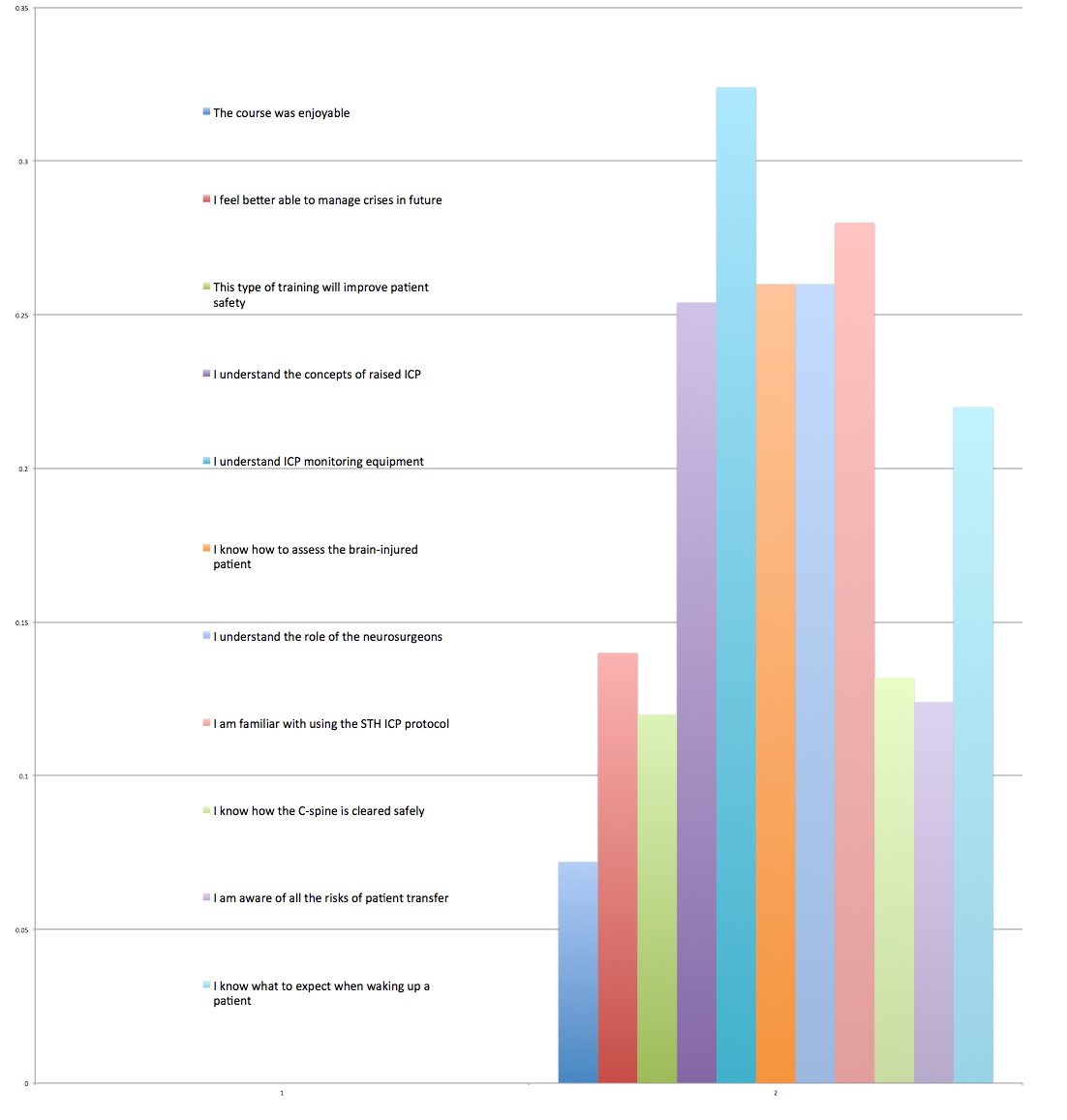
For each PDSA cycle, self-reported scores by the attendees were high for satisfaction with the course; increase in core knowledge relating to our pre-defined learning objectives with percentage increases in self-reported scores ranging from 7% to 32.4% (see attached graph).
Follow-up surveys (worded the same as the immediate post-course questionnaire) were sent one month after the initial course, which confirmed that outcome scores remained high (although knowledge retention very slightly lower, confirming a continuing education requirement) and also included positive comments about the direct effect on their practice:
"Well done"
"We ought to send more staff to this"
"Very informative, all speakers relevant, and approachable"
"Very enjoyable"
"Would like more information on [different types of] head injuries"
"2 neurosurgical patients looked after since study day, many thanks"
"V well taught day"
"I've looked after 3 neurosurgical patients since the study day, thanks again"
See supplementary file: ds3303.png - “Graph illustrating % increase in self-reported Likert scale scores post-course”
Lessons and Limitations
We learned that to implement a new training course one comes up against a number of obstacles, primarily logistical. We had expected some degree of resistance regarding the simulation-based aspect of the course, but in fact people found this a very effective way of learning and demonstrating key principles. We found that due to the multidisciplinary nature of the course there was by necessity a lot of communication, and some issues relating to venues, transport, and release from clinical duties.
Running the courses was relatively resource-intensive, but got easier with each session. The eventual aim is for the knowledge imparted to be cascaded by senior GITU staff; reducing the frequency of the courses. We felt that simulation was the best way of cementing the topics that the multidisciplinary team need to know, but are looking at ways to reduce the time burden on the educators. For example, rather than one person delivering the same lecture at several different courses, a screencast could be made available on the trust intranet that can be viewed by learners at their leisure, along with quick and standardised reference guides to key topics, for example the locally used, evidence-based algorithm used in the medical management of raised ICP.
As yet, we have no way of proving our intervention has lead to improved patient outcomes, but intuition would suggest that a practitioner who is up-to-date on the required knowledge and skills will be able to deliver safer, better quality care, resulting in superior neurological outcomes.
Conclusion
The problem that we faced was that following a restructuring of our trauma care, a group of (primarily nursing) general intensive care staff were being exposed to a group of patients for whom they did not normally care, and they lacked confidence doing so. To tackle this issue we implemented a simulation based team training programme to help them manage neurosurgical patients with head injuries, hoping that this would ultimately lead to better outcomes for this subgroup of ITU patients. To do this we made a proposal to a multidisciplinary group of potential stakeholders, and devised an educational programme with their input.
We proceeded on the basis of our own clinical knowledge, background research, and the intuitive assumption that better care would be delivered by those with an enhanced knowledge and skill-set. We based our PDSA cycles on outcomes measured from self-reported surveys filled in by course delegates. These have demonstrated continuous self-perceived benefit to those attending.
We believe that as a result the quality of our TBI patient care will ultimately be improved by our intervention, however, demonstrating the benefits of simulation training translated into tangible quality improvement is difficult. Previous work[5] reports that implementing neurocritical care principles for TBI patients improves clinical outcomes, shortens hospital stays, and reduces total cost of care, and can translate into large financial savings. Current data from senior GITU staff at our institution [personal communication] suggests that our GITU currently cares for between three and five patients per month with TBI, a number expected to increase. At an approximate cost of £1000 per day for an intensive care bed in the UK, there is clearly the (albeit currently theoretical) potential for cost-saving from our relatively simple intervention, as well as the promise of improved patient outcomes. Our future intention is to use similar outcome measures once we have trained the majority of departmental staff to see whether this can be said for our own institution. However, with the training of staff on-going and necessarily limited by factors such as the 'safe' release of departmental staff and/or availability for each session, we cannot currently define pre- and post-intervention periods for the whole project.
Reflecting on the project as a whole we both feel a great sense of satisfaction. With a development time of months, the roll-out of this intervention has gradually already been executed. Whilst the targeted employees were mainly the nursing staff, other stakeholders included physiotherapists, ITU technicians, neurosurgeons, neuroanaesthetists, and clinical nurse educators. It could easily be argued that medical staff on the unit would benefit from the course, and we plan to consider this and the potential effect on the existing course and its aims in the future.
References
TRAUMA.org: Neurotrauma: Cerebral Perfusion Pressure. [Internet] (2000). Available from http://www.trauma.org/archive/neuro/cpp.html (Accessed 15th March 2014).
Mishra LD, Rajkumar N,Hancock SM. Current controversies in neuroanaesthesia, head injury management and neuro critical care. Contin Educ Anaesth Crit Care Pain 2006;6(2):79-82.
Smith M. Neurocritical care: has it come of age? Br. J. Anaesth. 2004;93(6):753-755.
Binstadt ES, Walls RM, White BA, et al. A comprehensive medical simulation education curriculum for emergency medicine residents. Ann Emerg Med. 2007;49(4):495-504, 504.e1-11.
Mirski MA, Chang CWJ, Cowan R. Impact of a Neuroscience Intensive Care Unit on Neurosurgical Patient Outcomes and Cost of Care. J Neurosurg Anesthesiol 2001;13(2):83–92
Declaration of interests
Nothing to declare.
Acknowledgements
I am immensely thankful for the help and guidance of Dr Stefan Jankowski, Consultant Neuroanaesthetist, Sheffield Teaching Hospitals NHS Foundation Trust, for his tireless work and encouragement in helping to drive the project forward.
Supplementary materials
Supplementary Material for Simulation-based training improves ITU staff knowledge in the management of head injuries.
Extra information supplied by the author
Files in this Data Supplement:
{kind=link}