Article Text

Abstract
The laryngeal mask airway (LMA) is used to facilitate adequate ventilation in the majority of procedures requiring general anaesthesia in the UK. Excessive LMA cuff pressure and/or volume, generated by injection of air to form an adequate seal within the upper airway, has been associated with pharyngolaryngeal morbidity, an indicator of quality in anaesthetic practice. However, measurement of LMA cuff pressure to limit excessive cuff pressure is not routine practice, despite trial data showing this reduces adverse outcomes. Our aim was to reduce morbidity from the LMA through the implementation of an educational and interventional program targeted at anaesthetic nurses and operating department assistants (ODA), to alter their physician colleagues’ practice. LMA cuff pressure measurements were made, and postoperative outcomes recorded, in an observational cohort of surgical patients over an initial 2-month period. These results, including patient morbidity and the evidence for LMA cuff pressure measurement, were presented to anaesthesia providers and their assistants. An implementation plan to adjust pressures within recommended levels was then undertaken by anaesthesia assistants.
In 90 patients, >95% of LMA pressures were beyond the recommended level; higher volumes of injected air correlated with excess pressure (r=0.58; p<0.0001) and were associated with pharyngolaryngeal morbidity in 28% patients (P=0.04). There was no association with difficulty in LMA insertion, duration or type of surgical procedure. In the implementation cohort (102 patients), pharyngolaryngeal morbidity was reduced to 11% (P=0.001) in the 45 patients where LMA cuff pressure was reduced to within normal limits (absolute risk reduction: 38% (95% CI: 22-54%). LMA manometry in three patients (95% CI: 2-5) was required to prevent an episode of postoperative pharyngolaryngeal morbidity.
A systematic educational and interventional program targeted at the entire perioperative anaesthesia team, but implemented by anaesthesia assistants, can improve perioperative safety and quality.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
The laryngeal mask airway (LMA) device facilitates effective ventilation in the majority (56%) of 2.9 million patient-episodes of general anaesthesia per year in the United Kingdom (1). Used in over 200 million patients worldwide, the LMA device is associated with appreciable, adverse patient-related perioperative outcomes, ranging from sore throat, delayed discharge, and (rarely) life-threatening complications (2). Insufflation of air into the cuff of the LMA (usually by an anaesthetic assistant in the UK) maintains a patent airway under general anaesthesia through its close apposition with the pharyngolaryngeal anatomy (3). In the event of an excessive volume of air being insufflated, and therefore excessive pressure generated, local tissue trauma may develop. Recent data has confirmed manufacturers’ warnings that higher cuff inflation pressures are associated with pharyngolaryngeal morbidity (2). However, routine measurement of LMA cuff pressures in theatres is rarely practiced, perhaps reflective of a wider reluctance to adopt evidence-based practice in this clinical arena. There were no guidelines in place at UCLH governing the measurement of cuff pressures in theatres. We sought to improve the quality of LMA practice in our institution through an implementation program to change anaesthetists’ practice by targeting and empowering anaesthesia assistants.
Background
The LMA has transformed anaesthetic practice and as designs have evolved, their application has widened. They are now used in 56% of the 2.9 million general anaesthetics given in the UK each year (1).
Over the years the overall safety of anaesthesia has improved considerably. As a consequence, major morbidity after ambulatory surgery is rare. Addressing the more minor consequences, such as pharyngolaryngeal morbidity, therefore becomes increasingly important from the patient’s perspective in improving their experience and overall satisfaction. Sore throats have been reported as one of the most undesirable outcomes in the post-operative period (4) and adversely affects patient experience. Studies have reported that post-operative sore throats following the use of an LMA may be as high as 42% (5). Excessive cuff pressures and malposition of LMAs may also lead to the less common, but more serious, consequences of nerve injury and vocal cord paralysis.
Previous research, including a prospective randomised trial carried out by Seet et al (2), has concluded that using manometers to ensure that LMA cuff pressure did not exceed 60cmH2O reduces pharyngolaryngeal morbidity by 70%.
In today’s healthcare climate, with an ever growing emphasis on patient safety, the search is on to find the means and ways of reducing iatrogenic injuries arising from patient care.
Baseline Measurement
SQUIRE (Standards for Quality Improvement Reporting Excellence) guidelines were adhered to (6). The protocol was reviewed by the University College London/University College Hospitals Biomedical Research unit, who confirmed that the proposed study represented clinical audit and service evaluation; therefore, the study did not require approval by the research ethics committee.
90 patients (>14 years old) undergoing elective surgical procedures under general anaesthesia requiring an LMA, as determined by their attending anaesthetist, were studied. Anaesthesia practice and analgesic prescription was determined by the attending anaesthetist. An LMA was inserted, and the cuff was inflated as per usual local practice. The volume of air used and the LMA intracuff pressure were recorded using a calibrated manometer (VBM Medizintechnik GmbH, Sulz a.N., Germany). High cuff pressure was defined as >60cmH2O, according to manufacturers’ stated upper limit. These data were not revealed to the attending anaesthetist or anaesthetic assistant. Presence of sore throat was assessed 2-4h postoperatively. Following the first cohort, LMA cuff pressure data and postoperative outcomes were presented to the department of anaesthesia and anaesthetic assistants.
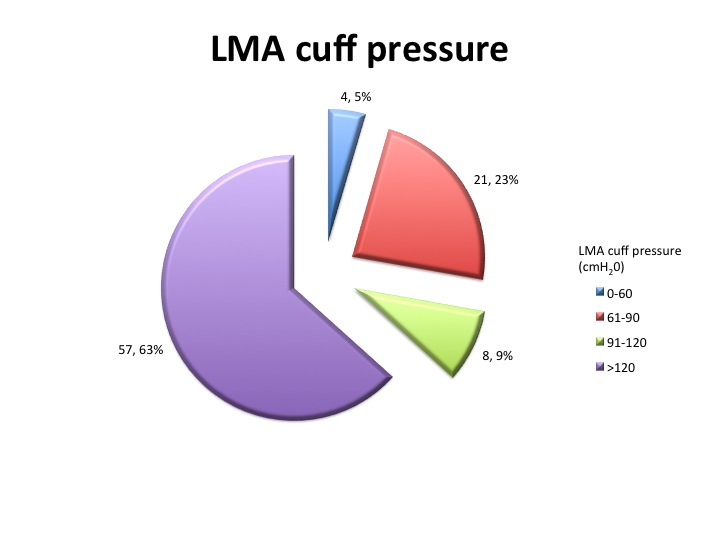
The results showed that almost all LMA cuffs were overinflated and only four (5%) were inflated to within the manufacturers' recommended pressure of <60cmH2O. In addition to this, 57 (63%) of recorded readings exceeded the scale of the manometer and were therefore recorded as >120cmH2O (see Figure 1).
25 (27%) patients reported a sore throat in recovery and 20 (83%) of these were deemed mild.
None of the four patients who had a cuff pressure within normal limits developed a sore throat. Conversely, 16 out of 25 (64%) who developed a sore throat had a cuff pressure >120cmH2O.
See supplementary file: ds1825.jpg - “Figure 1”
Design
Following the first cohort, LMA cuff pressure data and postoperative outcomes were presented to the department of anaesthesia and anaesthetic assistants.
The results showed that LMA cuff pressure was not routinely measured in theatre and that the vast majority (96%) of patients had cuff pressures greater than those recommended by the Royal College of Anaesthetists and manufacturers of the devices.
It has been shown that estimating cuff pressures by palpation of the pilot balloon is inaccurate and a manometer should be used.
As a result of these findings the anaesthetic department at UCLH invested in manometers to ensure that there was one available in each theatre. The anaesthetic assistants received educational guidance on using the manometers and adjusting the cuff pressure to within recommended limits (<60cmH2O). During the initial audit the anaesthetic assistants had watched us measure numerous cuff pressures in theatre so were already familiar with their use. The educational programme began with the verbal presentation of the initial findings and demonstration of inflating and measuring LMA cuff pressure using a manometer. Explanation of the dangers of overinflation, the improved seal with reduced cuff pressures, and the avoidance of morbidity such as sore throat were given. The manometers purchased were very user friendly and clearly demonstrated appropriate inflation pressures using a colour coded scale. We visited each theatre and observed the anaesthetic assistants using these manometers in patients.
Adherence to this change in practice was audited 6 months later.
Strategy
The failure of perioperative medicine to implement such evidence-based practice is observed across similar medical disciplines: despite repeated efforts, clinical practice guidelines infrequently alter physician behaviour (7, 8). Physician adherence to guidelines may be hindered by a variety of barriers (9). The chief barriers preventing alterations in LMA practice by the anaesthesia team are likely to hinge on outcome expectancy (lack of local evidence), an inability to overcome the inertia of previous practice, and external barriers such as lack of manometers. To address each of these possibilities, we applied principles gleaned from the analysis of implementation programs that have been associated with successful intermediate results (10). First, we ensured that all anaesthesia providers had clear involvement in the quality improvement efforts, enabling agreement with, and adherence to recommendations, whilst improving knowledge and delivery of best practice. Second, the joint involvement of anaesthetists and anaesthetic assistants ensured that teamwork was a major component of the implementation process. The fact that the anaesthetic assistants knew the benefits of using a manometer allowed them to feel more confident in explaining the importance of their use if challenged by the attending anaesthetist. Since this implementation program, the use of manometry as a standard of care for LMA insertions has been adopted as standard of care at University College Hospital.
Results
Following the introduction of manometers and education programme, we measured the cuff pressures of 102 patients with LMAs. The availability and use of manometers had resulted in a measurable decrease in LMA cuff pressures. The number of LMA pressures that were within the recommended limits increased from 5% to 43%. Those that exceeded the capabilities of the manometer reduced from 64% to 16%. Although we did not specifically measure the time taken to perform the measurement, it only takes a matter of seconds and therefore adds no significant time to that spent in the anaesthetic room.
Our data confirmed correlation between elevated cuff pressures and incidence of sore throat (p<0.0000001). There was a reduction in sore throat in those patients in whom a manometer was used however this was not statistically significant.
See supplementary file: ds1830.png - “Initial versus re-audit”
Lessons and Limitations
Despite the change in practice with the provision of manometers in all theatres and the implementation of staff education, adherence to the recommended standards remained suboptimal. In order to ensure that the improvements are maintained and built upon, such that the guidelines are followed 100% of the time, ongoing training is required.
High staff turnover and the use of agency anaesthetic assistants compound the difficulties in ensuring that these improvements are sustained. The education and training must be regularly repeated and incorporated in to the local induction programme.
Repeat audit of departmental practice, as a way of quantifying adherence to these guidelines, is required and comprises one of the pillars of clinical governance.
Conclusion
Since this implementation program, the use of manometry as a standard of care for LMA insertions has been adopted as part of routine practice at University College Hospital.
The introduction of manometers resulted in a measurable decrease in intracuff pressures. The number of LMA cuff pressures within the recommended limits increased from 4% to 43%. Those that exceeded the capabilities of the manometer reduced from 64% to 16%.
Routine manometry to keep cuff pressure within normal limits is associated with reduction in the incidence of pharyngolaryngeal morbidity. This is a very important finding given the number of patients undergoing general anaesthesia with LMAs world wide, with the potential to significantly reduce post-operative morbidity and improve patient experience.
Implementation of best anaesthetic practice requires a systematic team approach, specifically empowering non-physician assistants to deliver optimal care.
References
Cook T, Woodall N, Frerk Cl on behalf of The Fourth National Audit Project. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: Anaesthesia. Br. J. Anaesth. 2011; 106 (5): 617-631.
Seet E, Yousaf F, Gupta S, Subramanyam R, Wong DT, Chung F. Use of manometry for laryngeal mask airway reduces postoperative pharyngolaryngeal adverse events: a prospective, randomized trial. Anesthesiology. 2010; 112(3): 652-7.
Brain AI. The laryngeal mask--a new concept in airway management. Br J Anaesth. 1983; 55(8): 801-5.
Higgins PP, Chung F, Mezei G. Postoperative sore throat after ambulatory surgery. Br J Anaesth. 2002; 88: 582-4.
Brimacombe J, Holyoake L, Keller C, Barry J, Mecklem D, Blinco A et al. Emergence characteristics and postoperative laryngopharyngeal morbidity with the laryngeal mask airway: a comparison of high versus low initial cuff volume. Anaesthesia. 2000; 55(4): 338-43.
Ogrinc G, Mooney SE, Estrada C, Foster T, Goldmann D, Hall LW, et al. The SQUIRE (Standards for QUality Improvement Reporting Excellence) guidelines for quality improvement reporting: explanation and elaboration. Qual Saf Health Care. 2008;17 Suppl 1:i13-32.
Lomas J, Anderson GM, Domnick-Pierre K, Vayda E, Enkin MW, Hannah WJ. Do practice guidelines guide practice? The effect of a consensus statement on the practice of physicians. N Engl J Med. 1989; 321(19): 1306-11.
Woolf SH. Practice guidelines: a new reality in medicine. III. Impact on patient care. Arch Intern Med. 1993; 153(23): 2646-55.
Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, et al. Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999; 282(15): 1458-65.
Chou AF, Vaughn TE, McCoy KD, Doebbeling BN. Implementation of evidence-based practices: Applying a goal commitment framework. Health Care Manage Rev. 2011; 36(1): 4-17.
Declaration of interests
We declare that we have no conflict of interest.
Acknowledgements
Ellie Walker and Isabelle Reed would like to be joint first authors as this would accurately represent our equal input to this quality improvement project.
We thank the Academy of Medical Sciences/Health Foundation Clinician Scientist scheme (GLA), and Centre for Anaesthesia, Critical Care and Pain Management for financial support.
We also thank Professor Martin Marshall (Professor of Healthcare Improvement, University College London) for helpful discussions.
This work was undertaken at University College London Hospitals NHS Trust/University College London who received a proportion of funding from the Department of Health UK NIHR Biomedical Research Centre funding scheme.
But most of all we would like to thank Gareth Ackland for doing the statistics and Simon Clarke for ongoing mentoring throughout this project.
Supplementary materials
Supplementary Material for An implementation program targeted at non-physician, anaesthesia assistants improves the quality of laryngeal mask anaesthesia
Extra information supplied by the author
Files in this Data Supplement:
{kind=link}
{kind=link}