Article Text

Abstract
A satisfactory patient care culture model can help improve most patients’ quality of care in a hospital. This study aims to improve patients’ experiences (PX) by implementing a culture model at King Abdul-Aziz Armed Forces Hospital in Dhahran, Saudi Arabia. To achieve the research aim, a set of interventions were implemented that included a patient and family advisory council, empathy training, recognition of the PX, leadership–patient interviews, PX champions and quality improvement. These interventions were further measured using the Hospital Consumer Assessment of Healthcare Providers and Systems survey in the inpatient, outpatient and emergency departments. The improvement project was conducted in 2020, focusing mainly on transforming the culture and launching activities targeting specific touchpoints identified as priority areas. After making these changes, the hospital saw improvements in all patient relationships, with an average score across all dimensions collectively increasing by more than 4%. The quality improvement project using the PX culture model approach demonstrated significant improvements. In addition, employee involvement in patient care has become a significant factor in improving the quality of care. The critical elements for improving the PX and culture included recognising staff and creating networks across the system through effective leadership, employee engagement and engagement of patients and their families.
- Patient satisfaction
- Quality improvement
- Organizational Culture
- Patient-centred care
- Patient Reported Outcome Measures
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Patient satisfaction
- Quality improvement
- Organizational Culture
- Patient-centred care
- Patient Reported Outcome Measures
WHAT IS ALREADY KNOWN ON THIS TOPIC
Beryl Institute has defined the patient experience (PX) as ‘the sum of all interactions shaped by the organisation’s culture that influence the patient perceptions across the continuum of care’.1 PX represents a valid indicator and measure of patient-centred care, one of the healthcare quality domains.2
WHAT THIS STUDY ADDS
King Abdul-Aziz Armed Forces Hospital (KAAB-AFH) defined PX improvement through effective change by adopting a plan with two main drivers: (1) to define hospital priorities based on the Hospital Consumer Assessment of Healthcare Providers and Systems survey findings and (2) to implement evidence-based changes to improve the culture of care. The Improvement project focused primarily on transforming the PX culture and launching activities focused on specific touchpoints identified as priority areas.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
A quality improvement project using a PX improvements model demonstrated significant improvements in PX culture in KAAB-AFH and positively impacted total PX scores across inpatient, outpatient and emergency department settings. Based on these positive outcomes, future studies in various Saudi hospitals can be conducted, contributing to future research, policy, and most importantly, practice, that is, the implementation of PX improvement throughout the country.
Introduction
Patient experience (PX) is an independent dimension of quality of care, clinical efficacy and patient safety.1 2 The Beryl Institute has defined the PX as ‘the sum of all interactions shaped by the organisation’s culture that influence the patient perceptions across the continuum of care’.3 In addition, the PX represents a valid indicator and measure of patient-centred care, one of the healthcare quality domains.4
PX is associated with increased clinical efficacy and safety, making it one of the top priorities for healthcare organisations in the short and long term.5 6 At the same time, a cross-disciplinary analysis published by Press Ganey in the 2017 Strategy Report demonstrated the interdependent relationship between PX, safety, service quality, workforce engagement and financial resources. According to these reports, an improvement in any of these areas can positively impact others and support progress in an improvement project, while a defect or deficiency in any of these areas can compromise other areas.7 Thus, although PX is multifaceted, learning about what matters to patients during illness provides a basis that can help guide future practice.8
It is widely recognised that patient engagement and voices are powerful tools for improvement.8 9 Consequently, several approaches have been developed to improve PX culture in the hospital. For instance, the Agency for Healthcare Research and Quality recommended establishing a patient and family advisory council (PFAC), as working with patients and families is an integral part of patient-centred and family-centred care and is necessary to improve quality and safety.9 It is essential to involve patients and their families in healthcare procedures as consultants, assess how they view the service, and make them valuable partners in order to mitigate medical errors while improving the safety and quality of care.10 In addition, Planetree International’s patient-centred care standards list empathy training as one of its standards, which positively impacts PX through patient engagement and improves treatment outcomes.10 Empathy is a characteristic of communication between a patient and a healthcare professional in general practice and is considered the basis of relationships.11 12
Over the past decades, the healthcare system of the Kingdom of Saudi Arabia (KSA) has dedicated itself to improving the quality of healthcare services through improved PX.13–15 A recent literature review on PX and satisfaction reported a strong relationship between educational attainment, income and satisfaction levels.13 In addition, understanding the patient’s point of view could improve their experience. A summary of studies has shown that developing teamwork between patients and healthcare providers through mutual communication can improve PX.13–15 Nevertheless, there is a scarcity of empirical studies that examine how to improve the average PX scores in inpatient, outpatient and emergency departments. Hence, this study aimed to explore how to improve the average PX scores in inpatient, outpatient and emergency departments at King Abdul-Aziz Armed Forces Hospital (KAAB-AFH), and contribute to the goals of the Saudi Ministry of Defense to foster excellence and leadership.
Methods
Design and setting
This was a cross-sectional research, conducted at KAAB-AFH from July 2019 to the end of September 2021. To address the research aim, the standardised Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey was applied to explore the PX and based on findings to improve PX at least by 4% or more in inpatients, outpatients and emergency departments, thereby setting out a 2-year target of benchmarks16–20 (figure 1).

Action plan of research based on the research aim. HCAHPS, Hospital Consumer Assessment of Healthcare Providers and Systems.
Benchmarking in healthcare is defined as the continuous and collaborative discipline of measuring and comparing the results with those of the best performers in evaluating an organisation’s performance. Benchmarking allows hospitals and practitioners, individual physicians and other healthcare organisations to track their own performance.19 20 Two types of benchmarking can be used: (1) internal benchmarking—to identify and compare best practices within an organisation, and to compare current practices over time; (2) external benchmarking involves the use of comparative data between organisations to evaluate performance and identify improvements that have proven effective in other organisations. Because KAAB-AFH targets are set annually rather than biennially, this study adopted an external benchmarking approach.19 Thus, based on the best practices of research, a goal was set, taking into account the performance of a third-party similar facility. The baseline was considered the data of the 4th quarter of 2019, which was 83.96% (inpatient), 66.53% (outpatient) and 59.75% (emergency) with an increase of at least 4% by the 4th quarter of 2021.
Data collection and intervention
As shown in figure 1, the aim of the research was achieved in two stages. At first stage, the primary driver was to identify hospital priorities, based HCAHPS survey. The HCAHPS survey is a 29-item instrument and data collection methodology for measuring patients’ perceptions of their hospital experience (2006).16 17 Alanazy et al translated the survey and validated the Arabic version of the survey. The study findings showed that the overall Cronbach’s α for the Arabic HCAHPS version was 0.93, showing good internal consistency.17 According to the WHO, quality of care is the degree to which health services for individuals and populations increase the likelihood of desired health outcomes. As countries commit to achieving health for all, it is essential to carefully consider the quality of healthcare and health services that will be equitable for all and not vary in quality based on gender, ethnicity, geographical location and socioeconomic status (SES). Thus, as this research aimed to improve the overall PX culture, no demographic data were collected, that is, age, gender and SES.18
The secondary driver was to implement evidence-based changes to enhance the culture. To achieve the secondary drivers, the research team developed a PX culture model, shown in figure 2.

Patient experience culture model.
The model consisted of six steps:
PFAC—a necessary step was to develop the structure and responsibilities of an interdisciplinary team to initiate PFAC. First, the plan included the personal characteristics of patient advisors, a detailed selection process including personal interviews, appointing the advisors, orienting them to the hospital, and signing consent and confidentiality forms. Then, the council started to discuss PX with two patient advisors.
Empathy training—a 4-hour workshop for training registration and clinical staff was implemented, including service excellence training.
Recognition for PX—staff who received positive comments and were acknowledged by patients were awarded a certificate of appreciation from the hospital director.
Leadership–patient interviews—as part of the weekly leadership safety walk rounds, the leaders interviewed patients regarding their stay in the hospital and the PX Head documented the patients’ comments for follow-up.
PX champions—in every department and nursing unit, a PX Champion was selected to work part time to follow up on the implantation of the PX action plans in their area and to share the knowledge and information about PX with healthcare providers in the same area.
Quality improvement—to conduct quality improvement projects in inpatient, outpatient and emergency to develop the PX priorities based on HCAHPS results.
Study of the interventions
The improvement project was conducted in 2020, focusing mainly on transforming the culture and launching activities targeting specific touchpoints identified as priority areas. The first intervention involved patients and their families and developed a standardised process for interviewing and selecting patient and family advisors who were recognised as PFAC members. The second intervention involved standardising the process for dealing with patient comments by developing a policy for responding to positive and negative feedback and rewarding staff based on positive comments. The third intervention included empathy training, workshops and a series of lectures for all staff. Leadership interviews with patients as part of the bypass was also one of the methods to increase the patient care culture. Moreover, to create a network and facilitate communication for the PX initiative, PX champions were appointed in clinical departments. Evidence-based change ideas were developed to target aspects of culture of care (table 1).
Evidence-based change ideas to target the culture of care
The evidence-based change ideas focused on patient care priorities that were selected from the Press Ganey Solution Starter, showing the percentage of successfully implemented changes out of all planned changes in quality improvement projects in inpatient, outpatient and emergency settings with example HCAHPS results presented in table 2. This was followed by evidence-based change interventions focusing on patient care priorities, based on the ‘Getting Timely Appointments, Care and Information’ report by 7, which provides recommendations on techniques and procedures to consider when a healthcare organisation begins implementing an improvement strategy.19 Recommendations are organised by composite and global metrics of the HCAHPS Clinician & Group Expanded Survey, the combination of reviews of comments from previous surveys, literature reviews, client testimonials, patient focus groups and Press Ganey Client Advisory Board experts’ feedback.19 The priority areas included:
Inpatient department—(1) improving PX in inpatients by focusing on accommodation and comfort for visitors and (2) improving PX at discharge.
Outpatient department—(1) improving PX in outpatients by focusing on the courtesy of registration staff.
Emergency department—(1) improving PX in emergency room (ER) by focusing on waiting time to see the physician (table 2).
Compliance rates of implemented evidence-based change ideas focusing on PX priorities.
The improvements were monitored over time by the outcome and process measures in accordance with the key performance inidcators (KPIs) based on the PX culture model (table 3).
List of outcome and process measures
Data analysis
Data were analysed using QI Macros statistical process control software package. Quantitative measures (numerical assessment of processes and outcomes) were collected over time and reported as control charts with phase analysis for the preintervention and postintervention phases. The corresponding mean, upper control limit and lower control limit were calculated using the to identify improvements in these measures. To test the mean difference between three groups, a one-factor ANOVA was used. To determine the statistical significance of findings, a p≤0.05 was considered for statistical significance at 95%.
Results
This first of its kind study in KAAB-AFH achieved its aim. This study improved patient safety experience and care using a PX culture model. The improvement project was unique in breadth and scope as it involved patients, families, staff and leadership engagement for shared PX improvement. The project implemented the corresponding changes using the PX culture model approach. The PX culture model approach demonstrated significant improvements in PX culture at KAAB-AFH and had a positive impact on overall PX scores across inpatient, outpatient and emergency department settings.
Table 4 shows the average results before and after improvement, the number of survey respondents and corresponding p-values. An overall improvement occurred in all departments, and the improvement has been maintained for four consecutive quarters. The outpatient, emergency department and inpatient follow-up chart average quarterly PX scores showed an upward trend, the improvements in the outpatient (p=0.037) and emergency department (p=0.010) PX scores were statistically significant. This allows to suggest the more work is required to improve PX in inpatient department that will lead to statistically significant differences and better performance.
Patient experience before and after improvements
Key to the success of this project was leadership commitment and tireless support to help align the PX culture model with organisational priorities and strategies. Employee involvement in patient care has become an effective culture factor for improving the quality of patient care. As shown in figure 3A, the inpatient experience increased from 83.58% in Q2-2019 to 89.62% for Q3-2021; the outpatient experience (figure 3B) increased from 64.1% in Q2-2019 to 73.34% for Q3-2021. Lastly, the ER PX increased from 58.09% in Q2-2019 to 67.81% for Q3-2021 (figure 3C).

Control charts. (A) Inpatient experience, (B) outpatient experience, (C) emergency room (ER) experience. LCL, lower control limit; UCL, upper control limit.
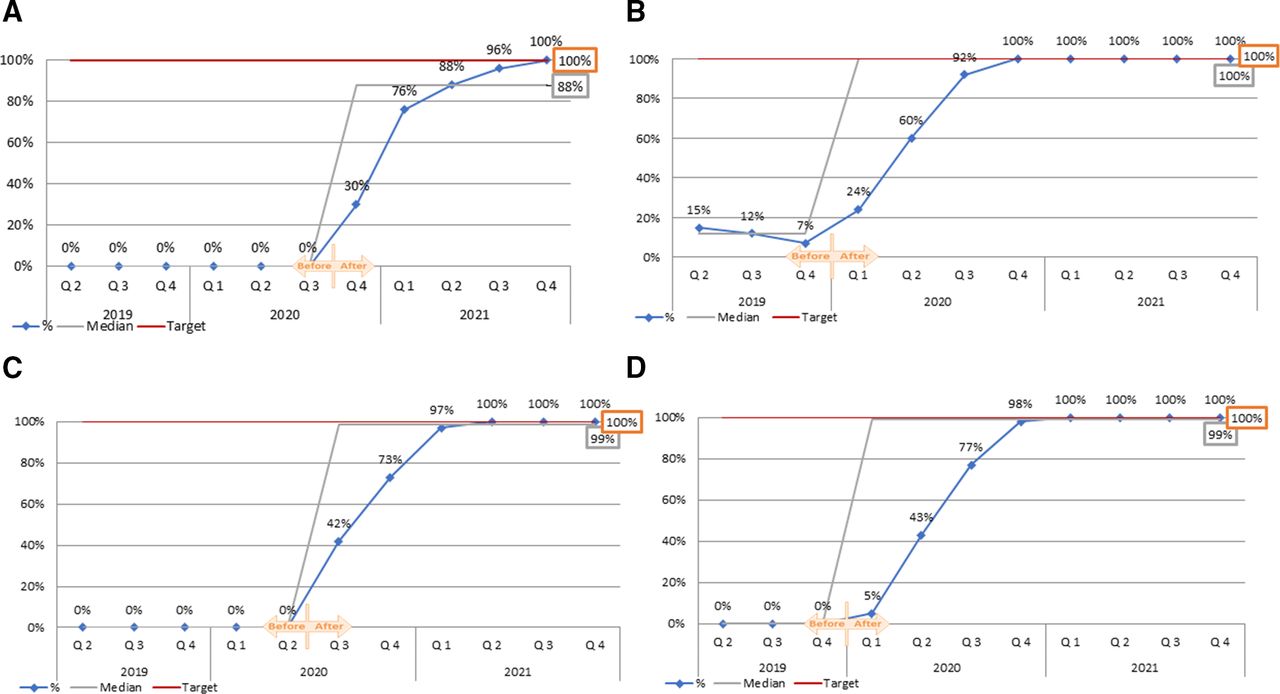
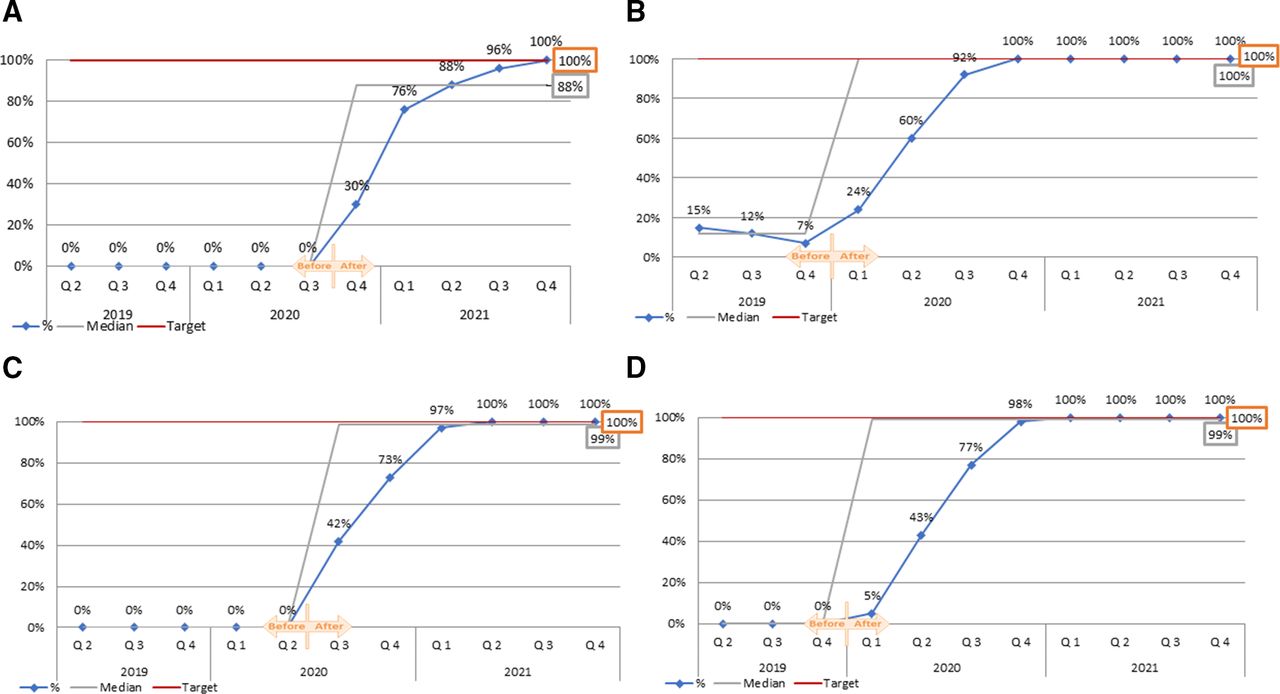
The analysis of the empathy training KPI showed that first positive progress of 30% was in the fourth quarter of 2020, reaching 100% in the fourth quarter of 2021. Likewise, there has been a gradual increase in the KPIs of the PX champions to 100% in the fourth quarter of 2021. In comparison the KPI of leadership–patient interviews was 7% in the fourth quarter of 2019 and gradually increased to 100% in the fourth quarter of 2020. This KPI, equal to 100%, has been preserved onwards. In terms of PX recognition, the first positive progress was recorded in the first quarter of 2020 with a 5% increase, reaching 100% by the first quarter of 2021 and keeping this trend onwards (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
KPI performances 2019–2021. (A) Empathy training, (B) leadership-patient interviews, (C) patient experience champions, (D) recognition of patient experience. KPI, key performance inidcator.
Benchmarking results showed progress more than originally set at 4% (table 5). Despite slightly varying sample size (n), all departments achieved the 4% and exceeded the set-out target by at least 1.5%. This number allowed for a 2-year internal benchmarking for future performance and reporting goals.
Biennially benchmarks set for the KAAB-AFH (2019–2021)
Discussion
The experiences of patients, their families, clinicians and the wealth of evidence on the quality of care in KSA provided the basis for this research project to ensure that services are safe, effective, patient-centred, timely and efficient.12–15 To address this gap, the pilot research project was initiated to explore how to improve the average PX scores in inpatient, outpatient and emergency departments at KAAB-AFH. The standardised HCAHPS survey was administered to address the research aim. However, since HCAHPS and the PX are distinct but related entities, data collection was followed by implementing the six-step PX culture model.
Evidence in the literature suggests a positive relationship between HCAHPS survey response rates and patient satisfaction scores, which was also observed in this study.21 22 At the same time, as in a recent study in seven European countries, the results of the current study highlight that there may be different contributions of specific HCAHPS experiences across different hospitals in the Kingdom. Therefore, future studies are expected to explore in more detail the critical points within and between hospitals that can represent varying PX.21 The findings of HCAHPS served as a basis for the PX culture model for the three departments of the hospital, namely inpatient, outpatient and ER.
In improving PX, one of the first steps was the establishment of the PFAC to promote best practices in the hospital, explore and learn from a patient and family perspective, and promote patient-centred care.22–24 The discussions at the meetings provided significant insights into patients' understanding and concerns regarding primary care delivery. Although most of the topics did not concern clinical decisions, these discussions highlighted the need to improve communication with patients and their families regarding the care process and provided several opportunities for quality improvement. Likewise, Buchanan et al,23 in their study on the importance of patient participation in research, reported that the influence of the research family advisory committee had increased researchers’ awareness of the role of the patient and family in shaping research practice, integrating family-friendly language into communication with patients and informal reports of increase study participation.23
The second step in improving the PX model aimed to improve empathy towards patients through education and a series of training programmes among all staff. This approach was consistent with previous studies, including systematic reviews examining the effectiveness of empathy in general practice, which found an association between clinician empathy and patient satisfaction.25–27 This research observed a direct positive relationship between increased patient support and lowered patient anxiety and distress, leading to significantly better clinical outcomes.24–26 In addition, an earlier study in Korea among 550 outpatients found that physician-perceived patient empathy significantly influenced patient satisfaction and compliance through communication, perceived experience, interpersonal trust and partnership.26 Hence, as found in this research and supported by previous studies, empathy needs to be constantly assessed and improved among healthcare providers in order to improve their communication and patient care.25–27
Since this study aimed at bringing together the best practices, the next step in the model was to recognise the experience of patients, that is, PX with staff named in positive comments are awarded a certificate of appreciation from the hospital director.27–30 It is well established that reward and recognition programmes for healthcare professionals can help employees feel more valued, reduce fatigue, stress and workload anxiety, and motivate them to provide better patient care.29 30 As such, this research supported the evidence that employee motivation and reward, not necessarily financial, can support the efforts of healthcare providers. However, it is very important to consider the needs and requirements of employees that might improve their work conditions, leading to improved patient satisfaction and PX culture.28 31
It has long been believed that the key to a hospital’s success is ensuring that employees know and understand the organisation’s vision and mission.30–33 However, studies conducted among various population groups, including among patients, show that the involvement of the board of directors in the work of healthcare quality management can lead to even better results that meet the mission and vision of the organisation and, most importantly, improve the PX culture. Hence, leaders are an important component of successful healthcare initiatives.32 33 The current research findings showed that leadership–patient interviews to the scheduled weekly leadership safety walk rounds had positive effects among the patients and in improving the quality of care. Consistent with Brown’s study, the results show that hospital management can improve management effectiveness by focusing on key communication and leadership aspects with patients and staff.33
In addition to leadership interviews, PX champions were assigned to each department to work part time to follow up on the implantation of the PX action plans in their area and to share the knowledge and information about PX with healthcare providers in the same area.33–35 This approach has contributed to successful change efforts by creating institutional support for new practices through various engagement initiatives and coordination of care aimed at improving the PX the quality of care. Although there is a lack of studies in this area to allow comparison, the most recent study by Bonawitz et al.35 reported on the importance of the attributes of champions to health change efforts.35 Authors reported six key attributes of champions emerged: influence, ownership, physical presence at the point of change, persuasiveness, grit and participative leadership style.35 These attributes have contributed to the success by enabling champions to bridge institutional fragmentation, build and leverage professional networks, create pressure for change, positive learning climate, optimise compatibility with existing workflow and engage key stakeholders. Hence, future studies in KSA are recommended to not only consider PX champions, but also explore the key attributes of champions that may contribute to even greater change.
The last step in PX improvement model of the current research was the quality improvement. According to Lohr and Schroeder36, ‘the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge’ (p. 1161).36 This includes a systematic and coordinated approach using specific methods and tools with the aim of bringing about a measurable improvement.36–38 As shown in this research, the systematic approach and 6 steps undertaken resulted not only into the quality improvement but also in exceeding the initial target of 4% by at least 1.5% in each department. These results confirmed that quality improvement measurement is an important measure of performance reflecting quality practices, and that comparing the performance of periods and departments will improve the overall performance of the entire facility, that is, KAAB-AFH.35–38
In terms of score differences, the three surveys of inpatient care, medical practice and emergency departments reflect very different PX. Thus, the questions that patients were asked in the three surveys were different, and in each of them, patients had different points of view. This pattern was also consistent with the evidence of previous researchers.39–41 For instance, a study by Krol et al39 found some systematic differences in PX between types of hospital departments in different hospitals. The authors further concluded that these results highlight the importance of analysing qualitative information about inpatient care not only at the hospital level but also at a more specific department level.39 The overall synthesis of the results of this study and previous data shows that while PX is an important outcome of quality of care, patient-reported experiences are the key to improving quality of care. These experiences may vary depending on the patients’ opinions and feelings and the department. Thus, further study of PX, especially in the inpatient department, may be one way for researchers to evaluate patient-reported experiences and examine patient satisfaction, which can provide insight into the gap between expectations and actual experience.
In terms of cost, feasibility and the most essential improvements of the research, out of these six steps, the quality improvement phase was the most expensive, time-consuming and hard to achieve due to structural changes such as improving waiting areas and refurbishing or improving facilities. This was followed by the PX champions step, which required staff members to work overtime to improve patient care quality. Empathy training was organised during the break, conducted by the human resources department and the hospital management, and did not require additional expenses. In contrast, leadership–patient interviews were the easiest and took place during the routine weekly safety walk rounds of the management and took the form of uncomplicated communication, which did not involve any costs. The PFAC consisted of patients, caregivers and staff who worked together to promote excellence in the hospital, which did not require financial support. Lastly, recognition for PX included the certificate of appreciation of conducted work, which did not include any costs and was based on the survey data.
In sum, while there were statistically significant changes and improvements in PX culture and the performance of the medical staff, more work is required to improve PX in inpatient department. These positive changes and set out targets allow to suggest that the team of KAAB-AFH is on the right path of improvements. This approach to research practical changes can serve as a model for future studies in various healthcare facilities of KSA.
Limitations
This was a pilot study in a single facility, which may limit the overall applicability of the PX culture model, but the basic principles described in the model can be applied in other institutions. One of the main limitations of the study was the lack of a dedicated budget to implement changes that target PX priorities. The team has also faced some restrictions due to the COVID-19 outbreak which has affected rounds, training and other activities. More studies will allow comparative evidence. Future research is encouraged to observe associations between outcomes, interventions and relevant contextual elements. The outcome variable (i.e., PX) across departments should be standardised so that better comparisons of improvements across departments can be made. One possible approach can be recruiting both patients and medical staff, and exploring their expectations from the healthcare providers and patients, respectively. Despite the improvements reported in this study and its unique contribution, it did not consider confounding factors and used purposeful sampling, that is, only one healthcare facility. Therefore, it is recommended that future studies include several facilities so that PX culture can be compared across different healthcare settings and how this might affect improvement. Lastly, given the sensitive nature of the data collection process, the government provided only limited access to the survey data, which has been analysed and presented in the paper. As such, no data on the demographic data of participants were provided since this research aimed to improve the overall PX culture; no demographic data were collected, that is, age, gender, SES. Therefore, future studies in different settings may consider collecting demographic data and providing response rates by age and gender breakdown of respondents.
Conclusion
Improving the culture at the healthcare organisation by using a PX culture model was found to enhance the comfort and care of patients in multiple departments. Although the team faced challenges in implementing the action plans due to limitations in resources and budgets, the hospital could achieve the PX targets in all three settings, including inpatient, outpatient and emergency departments. The critical elements for improving the PX and culture included recognising staff, creating networks across the system through effective leadership, employee engagement and engagement of patients and their families.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors NAA developed the research idea and objective, supervised the procedures and drafted the manuscript; MA and OSA collected, processed and analysed data; MHA, NAS structured and designed the manuscript; AW and AAM critically revised and edited the manuscript. NAA accepts full responsibility for the work and/or the conduct of the study, has access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.