Article Text

Abstract
Background Medication administration errors (MAEs) are a major cause of morbidity and mortality. An updated barcode medication administration (BCMA) technology on infusion pumps is implemented in the operating rooms to automate double check at a syringe exchange.
Objective The aim of this mixed-methods before-and-after study is to understand the medication administrating process and assess the compliance with double check before and after implementation.
Methods Reported MAEs from 2019 to October 2021 were analysed and categorised to the three moments of medication administration: (1) bolus induction, (2) infusion pump start-up and (3) changing an empty syringe. Interviews were conducted to understand the medication administration process with functional resonance analysis method (FRAM). Double check was observed in the operating rooms before and after implementation. MAEs up to December 2022 were used for a run chart.
Results Analysis of MAEs showed that 70.9% occurred when changing an empty syringe. 90.0% of MAEs were deemed to be preventable with the use of the new BCMA technology. The FRAM model showed the extent of variation to double check by coworker or BCMA.
Observations showed that the double check for pump start-up changed from 70.2% to 78.7% postimplementation (p=0.41). The BCMA double check contribution for pump start-up increased from 15.3% to 45.8% (p=0.0013). The double check for changing an empty syringe increased from 14.3% to 85.0% (p<0.0001) postimplementation. BCMA technology was new for changing an empty syringe and was used in 63.5% of administrations. MAEs for moments 2 and 3 were significantly reduced (p=0.0075) after implementation in the operating rooms and ICU.
Conclusion An updated BCMA technology contributes to a higher double check compliance and MAE reduction, especially when changing an empty syringe. BCMA technology has the potential to decrease MAEs if adherence is high enough.
- Medication safety
- Anaesthesia
- Healthcare quality improvement
- Patient safety
- Quality improvement
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Medication administration errors (MAEs) cause patient’s harm. Medication double check is introduced to reduce MAE but variation in daily practice results in low compliance.
WHAT THIS STUDY ADDS
Barcode medication administration (BCMA) technology on infusion pumps is implemented to automate double check at pump startup and syringe exchange. BCMA technology showed potential to reduce reported MAEs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Rolling out of automated barcode double check on OK, ICU and the ward may increase patient safety.
Introduction
Medication administration errors (MAEs) are a major cause of morbidity and mortality among hospital patients.1 2 Approximately, 30% of medication errors occur at the administration stage and are often not intercepted.2 Especially high-risk medications dispensed with an infusion pump pose a risk to patient safety.3–5 These medications, such as narcotics, opioids and sedatives, are used in operating rooms daily.
In the past years, there have been several improvements to reduce medication errors. These include pharmacists preparing medication (ie, ready to use and ready to administer), the use of printed labels and the medication double check.6 In the Netherlands, a protocol for safe injectable medication administration has been implemented in 2009, including the double check proceeding.7 However, there is variation in daily practice resulting in low compliance with the double check.8–11 Furthermore, a systematic review by Koyama et al did not show sufficient evidence that double check versus single check of medication administration is associated with lower rates of MAEs or reduced harm.12
The latest development to improve compliance is the use of barcode medication administration (BCMA), in which a barcode reader substitutes the double check by a coworker. Thompson et al found that the introduction of BCMA decreased MAEs by 43% and actual patient harm events by 54%.13 The automation can forestall human error, and therefore, prevent substitution with the wrong medication. Nonetheless, van der Veen et al found that workarounds to BCMA were used in nearly 63% of the administrations to cope with technical shortcomings.14 Koppel et al identified different causes of workarounds, including unreadable medication barcodes and malfunctioning barcode readers.15
The B. Braun Space Infusion Pumps with standardised medication library for operating rooms and ICU were introduced in the Erasmus MC in July 2017. Integration with the electronic health records (EHRs) system provided autodocumentation of administered medication. In July 2019, BCMA technology with barcode readers was introduced in the operating room for infusion pump start-up. Until implementation BCMA cannot be used when changing an empty syringe for a new one. If these shortcomings are solved with a new software, BCMA has the potential to further reduces risks and improves patient safety. However, this improvement can only be realised if there is enough compliance with BCMA.16
To ensure compliance with BCMA, better understanding is needed of how the double check is conducted in daily practice. Within the new safety management perspective Safety-II, the focus has shifted towards learning from what goes right in healthcare. This relates to the system’s ability to succeed under varying conditions.17 18 A central tenet is the understanding that systems and processes are complex, and that human performance is often satisfactory because people are resilient and adjust how they work to changing circumstances.17 19 Hollnagel states that the necessary capacities for resilient performance include the ability to monitor, respond, learn and anticipate.20
The functional resonance analysis method (FRAM) is a Safety-II tool to visualise the functions that make up a process, their interdependencies and the variability that emerges.19 21 22 FRAM helps reveal variability due to possible workarounds or adaptations from protocols that healthcare professionals undertake to ensure patient safety.23 24
Whereas other BCMA studies were about oral medication,13–16 our study is investigating double checking high-risk medications dispensed with new infusion pumps. The updated BCMA technology facilitates conducting the double check for infusion pump start-up and changing an empty syringe solely digitally.24 The double check is performed by the infusion pump software instead of the EHR system, ensuring double check in real-time instead of retrograde approval. An electronic alert is given in case of a mismatch. This before-and-after study aimed to improve the compliance with double check before and after implementation of the new BCMA technology.
Methods
Study design and setting
The study is a single-centre before-and-after study at the Erasmus University Medical Center (Rotterdam, The Netherlands). The study has a mixed-methods design using both qualitative and quantitative methods. Interviews and observations were conducted and reported MAEs were analysed. Observations were done in November 2021 before implementation of the new technology. Implementation began in January 2022 in the operating rooms, including recovery and Post Anesthesia Care Unit (PACU). Postimplementation observations were done from the end of February until the middle of March. The implementation on the Intensive Care Unit (ICU) started at the beginning of May and was rolled out in 2 weeks.
Medication errors
MAEs reported from 2019 to October 2021 were retrieved for analysis of the current situation. MAEs from 2020 to December 2022 were used for implementation evaluation. The incidents were voluntarily reported to the quality management system iProva (Veldhoven, the Netherlands). Trained employees analyse the medication errors with a risk assessment matrix. The matrix combines an estimation of the possible consequences and an estimation of the chance of repetition. A distinction is made between low, moderate, high and very high-risk incidents. MAEs from the operating rooms, recovery, PACU and the ICU department were retrieved for analysis. Incidents with prescription, preparation or storage of medication were excluded, as were omissions and oral medication incidents. Two researchers applied the risk assessment matrix for a second assessment of the remaining MAEs. The incidents were categorised as belonging to moments 1, 2 or 3. These moments correspond with three activities in the operating room:
Bolus induction of medication in the peripheral intravenous line.
Infusion pump start-up.
Changing an empty syringe in the pump for a new one.
A distinction was made between potentially preventable or unpreventable MAEs with the new N06 software. Disagreements were resolved by discussion and consensus.
Qualitative research
The FRAM was used to explore the process of medication administration. The ‘work-as-done’ was defined by interviews with healthcare professionals involved in the medication administration process in daily practice. A topic list based on the FRAM aspects (input, output, precondition, resources, control and time) was used for structuring the interviews.22 Interviews were conducted until the ability to obtain new information had been attained. Each interview lasted approximately 20 min. The interviews were recorded with permission and transcribed. Transcripts were analysed independently by two researchers and the outcomes were visualised in a FRAM model. Each essential function was displayed as hexagon and, if possible, relevant aspects were added: input (I), output (O), precondition (P), resources (R), control (C) and time (T). The coupling among functions can give insight into the variability of the process. Functions with variability in Output can affect the rest of the process. The FRAM model was built using FRAM Model Visualiser software.25 The FRAM outcomes were used to determine the contents of education about the new N06 software, in order to create confidence and prevent workarounds.
Patient and public involvement
A patient who experienced a medication error within the hospital was approached to report her story on video. This video was used for educating employees and raising awareness about medication safety.
Software and barcodes
High-risk medications are dispensed with B. Braun Space Infusion Pumps (B. Braun Medical; Melsungen, Germany) in the operating rooms. There is a unidirectional data flow from the pumps to the EHR system after scanning a medication barcode.
Before implementation, all medications were provided with new and scannable barcodes. Barcodes were standardised for ready to use and ready to administer medication. All barcodes need to be uniform for the specific medicine and concentration instead of manufacturer specific barcodes. This will guarantee that BCMA can be used for all medicines. In January 2022 the new B. Braun software N06 (exclusively available for Erasmus MC) was implemented on the OR, facilitating BCMA at this crucial moment.
Education
In January 2022, employees were educated about the new N06 software. Clinical lessons were provided for all employees. There was a presentation about the N06 software update with short video demonstrations. The importance of double checking and use of BCMA was emphasised. The impact of medication errors was illustrated by the video of a patient who told about her experience. Furthermore, two educated employees provided physical training of the software in the operating rooms. Additional information was provided on the online platform: Ask Erasmus.
Quantitative research
Quantitative research was conducted in the operating rooms to observe adherence to the protocol. Preimplementation data were collected for 4 weeks in November 2021. Postimplementation data were collected for 4 weeks in February–March 2022, 1 month after implementation of the N06 software. The medication administration in the operating rooms was observed by the disguised method.26 Staff was not made aware of the exact aim of the observations. Each observer accompanied the anaesthesiologist assistant or anaesthesiologist who administered the medication and observed all administrations. Observers documented every administration on a data collection form. They noted whether the medication was double checked by a coworker or whether BCMA technology was used. Different types of operations and different healthcare professionals were observed at moments 1, 2 and 3. Observation at moment 3 was only possible if operations lasted longer than 1–2 hours. BCMA was preimplementation only available for moment 2. Postimplementation, it was available for moments 2 and 3.
Data analysis
The observational data from the operating rooms and MAEs were described using descriptive statistics with Microsoft Excel. Differences were tested by a Mann-Whitney test. The percentage of double check was calculated for each operation and each moment. Designing graphs and statistical analysis was performed using GraphPad Prism software V.9.3.1. A p<0.05 was considered statistically significant.
Results
Analysis of reported MAEs
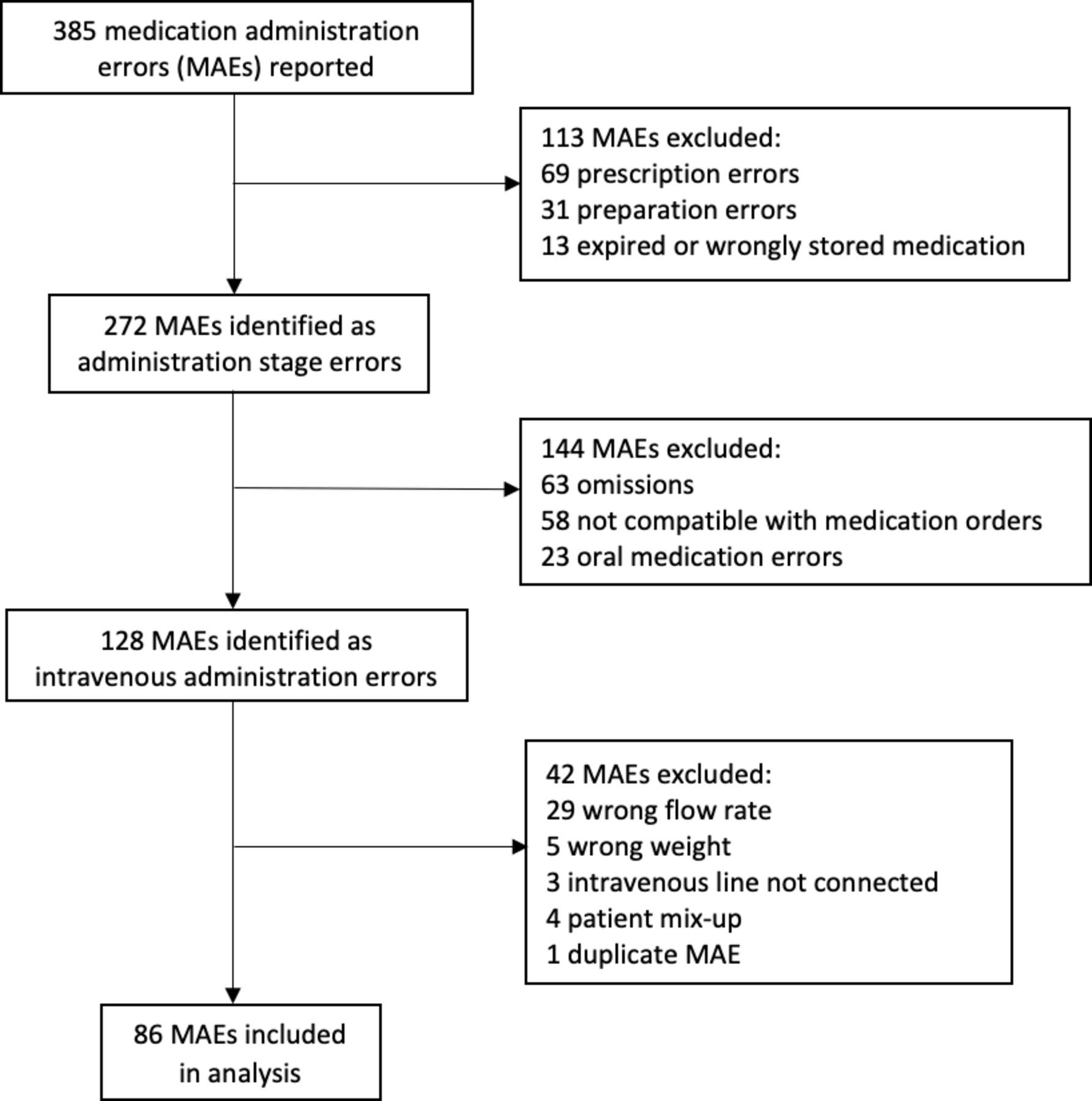
A total of 385 MAEs in the operating rooms, recovery, PACU and the ICU department were reported between 2019 and October 2021. After application of the exclusion criteria, 86 incidents were analysed (figure 1). Of the 86 MAEs, 22.1% belonged to moment 2 and 70.9% belonged to moment 3. The moment 1 incidents were excluded for further analysis, because they were not related to the infusion pump software.

Flow chart of MAEs selection between 2019 and 2021 in OR, PACU and recovery. OR, operating room. PACU, post anesthesia care unit
Almost 4% of the moments 2 and 3 MAEs were classified as very high risk. Most of the MAEs, 65.0%, potentially posed a high risk to patient safety. 27.5% of MAEs were classified as moderate risk. Ninety per cent of the moments 2 and 3 incidents were deemed preventable by the N06 software. MAEs about wrong weight registration in the infusion pump are not preventable with BCMA, but the N06 software has an extra function that shows a pop-up to confirm the right weight after restarting the pump.
Qualitative research
We conducted 10 semistructured interviews with employees with different professions in the operating room: two anaesthesiologists, one resident, six anaesthesiology assistants and one student anaesthesiology assistant. Functions in the process of medication administration were identified. Subsequently, they were linked by the different aspects. It was an iterative process with several adjustments while constructing the model.
Figure 2 shows the FRAM based on the interviews. The model represents the entire process from medication order to registration in the EHR system. Hexagons concern functions and lines concern couplings. The red functions are executed by the first employee and the blue functions are executed by a second employee. The model consists of 10 functions of which 2 foreground functions show the options for medication registration in the infusion pump: <select medication manually> and <scan barcode>.

FRAM model of medication administration in the operating room. EHR, electronic health record; FRAM, functional resonance analysis method.
Select medication manually
An anaesthesiology assistant selects medication from the medication library (resource). Ready to use medication is taken, or medication is prepared by an anaesthesiology assistant who puts a medication sticker on the syringe. A coworker needs to confirm that the pump display corresponds with the medication in the syringe. This is only possible if a coworker is present (precondition). Time influences the selection of the correct medication, as one needs to manually scroll through the alphabetical library.
Scan barcode
Ready to use medication is taken, or medication is prepared by an anaesthesiology assistant who puts a medication sticker on the syringe. Double checking this medication is only possible under the precondition that a coworker is present. If barcode scanning does not work, multiple attempts are necessary, which takes time. BCMA is only possible under the precondition that: the barcode is scannable. The medication library is a resource for this function. Medication in the infusion pump can be confirmed by either the first or second employee.
Variability in the process is mainly found in the manual preparation and selection of medication. Two double checks by a coworker are needed, which is not always done. Reasons are being unaware of the protocol and the absence of a coworker. The BCMA process does not require the presence of a coworker and automatic registration in the infusion pump is faster than manual selection. However, different reasons for workarounds to BCMA were identified. The first workaround was based on working efficiently in order to save time. Some employees found scanning takes too much time, especially if scanning does not work immediately and would therefore choose manual selection over barcode scanning. Reasons why barcode scanning may take too much time included: not all barcodes being known in the library and some did not provide a corresponding medication name and concentration. In addition, barcodes were sometimes unreadable. The barcode sticker needs to be well printed with enough ink, unwrinkled and in the right position on the syringe in order to be scannable while in the infusion pump. The second workaround was based on a lack of knowledge, some employees were not aware of the BCMA protocol or were not educated on using the barcode reader. Finally, some are used to their own way of working with the medication library and not willing to adept, until all barcodes are guaranteed scannable. The interviews revealed that employees who experienced a medication error were more aware of the double check procedure and were more likely to use BCMA.
Quantitative research
Preimplementation, a total of 49 operations were observed in 104 hours. Postimplementation, 29 operations were observed in 65 hours. In either situation, most observations were done for moment 1, followed by moment 2 and the least for moment 3. Table 1 shows the number of operations an amount of medication administrations and if and how the double check was conducted for each moment before and after the implementation.
Rates of compliance with the double check procedure before and after implementation of the N06 software
For moment 1, the double check was 90.1% and this increased to 94.1% after implementation. The new software has no impact on this moment, however. Moments 2 and 3 both showed an increase in the amount of double checking. The double check (by coworker and BCMA) for moment 2 changed from 70.2% to 78.7%, but the change was not significant (p=0.41). Preimplementation BCMA was performed in 15.3% pump start-ups and increased to 45.8%. There is a significant (p=0.0013) increase in the use of BCMA for moment 2. There is a shift visible from double checking by a coworker to double checking by BCMA.
For moment 3, the changing of a syringe, the double check significantly improved from 14.3% to 85.0% (p<0.0001). The largest contribution is the use of BCMA, which is used in 63.5% of administrations, but the double check by a coworker also increased.
Education
Eighty-two operating room employees attended the physical training of the N06 software preimplementation. This is 50.1% of the total employees. The other employees were trained on the job by their coworkers’ postimplementation.
Follow-up MAEs
After implementing BCMA in the operating rooms, BCMA was implemented in the ICU from early to mid-May 2022. Figure 3 shows a run chart of MEA’s over the last 3 years. From May to December 2022, a median of 11 MEAs (IQR 10–14.75) were reported monthly compared with 11.5 MEAs (IQR 9–14) (p=0.54) in the preimplementation period from January 2020 to December 2021.However, the median amount of MEAs concerning infusion pump start-up and changing an empty syringe (moments 2 and 3) significantly (p=0.0075) reduced from 2 (IQR 1–3) to 1 MAE/month (IQR 0–1.25) postimplementation.

{kind=link}
{kind=link}
{kind=link}
Runchart of all reported MAEs and MEA’s concerning infusion pump start-up and changing an empty syringe (moments 2 and 3). The software was implemented in January in the OR and in May in the ICU. BCMA, barcode medication administration; MAEs, medication administration errors; OR, operating room. ICU, intensive care unit
Discussion
Principal findings
The FRAM model illustrates the process of starting up an infusion pump in the operating room. It shows variation and contextual factors that may cause variation. Through the interviews, different reasons for workarounds to double check and BCMA were identified. The most important reasons were unreadable barcodes, lack of time and hesitance to adapt. Concerning the last reason, healthcare workers like to stick to old habits and sometimes do not see the urgency to change. Earlier studies indicate that guideline adherence is not high without specific intervention, but certain interventions (typically multifaceted and resource-intensive ones) improve adherence.27
Before implementation of the N06 software, the underlying reasons for workarounds were eliminated as much as possible. All medications were provided with new and scannable barcodes. This will guarantee that BCMA can be used for all medicines. If some medication is not scannable, people are resistant to change. In addition, time is an important factor in vasoactive medication. BCMA will extend the interruption for changing a syringe. Working with two pumps with vasoactive medication at the same time would overcome this issue. The findings contributed to a good implementation by education and building confidence in the system. This enhanced the willingness to use BCMA technology, and therefore, steer clear of possible workarounds.
The analysis of MAEs gave insight into the seriousness of the problem and the crucial moments in the process. The results showed that 70.9% of MAEs occurred at moment 3, which often led to potentially high-risk and very high-risk incidents. The changing of an empty syringe accordingly seems to be a crucial moment. The implementation of the software has the potential to improve safety, as 90% of the moments 2 and 3 errors were deemed preventable. However, MAEs cannot be completely eliminated by BCMA as errors can still occur with preparation and prescription of the medication. The next step to increase medication safety would be to solely use ready to administer syringes.
The before-and-after observations in the operating rooms were done to evaluate the implementation of the software. In general, the protocol adherence to double check improved after the implementation for all moments. Before implementation, double check for moment 1 was already performed in 90.1% of the cases. It is better than the 52% double check by second nurse described by Schilp et al.11 A plausible explanation is that when bolus medication is administered for induction of anaesthesia, both the anaesthesiologist and the anaesthesiology assistant are present. In the clinic, a healthcare worker should be asked to perform the double check. Since the double check for moment 1 has increased to 94.1%, while the new software has no influence at this moment, the increase must be due to an increased awareness of the importance.
Furthermore, the double check for moment 2 changed not significantly. This could be explained by the shift from checking by coworker to double checking by BCMA. BCMA adherence significantly increased to 45.8%. For moment 3, BCMA was only postimplementation available and was used in 63.5%. In addition, the double check by a coworker also increased, adding up to a significantly higher total of 85.0%. This increase could also be a result of improved education or the facilitated process. Unfortunately, we were not able to increase the adherence rate to 94.4% as described by Thompson.13 There is however still room for improvement of BCMA adherence rates. The goal is to conduct the double check solely digitally, which makes the presence of a coworker unnecessary.
The run chart of MEAs over the last 3 years showed a significant reduction of MEAs concerning infusion pump start-up and changing an empty syringe post implementation. As a result of changing the label of vasoactive medication, the barcode code was no longer scannable in autumn 2022. A workaround with a scannable label on the plunger holder was created. This resulted in two MAEs for moment 3 on both October and November. Since then scanning is possible again. This workaround showed the importance of staying resilient.20
In context of literature
The findings of the study are in line with other studies on BCMA.13–16 28 Workarounds are primarily caused by unreadable barcodes and malfunctioning barcode readers.15 This causes distrust in the system. Identification of workarounds is essential to implement better software which fits the workflow in practice. van der Veen et al state that the nurse workload was a potential risk factor associated with the workarounds.14 BCMA can avoid this risk factor, as it is faster than a manual double check, and it can be performed without the presence of a coworker. Ideally, BCMA helps confirm the five ‘rights’ of medication administration: right patient, drug, dose, route and time.15 BCMA has the potential to reduce administration errors, except for wrong time errors. However, these errors are considered less clinically significant.28
A competent medication administration process functions under varying conditions. Hollnagel states that resilient performance is possible for systems, if the four necessary abilities are present.29 These four abilities are: the ability to respond, monitor, learn and anticipate. Monitoring means being able to monitor the system’s performance and what affects it. Without monitoring, the system must constantly be able to respond to every possible situation, which is not sustainable. If the process of double checking medication administrations is monitored, one can learn from it and improve the process. Continuous measurements of BCMA adherence can help to indicate the safety of the process. Unfortunately, at the moment, there is no dashboard for monitoring the BCMA adherence available, but it will be in the near future.
Strengths and limitations
A strength of the study is the combination and timing of qualitative and quantitative research. The education on the N06 software was adapted to the findings of the FRAM. Possible problems, such as unreadable barcodes and hesitance to adapt, were anticipated to ensure higher adherence rates. The observations before and after implementation showed an increase in BCMA adherence. Lastly, MAEs concerning infusion pump start-up and changing an empty syringe (moments 2 and 3) reduced significantly.
Nonetheless, the study has some limitations. There might have been interobserver variability with the observations in the operating rooms. This was probably limited by clearly defining the categories for observation (moments 1, 2 and 3). There was consensus about noting the double check positive after nodding, as there was no verbal confirmation in most observations. There was no dashboard available to show the exact BCMA adherence rates. Therefore, the observations are only an indication of the real numbers. Since observations were recorded manually, the sample size of the study is small, especially for moment 3.
In addition, the FRAM model only shows the main routes of the complex medication administration process. Many different factors are involved, which may cause more natural variations in practice than illustrated in the FRAM model. Furthermore, the generalisability and sustainability of the study may be limited because of the monocentric setting with implementation in the operating rooms and ICU. Results can be different when implementing the software in other hospitals or departments.
Finally, reported MEAs represent only a fraction of all medication errors and should be viewed with caution.
Further research
To show the exact BCMA adherence rates, a dashboard for monitoring is necessary. Future analysis of reported MAEs can show if there is a sustainable reduction in number and seriousness of incidents. The increase of double checking was a result of the new software together with a behavioural change. It would be interesting to conduct interviews again and explore if and why there are still workarounds to BCMA after implementation.
Conclusion
Taking into account both our findings and the findings of previous studies, BCMA technology has the potential to decrease MAEs. Most MAEs occurred with the changing of an empty syringe, often leading to potentially high-risk incidents. This moment particularly has shown a significantly increased double check after implementation of the new technology. Adherence to BCMA can be increased through education and raising awareness about the damaging effects of medication errors. This increased awareness in the occurrence of medication errors, in combination with an updated BCMA technology, can optimise medication safety in the operating rooms.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The local Medical Ethics Review Committee reviewed the research proposal (reference number MEC-2021-0903). Interviews and observations were performed with consent from respondents.
References
Footnotes
Contributors All authors meet all four ICMJE criteria for authorship. MH: design of the study, data acquisition, analysis, interpretation of the data, drafting and revising the manuscript. MS: analysis, interpretation of the data, revising the manuscript. LvD: analysis, interpretation of the data, revising the manuscript. MF: data acquisition, analysis, interpretation of the data, revising the manuscript. NK: design of the study, Implantation of software, revising the manuscript. SEH: design of the study, analysis, revising the manuscript. RB: design of the study, interpretation of the data, revising the manuscript. MtH: design and guarantor of the study, data acquisition, analysis, interpretation of the data, drafting and revising the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.