Article Text

Abstract
Introduction Wound care is a multibillion-dollar industry, and most research and treatment are geared towards late-stage or end-stage care. The longer a patient has a wound, the more likely it is that complications (like sepsis or vascular compromise) will occur that will both extend treatment and multiply costs. We postulated that much of the suffering and healthcare costs of chronic wounds could be avoided by early identification of high-risk patients and subsequent earlier intervention. In an established regional wound clinic, our aim was to decrease referral times by 50% within 1 year, and to demonstrate the beneficial outcomes on wound healing and total cost of care.
Methods A prospective interventional quality improvement study was performed between June 2017 and June 2018. We determined baseline referral times to the clinic and then performed three interventions. The effects on referral time, healing time and number of home care visits to achieve wound healing were collected and displayed on annotated control charts. The cost of care and potential for cost avoidance was determined by an analysis of the medical encounters of twenty chronic wound patients.
Results We achieved a 53.6% reduction in average referral times to the clinic, a 59.6% reduction in average healing times and a 66.0% reduction in the average number of home care visits required to achieve healing. Our cost analysis suggested the potential for significant cost avoidance (87.7%) compared with delayed treatment outside the clinic.
Conclusions Early identification and treatment of patients at high risk for wound chronicity and complications, followed by early referral to and treatment at a specialised wound clinic, resulted in faster healing and reduced health system costs.
- quality improvement
- control charts/run charts
- primary care
- home nursing
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The treatment of chronic and complicated wounds is difficult, associated with serious complications, and expensive to the health system. Most research focuses on advanced modalities that could expedite healing.
WHAT THIS STUDY ADDS
Early identification of high-risk wound patients, followed by early referral to specialised care results in faster healing and the potential for enormous cost avoidance.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
While specialised wound care is often reserved for complicated, chronic or advanced stage wounds, this study shows that early (or even preventative) intervention by wound specialists leads to better outcomes and cost avoidance for high-risk patients.
Introduction
Problem description
Chronic wounds represent a significant burden for patients, families, caregivers and healthcare institutions.1 2 Wounds cause pain, suffering, loss of function, lead to social stigma and are associated with a loss of personal identity3 4 and psychological distress. Patients with chronic wounds often have comorbid states that contribute to their impaired healing (vascular disease, diabetes, impaired sensation, etc). These conditions can require referral to multiple specialists or services with the potential for delays in diagnosis and treatment. The longer a wound persists, the more likely it is that complications will occur (including infection and sepsis) which can increase the cost of treatment several fold.
Available knowledge
Wound chronicity is, in many circumstances, avoidable. A common tenet in wound care suggests that early diagnosis and treatment leads to earlier healing.5 Conversely, an undiagnosed contributing condition (such as diabetes, immunosuppression or vascular disease) can make wound healing impossible.6 7 Patients with these conditions are at high risk for wound chronicity and subsequent complications.
Rationale
Complex patients at elevated risk for delayed wound healing are usually identifiable. If these patients can be ‘fast-tracked’ into specialised wound care, including optimisation of contributing comorbidities, their wounds will heal faster. This will lead to a shorter course of wound care, fewer complications and, ultimately, reduced cost.
Specific aims
The aim of this study was to reduce referral times to the Fraser Health Complex Wound Centre (CWC) by 50% within 1 year (by June of 2018). We anticipated that earlier assessment of wound patients within our multidisciplinary wound care practice environment would lead to the earlier initiation of treatment and commensurate faster healing times and decreased cost.
Methods
Context
The Fraser Health Authority (FHA) is the largest of several health authorities in British Columbia responsible for the healthcare of 1.8 million residents. This study was performed within the context of the Fraser Health CWC. The CWC is the sole outpatient programme within FHA with a specific focus on complex lower limb wounds (predominantly venous stasis ulcerations and diabetic foot ulcers).
The CWC is an interprofessional practice environment providing comprehensive wound care to patients within the FHA. An evaluation of our patient population and treatment statistics in November 2017 suggested average referral times of 205 days and average healing times of 182 days. These results were unacceptable to our clinical staff and leadership.
Interventions
Given our hypothesis that earlier referral would lead to earlier diagnosis, treatment and healing, our interventions were focused on the expedited identification of patients at high risk for wound chronicity followed by immediate referral to the CWC. We wanted to see at-risk patients (targeting those with diabetes, peripheral vascular disease and patients with a history of slow-healing wounds) earlier in their medical wound experience including both acute and subacute wounds.
Three main interventions were designed.
Home care office visits. Half-day visits to all regional home care offices were performed by the CWC physician lead (JMH) between June and August 2017. These visits focused on discussion with staff around the challenges of chronic wound care, perceptions of the role of the regional CWC and impediments to timely referral of complex wound patients. Specifically, home care office staff and leadership were asked to immediately refer patients with a lower limb wound with risk factors for slow wound healing including: a history of diabetes, vasculopathy (including venous stasis or arterial insufficiency) or slow-healing wounds to the CWC. Follow-up correspondence with home care office wound care clinician nurses was performed over the phone by designated CWC wound care clinicians.
Family physician engagement letter. The CWC primary care referral base prior to August of 2017 was exclusively chronic (greater than 3 months) home care wound clients. In August 2017, a new rules of engagement letter was sent to all regional family practice offices to advertise the CWC. Specifically, family physicians were encouraged to refer patients with lower limb wounds and a history of diabetes, vasculopathy (including venous stasis or arterial insufficiency) or slow-healing wounds without delay to the CWC. The CWC physician lead (JMH) also performed a few large-group FP office visits to reinforce the concept of early referral of high-risk patients.
In September of 2017, we circulated a new CWC referral form (both online and physical forms). These forms were made available to family practice and specialist offices as well as to regional home care services. This referral form emphasised the importance of early referral of patients with lower limb wounds and a history of diabetes, vasculopathy (including venous stasis or arterial insufficiency) or slow-healing wounds to the CWC.
Following patient assessment at the CWC, appropriate investigations and referrals were made in a similar fashion to our practice prior to this quality improvement initiative. The majority of day-to-day wound care was still performed by regional home care services although under the direction of and in collaboration with the CWC.
Study of interventions
We studied our baseline data on referral times, wound healing times and home care visits to achieve healing. A year of baseline data suggested the presence of a stable system (figures 1–3). This stability of background data allowed for rapid detection of special cause variation based on our interventions.

Referral time to CWC from initial medical encounter for wound assessment. CWC, complex wound centre.

Time to wound healing after first CWC assessment. CWC, complex wound centre.
{kind=link}
{kind=link}
{kind=link}
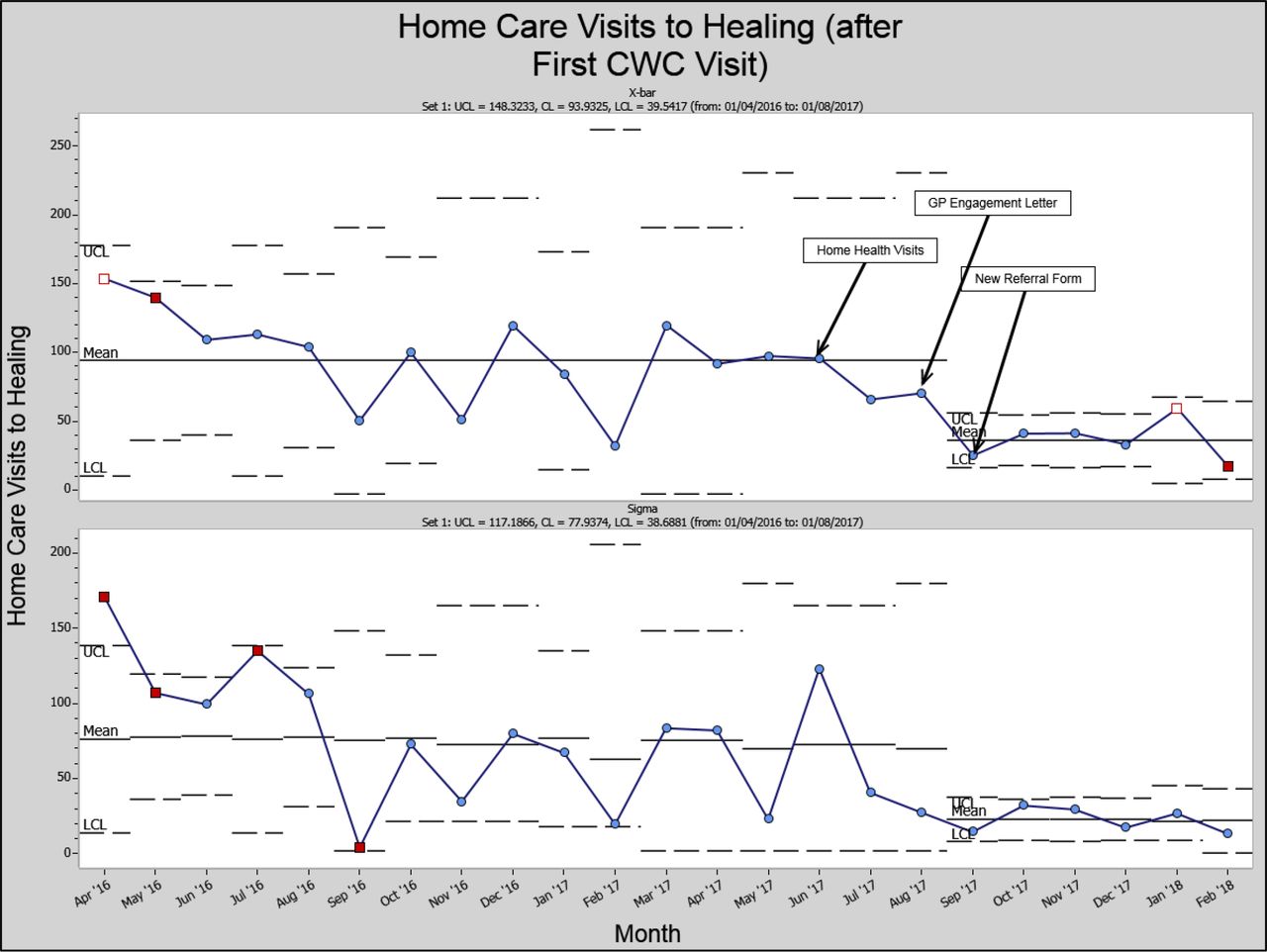
Number of home care visits to achieve wound healing.
The financial impact of care provided at the CWC was calculated through an assessment of the medical encounters of a cohort of 20 CWC patients. Using the FHA electronic medical record, all documented appointments for wound care, wound assessment or treatment of wound complications were identified from the start of the wound through to healing. Medical interventions at each encounter (including consultation, imaging, wound care, antibiotics, emergency care, etc) were noted and costs assigned according to databases available through the FHA finance department and government websites (provincial government of British Columbia and the Canadian Institute for Health Information). In collaboration with a student and faculty from the University of British Columbia Sauder School of business, we compared the costs of treatment both before and after CWC assessment and were able to estimate cost avoidance.
Measures
The primary outcome measure for this study was the referral time to the CWC. This was defined as the time between the patient’s first documented medical encounter for wound care (usually by their family physician but occasionally through home care services or emergency departments) and the date of their first CWC appointment. This was collected from the regional home care database (Pixelaire) which is also used at the CWC.
Wound healing time was defined as the time between the first CWC assessment and the first documented date of healing (as determined by a physician, wound care clinician nurse or home care nurse). These data were collected via the home care database (Pixelaire) but occasionally required paper chart review or review of the electronic medical record (Meditech).
As most of the day-to-day wound care was still performed by regional home care services after CWC assessment, we also measured the number of home care visits that were required between the time of the first CWC assessment and documented wound healing.
Measurement of cost of care and estimation of potential cost avoidance was described above.
Analysis
Annotated control (x-bar and s-bar) charts were used to evaluate for special cause variation in referral times, wound healing times and the number of home care visits until healing.
The evaluation of the impact of care on cost was difficult given a paucity of case-costing data. We attempted to use the lowest cost estimate available and exhausted local data prior to using provincial-level or national-level cost estimates. This method excludes costs for medical encounters outside of the electronic medical record, for personal financial costs or for societal costs (caregivers, family time, loss of work, etc). Our generated figures were compared with those from the literature8–10 (eg, estimated care costs in the literature for patients with diabetic foot ulcers, pressure sores or venous stasis ulcerations), and we found that our estimates were within those found in the literature.
No conflicts of interest were identified by any of the authors.
Informed consent was attained by the CWC physician lead for all surveys. Surveys did not include any patient identifier data.
All data were stored on a secure FHA server with all patient identifier data removed prior to data extraction.
Patient and public involvement
It was assumed that shorter wound healing times and fewer home care visits to achieve healing (two of the main outcome measures of this study) would be associated with improved patient experience. Indeed, surveys administered at the CWC suggest that patient experience is very positive while at the CWC and improved when compared with pre-CWC experiences (the results of these surveys are not provided in this article).
No patient-identifying data were recorded for this study. Patients were not directly involved in the design of this study, although a patient advocate was part of the teaching faculty of Physician Quality Improvement programme that this study was supported by. Patients were not involved in the recruitment to or the conduct of this study. As no patients were recruited for this study, no plan is in place for the dissemination of results to study participants.
Results
A decrease in average referral time was identified from September 2017 to February 2018 (95.2 days) compared with April 2016 to August 2017 (205.0 days) representing a 53.6% decrease in referral times (figure 1).
A decrease in average wound healing times was identified in patients first assessed at the CWC from September 2017 to February 2018 (73.3 days) compared with patients first assessed at the CWC from April 2016 to August 2017 (181.6 days) representing a 59.6% decrease in wound healing times (figure 2).
A decrease in average home care visits for wound care was identified in patients first assessed at the CWC from September 2017 to February 2018 (104.0 visits) compared with patients first assessed at the CWC from April 2016 to August 2017 (35.4 visits) representing a 66.0% decrease in home care visits to wound healing (figure 3).
All three control charts (figures 1–3) suggest a temporal relationship between the aforementioned interventions and special cause variation demonstrating improvement.
Our assessment of 20 CWC patients revealed an average cost per patient of US$47 487.88 prior to assessment at the CWC. Within the cohort, there was a large difference in costs of care between diabetic foot ulcer (DFU) patients (eight patients) which averaged US$62 589.90 while venous stasis ulceration patients (seven patients) averaged of US$28 312.34 (table 1).
Costs of chronic wound care and estimated cost avoidance using CWC model
After assessment at the CWC, patients costed an average of US$5827.08 (12.3% of the previous expenditure to achieve wound healing—an estimated cost avoidance of 87.7%). DFU patients costed an average of US$3980.75 (estimated 93.6% cost avoidance). Venous stasis ulceration patients costed an average of US$3936.88 (estimated 86.1% cost avoidance) (table 1).
We anticipated, with an expansion of our referral base to family practitioners and a call to refer complex wound patients earlier in their wound experience, that CWC waitlists might increase, also increasing our referral times. During the interval of this study (June 2017 to June 2018) we did not experience an increase in our waitlist.
Discussion
Summary
We were able to accomplish a 53.6% reduction in average referral times to the CWC. Consistent with our hypothesis that earlier referral, assessment and treatment would lead to faster healing and fewer treatments, we also observed a 59.6% reduction from baseline in wound healing times and a 66.0% reduction in home care visits required to achieve healing.
We demonstrated a potential for cost avoidance in our complex wound treatment model (an average of US$41 660.80 per patient) when compared with the current system in the FHA. While this observed cost avoidance was not specifically linked to this study’s interventions, it is reasonable to assume that more improvements to expedite wound healing would further reduce the number of medical encounters for wound care, the number of wound complications and the overall cost of care.
Interpretation
The project rationale was firmly grounded in well-accepted wound care dogma: early treatment equals fewer complications and earlier healing.5 We made changes in our referral process to attract high-risk wound care patients earlier in the patient experience. Assuming our interventions were successful, the anticipated results (faster healing times and cost avoidance) were, we felt, assured.
In our own experience at the CWC, chronic wounds are usually the result of patients not receiving a clinical standard of care or concurrent treatment of contributing comorbidities in a timely manner. This is not to say that other local or regional wound care resources are incapable of providing service. More likely, there are multiple health system and socioeconomic barriers that prevent patients from accessing all necessary services including a lack of attachment to a primary care provider. As a specialised wound clinic, the CWC has standardised clinical pathways and expedited referral networks that mitigate against patients falling through the cracks.
Another interesting observation was the magnitude of the estimated cost savings generated by care at the CWC. While our raw data suggests that wound care healing times can be reduced by between 30% and 60% compared with therapy outside of the CWC, the magnitude of estimated cost avoidance was greater—an average of 87.7% for all patients and 93.6% for patients with DFU. A cursory evaluation of the cost analysis data reveals that ongoing costs of wound care (eg, dressing changes and home care visits) can be done at minimal cost. Most of the cost avoidance seen in this study comes from the avoidance of wound complications such as infection, sepsis and amputation. For example, we know that DFU are associated with a 15% lifetime risk of amputation, and a doubling of 5-year mortality when compared with non-DFU diabetics even when accounting for their higher risk of cardiovascular events.11 This conveys some urgency to the problem of chronic wound care. The longer wounds stay unhealed, the more likely it is that patients will develop a serious wound complication. These complications cause additional suffering and cost to the medical system and can be avoided as we have shown.
Limitations/conclusions
A limitation of this study is the lack of sustained data beyond 2018. Data concerning wound healing rates (date of wound initiation, time of first medical encounter, time of wound closure) was manually extracted from patient charts and/or documentation from multiple patient databases by a designated research student who was unavailable after the end of the study. The clinic was also closed for a period of almost 6 months in the initial stages of the COVID-19 pandemic. Our absence of wound healing data beyond 2018 highlights the difficulties of performing wound research and quality improvement including our lack of a wound database or a unified patient electronic medical record in our health jurisdiction.
With that being said, administrative data suggest that our clinic waitlists and time from referral to initial consultation have not increased since 2018 and, anecdotally, it seems that referral patterns for early consultation of high-risk wound patients are similar.
An ongoing challenge has been identifying exactly what we are doing at CWC that leads to faster wound healing compared with pre-CWC care. Indeed, the CWC does not have access to advanced wound care modalities that are unavailable elsewhere in the health authority. One possibility is the presence of a physician with wound care training, which is a relative rarity. Another possibility is increased experience in selected wound care entities, specifically DFUs and venous stasis ulcers which make up approximately 90% of the CWC practice. Finally, the CWC has developed relationships and expedited referral pathways to wound specialists (eg, infectious disease physicians, vascular surgeons, plastic surgeons, dermatologists, orthopaedic surgeons), which may further decrease time to needed treatment. The spread of the CWC model of care will be the main subject of a future QI study.
By proactively identifying patients at high risk of wound chronicity quickly after initial injury and then expediting care in an experienced wound care setting, we have shown that quicker healing and reduced cost is possible. The results of this study should be widely generalisable, even in the absence of a multidisciplinary complex wound clinic. Experienced and specialised care may come from a specialty clinic, specialist, wound care clinician nurse or even another practitioner with an interest in wounds. The care should be coordinated, control contributing risk factors, and be meticulous and consistent. And this care should begin as soon after initial injury as possible. If we wait for patients to develop chronic wounds (>3 months), the wounds are more difficult to heal, are at risk of developing complications and will cost much more.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Prior to initiation of this project, we generated A pRoject Ethics Community Consensus Initiative (ARECCI) score, a web-based ethics screening tool developed in Alberta, Canada. Initial screening generated a low score suggestive of minimal risk. As such, a formal research ethics board approval was not required by the Fraser Health Authority.
Acknowledgments
This project was performed as part of the Fraser Health Physician Quality Improvement Program (PQI). The PQI Initiative is a collaboration between the Fraser Health Authority, British Columbia Mistry of Health and the Specialist Services Committee, Doctors of BC.
Footnotes
Contributors JMH is the sole author and also the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.