Article Text

Abstract
Background Adherence to pharmacotherapy is crucial to prevent symptom deterioration in chronic diseases. However, non-adherence to chronic treatments is prevalent, especially in polypharmacy. Practical tools to assess adherence to polypharmacy in primary care are missing.
Aims We aimed to develop an Adherence Monitoring Package (AMoPac) for general practitioners (GPs) to identify patient non-adherence. We tested the feasibility and acceptance of AMoPac in the primary healthcare setting.
Methods AMoPac was developed based on peer-reviewed literature. It consists in (1) electronic monitoring of patients’ medication intakes for 4 weeks, (2) receiving feedback on intake behaviour by the pharmacist and (3) generating an adherence report to communicate to the GPs. A feasibility study was conducted with heart failure patients. GPs’ acceptance of AMoPac was explored with semistructured interviews. Electronic transmission of the reports into the GP’s electronic health record along with laboratory reports stating N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels was analysed.
Results We developed AMoPac and tested its feasibility with six GPs and seven heart failure patients. GPs were satisfied with the adherence report including the pharmaceutical-clinical recommendations. Integrated transmission of adherence reports to GPs was not feasible due to technical incompatibilities. Mean taking adherence was 86.4%±12.8% and three patients had low correct dosing-days (69%, 38% and 36%, respectively). NT-proBNP ranged from 102 to 8561 pg/mL and four patients had elevated values (>1000 pg/mL).
Conclusion AMoPac is feasible in the primary healthcare setting, excluding the integrated transmission of adherence reports to GPs. The procedure was highly accepted by GPs and patients. AMoPac fills a gap by combining clinical values with adherence data, and therefore, delivers a multifaceted picture of the patient’s behaviour. In case of unmet adherence, our tool might facilitate the selection of patient-centred approaches to optimise pharmacological therapies in chronic heart failure patients.
Trial registration number NCT04326101.
- Polypharmacy
- Compliance
- Chronic disease management
- General practice
- Pharmacists
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Heart failure patients face complex treatments including polypharmacy. Non-adherence is a common issue, but practical tools to assess intake behaviours are missing.
WHAT THIS STUDY ADDS
We present an Adherence Monitoring Package, a comprehensive tool to guide general practitioners’ interpretation of patients’ individual adherence profiles.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
In case of unmet adherence, our tool might facilitate patient-centred approaches to optimise pharmacological therapies in chronic heart failure patients.
Introduction
Adherence to pharmacotherapy is a key element to achieve adequate outcomes. The complexity of strengthening medication adherence has been recognised over the last decades.1 In practice, a shift from paternalistic physician–patient relationship has occurred toward shared decision-making concepts. Patient and physician establish a partnership and a level of communication that is confident and stable to select the right treatment.2 Nevertheless, general practitioners (GPs) tend towards overestimating patients’ adherence, generally because of a lack of reliable tools to assess medication (non-)adherence in daily practice.3 Knowing patients’ adherence profiles could guide GPs when evaluating clinical outcomes and prevent the worsening of chronic diseases such as heart failure.4
Medication adherence can be computed from electronic data that deliver corresponding estimates. Among several proposed estimates, the three most comprehensive are taking adherence (=percentage of intakes during the observed period), timing adherence (=percentage of intakes within a given grace interval (eg, ±2 hours) during the observed period) and drug holidays (=no intakes on several consecutive days, mostly 3).4–6 These estimates deliver distinct aspects of patients’ intake behaviour. Many studies revealed alarming percentages of patients not taking medication as prescribed, including late or no initiation, erratic implementation or early treatment discontinuation.4 5 Medication errors such as non-adherence could lead to disease worsening, hospitalisation and increased healthcare costs, among others.7 Increasing medication adherence effectively improves health outcomes. It is therefore essential to examine any signs of deviating intake behaviour.8 Electronic monitoring is the gold-standard method when investigating the implementation of pharmacotherapy into daily life.4 9 Other methods such as assessing patients’ medicine refills can serve as a proxy for GPs with self-dispensing licence. Out of 26 cantons in Switzerland, 17 allow GPs to dispense medicine directly to their patients. This unique arrangement was developed to ensure medicine supply in rural areas.10 Although dispensing data are easily obtained from software systems and convenient to use, they fail to describe a dynamic intake behaviour.7
Polypharmacy, mostly defined as using five or more medicines, has been described to negatively affect adherence, among others.11–13 For chronic heart failure, polypharmacy including complex pharmacotherapies is common.14 Many patients struggle to follow strict medication intake schedules, in addition to daily weighing and dietary restrictions.14 Only for few medicines reliable biomarkers exist to predict medication adherence and assess the treatment success objectively. Further, biomarkers underlie physiological influences not linked to patients’ medication intake behaviours.15 In addition to physical examination and history taking, GPs can monitor heart failure by regularly assessing the biomarker NT-proBNP (N-terminal pro-B-type natriuretic peptide).16 This biomarker is used intensely in research and practice, but cut-off values are subject of controversy and differ between studies.17 Elevated values generally indicate uncontrolled disease management, which is noticeable through increased symptoms or the need for hospitalisation. NT-proBNP values are most representative within 2 weeks after changes in treatment.16
Globally, the opportunities in primary care linked to eHealth (eg, remote counselling) are expanding.8 Although Switzerland is among the late adopters of eHealth, electronic health records (EHRs) are considered as standard for recording patients’ medical history.18 19 In parallel, patients can self-monitor their disease management, including medication intake, with the use of mobile applications or wearable devices.8 However, these self-generated data are rarely included into GPs’ EHR.20 We expect that the availability of adherence data could guide GPs when adapting treatments and selecting targeted adherence interventions.
Aim
We aimed at developing an Adherence Monitoring Package (AMoPac) and evaluating its viability among GPs and heart failure patients. AMoPac consists of prospective electronic monitoring, calculation and report of patient’s adherence that is sent to the GP. In addition, we aimed to investigate GPs’ acceptance of AMoPac.
Materials and methods
Development of AMoPac
We developed the concept of AMoPac on the basis of peer-reviewed literature, primarily the work by Car et al on the role of eHealth within the patient’s journey through the healthcare system.8 In this article, the authors performed a literature review and proposed effective interventions to improve health outcomes and optimise medication adherence by using the opportunities that eHealth offers. We adopted the interplay of patient, pharmacy and physician, the simultaneous progression of the patient and the monitoring during his journey, and the personalisation of counselling.
Feasibility study
Study design
GPs were recruited in the network of one investigator (AZ). During routine appointments, GPs recruited heart failure patients. Patients assessed medication adherence with a small electronic device named Time4Med (Adherence Innovations, Hong Kong, China).9 Every time they take medicines, patients push a button that generates a time stamp. The monitoring duration was set at 4 weeks. The pharmacist conducted a home visit and gave patients feedback on their intake profile. An adherence report was generated by the pharmacist and sent to the GP. Patients’ NT-proBNP values were ordered by the GP once during the study duration (routine procedure for heart failure patients). The remuneration was 50 CHF for patients and GPs.
Patient inclusion criteria
Eligible patients were ≥18 years old, diagnosed with chronic heart failure (New York Heart Association (NYHA) class II–III), were prescribed at least two medicines to treat heart failure, self-administered their medication and were suspected of inappropriate intake behaviour by their GP (any reason was allowed).
Study outcomes
Our primary outcome was the feasibility of AMoPac, including collaboration between GPs and pharmacists, generating adherence reports and transmitting them into GPs’ EHR. Secondary outcomes were patients’ medication adherence and NT-proBNP. Adherence data were downloaded on a secured tablet and transferred as coded .csv files. Adherence metrics were given as:



drug holidays (days) = consecutive days (≥3) without medication intake.
The length of the grace interval was tailored to the medicine of interest. The pharmacist summarised the metrics for each patient in an adherence report and evaluated whether the intake behaviour was adequate or inadequate based on clinical-pharmaceutical considerations. NT-proBNP was assessed from blood samples and was analysed either at the GP’s surgery or at an external laboratory by applying their established method (not documented). Values >1000 pg/mL were considered elevated. We performed Spearman’s rank correlation test to investigate any correlation between NT-proBNP and medication adherence, a p<0.05 was considered statistically significant.
Transmission of the adherence report
We selected the software solution mednet (App V.2.4.389, ©2016–2021 novcom AG) owned by the Swiss company openmedical AG because it offers a secured gateway between the GPs’ surgery and the study pharmacy for the transmission of the adherence report.21 According to the Swiss data protection law, data are stored on local servers and secured through encrypted format.
Acceptance of the adherence report
We developed an interview guide (online supplemental appendix A) with 13 questions to investigate the GPs’ acceptance of the adherence report including a Numeric Rating Scale to rank the practical relevance of the report from 1 to 10 (1=unnecessary, 10=indispensable). We invited all GPs who had participated in the feasibility study (N=6). To widen the scope, we additionally invited 16 GPs who had participated in the BIOTICA study. In brief, GPs recruited patients in need of an acute antibiotic treatment and received our novel adherence report after patients had monitored their intake.22
Supplemental material
Study setting
One investigator (FD) interviewed the GPs face to face in their surgery or virtually (video call using ZOOM application). Interviewees gave verbal consent to record the interviews and use the data anonymously for further purposes. The remuneration was 50 CHF. Interviews were recorded (ZOOM application, Call Recorder Oygo or Recorder application). Two researchers transcribed (FD and AZ) and coded (FD and SB) the interviews independently. Differences were resolved through discussion; if no consensus was found, a third researcher (IA) was involved in the decision. All researchers had training in qualitative study methods. The reported results adhere to the COnsolidated criteria for REporting Qualitative research guidelines (online supplemental appendix B).
Supplemental material
Data analysis
Findings are presented as absolute numbers with percentages, means with SD and verbatim quotes. Representative quotes are presented in English after forward translation by one researcher (FD) from the original Swiss German language. Adherence reports were created by using Microsoft Word 2016 and Microsoft Excel 2016. Thematic analysis of the interviews with an inductive approach was used. Padlet 2022, a digital collaborative pinboard, served for coding the interview transcripts.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
The Adherence Monitoring Package
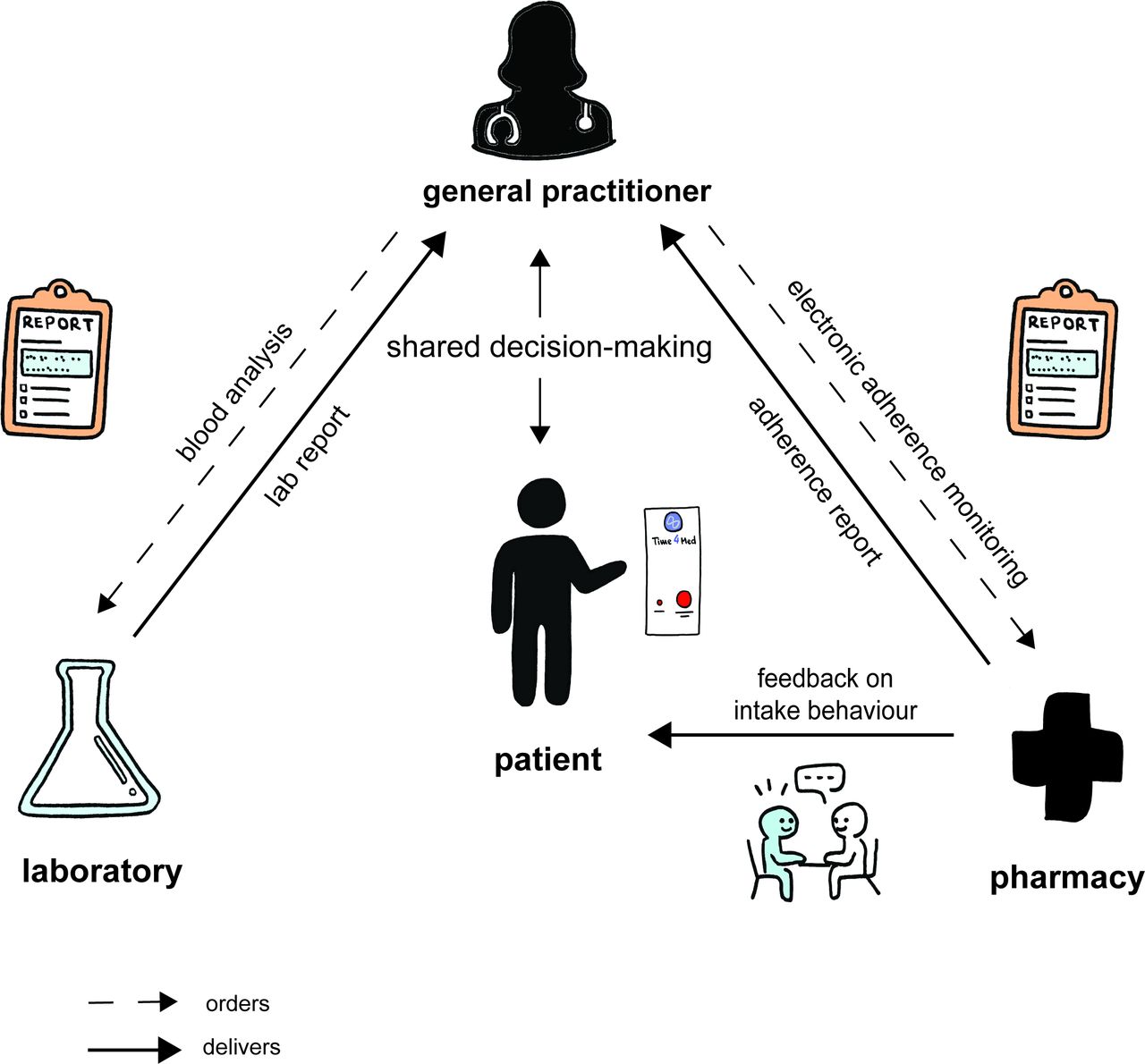
AMoPac interlaces the healthcare providers (GP, pharmacist), the supplier of proxy values (laboratory with biomarker results, pharmacy with adherence report) and the patient who is in the centre (figure 1) with focus on medication adherence. The process starts with the GPs’ suspicion of non-optimal intake behaviour whatever the reason, such as unmet therapy goals or uncontrolled clinical outcomes. After patients give their consent, the GP orders the monitoring of patients’ adherence at the pharmacy, in analogy to routine blood analyses such as NT-proBNP values from the laboratory. The pharmacist provides and instructs the monitoring device to the patient. After a preset monitoring time, optimally 3–4 weeks, the pharmacist downloads the monitoring data from the electronic device, generates a dot chart that displays every intake moment and comments on the medication intake profile. Direct feedback on adherence performance increases patients’ awareness of and motivation for the therapy, which leads to improved adherence and prevents deterioration of adherence over time.23 This can take place during a home visit or at the pharmacy in a private area. Patients are asked to clarify erratic or irregular intakes and to comment on delays or gaps. Then, the pharmacist analyses the monitoring data, enriches them with the patients’ comments and formulates an adherence report including pharmaceutical-clinical recommendations. The report illustrates the intake behaviour in a dot chart, delivers a clinical interpretation of patients’ adherence levels and recommends therapy optimisation if necessary.24
{kind=link}
The AMoPac concept is represented as a patient’s journey through the primary healthcare system that includes GP, pharmacy and laboratory. Central place is given to the electronic monitoring of patient’s adherence with the Time4Med device. AMoPac, Adherence Monitoring Package; GP, general practitioner.
With the knowledge of the adherence monitoring and the laboratory testing, an informed decision about potential therapy adjustments is possible. Appropriate adjustments can include tackling polypharmacy by means of for example single-pill combinations or deprescribing of unnecessary or inappropriate medicines (to reduce the daily pill burden and to increase adherence to essential medicines).11 25 Synchronising intake times with the patients’ daily routine is a further possible adjustment option. In addition, interventions to improve adherence should be selected in a shared decision-making process with the patient. Tailored interventions that focus on adjusting patients’ behaviour were more likely to succeed in trials.26 27 AMoPac can be used repeatedly for example, to evaluate the success of adherence interventions and treatment adaptions.
Feasibility study
Six GPs in the area of Basel, Switzerland, were recruited. Mean working experience was 22.5±8.5 years, and 80% were men. Five GP surgeries were not able or willing to instal the mednet software to receive adherence reports directly into the EHRs. Incompatibilities with their primary IT system or pending updates were the reasons evoked. One surgery installed the software and did not receive the transmitted adherence report. As a substitute, all adherence reports were sent as password-secured PDF files via email; reports were then manually transferred and saved in the EHRs. Therefore, the integrated transmission of reports was not feasible.
From August 2020 to September 2021, nine patients with heart failure were recruited by their GP. All patients gave written informed consent at study inclusion; study participation was voluntary. Two patients withdrew their consent and one patient died before finishing the study due to an acute heart failure decompensation. Six patients finished the study. Patients were on average 82.1±11.1 years old (table 1).
Characteristics of heart failure patients (N=7) with adherence monitoring values during 4 weeks of observation
Mean taking and timing adherence was 86.4%±12.8% and 85.9%±13.8%, respectively. No drug holidays (≥3 days without intakes) were observed. The individual intake pattern of three patients revealed inadequate intakes that is frequently omitted doses in the evening. In the adherence reports of these three patients, the pharmacist recommended additional support such as reminders to optimise treatment fidelity. Four patients had elevated NT-proBNP levels (>1000 pg/mL). The patient with the highest adherence (100%) showed the lowest NT-proBNP value (102 pg/mL) and vice versa (67%; 8561 pg/mL). However, the correlation test showed no statistical significance over the 6 patients (rs = –0.67, p=0.14). All patients appreciated the individual feedback on their medication-taking behaviour during the home visit from the pharmacist; no patient expressed difficulties with the study setting.
Acceptance of the adherence report
From April to October 2021, 22 GPs were invited and 11 (50%) participated in the interviews (7 from the BIOTICA study). Mean working experience was 27.3±7.1 years, and 64% were women. Interviews lasted on average 12.3±5.8 min. We identified four main themes: (1) merit of medication adherence, (2) determinants for the need to monitor adherence, (3) comments on adherence report and (4) factors facilitating the implementation of AMoPac, with subthemes and codes (online supplemental appendix C: Coding tree). GPs consistently expressed satisfaction with the adherence report and agreed with the recommendations. Minimal requests for improvement were made based on individual preferences such as omitting adherence calculation formulas or adding information on side effects. GPs with a self-dispensing licence (N=4) expressed concerns about the cooperation with pharmacies.
Supplemental material
The theme ‘merit of medication adherence’ includes that knowledge of medication adherence is valuable in GPs’ daily practice. Four GPs have implemented methods to assess adherence, such as analysing dispensing data from the pharmacy or their own surgery. When discussing adherence-related issues with patients, GPs mainly address if and how patients take medication and the occurrence of side effects.
I say: 'Do you still have some of these [tablets]?' 'Yes, yes, quite a lot.' […] 'But, if you take one [tablet] a day and picked [a package] in January, there should not be any left now, should there?' (GP-4)
The ‘determinants for the need to monitor adherence’ were outcome, therapy and patient related (high age and living situation). Five GPs suggested monitoring adherence when patients miss their clinical outcome goal, such as controlling high blood pressure. Monitoring adherence to chronic treatments was mentioned more often (N=8) than acute ones (N=3). GPs argued that patients would need a higher motivation to engage in treatment for a long time, especially when the disease is asymptomatic.
Yes, there are people where you have the feeling or where you ask yourself how adherent they are […] with the blood pressure medication, those who are not well adjusted even with higher [dosages] or multiple combinations, in that case, it would be beneficial. (GP-9)
The ‘comments on adherence report’ concerned the layout and content of the report. Both were generally complimented as clearly arranged and easy to understand. GPs rated the practical relevance of the transmitted information on average as 6.9±2.3. The GPs described the dot chart and the findings as essential parts of the report. Two GPs expressed general difficulties to look into the report in detail. Five GPs suggested minor improvements, such as adding information on side effects.
All easy to understand, excellent that it fits on one page, visually well arranged. (GP-10)
So for people who are less experienced, it may be that it is a bit overloaded. But I cannot exactly say what I find too much. (GP-1)
The ‘factors facilitating the implementation of AMoPac’ summarises necessary situations to implement the tool in practice. The process should be standardised with clearly distributed tasks. Ten GPs favoured receiving reports electronically via email or integrated into their EHR system. Six GPs recognised the cooperation with community pharmacies as valuable or even ideal in the case of polypharmacy. Three GPs with a self-dispensing licence had concerns about a third person interfering in their treatment recommendations and political issues.
Discussion
AMoPac was developed to assess non-adherence in patients with polypharmacy and to deliver a pharmaceutical analysis to primary care providers. In the literature, sophisticated approaches to identify non-adherence in everyday practice are rare. Some theoretical considerations include questionnaires to identify barriers before therapy22 but implementing such services in practice is pending. Our approach is linked to unmet treatment goals or non-response to treatment. If no clinical reason can be found to explain the situation, maximising dosage or adding a new medicine to the treatment is mostly performed. With AMoPac, GPs in search of an explanation for unmet treatment can insert an adherence monitoring period before therapy adjustment, and elucidate non-response and non-adherence.
We tested the feasibility of AMoPac and included the transmission of the adherence report directly into the EHR of GPs. The integrated transmission failed due to incompatibilities between the primary EHR provider and the mednet software. GPs were generally reserved when asked to instal new software or run the current updates because they regularly experienced technical issues in the following days. This belongs to barriers to implementing eHealth systems and is described in the literature. Car et al suggest adequate planning, piloting and digital literacy for successful execution.8 In Switzerland, the national strategy to implement an electronic patient dossier (EPD) had major throwbacks that are associated with technical incompatibilities.19 The overwhelming amount of over 50 software solutions for primary care providers, where each system requires its own gateway, complicates the situation in an unprecedented way.
The taking adherence in our sample of heart failure patients was 86.4%. This value is higher compared with the rate of 56%–77% adherence that was measured electronically in the same population in other studies.28 29 Riegel et al reported similar rates (84.7%) in discharged heart failure patients, although with decreasing tendency over time.30 However, the high taking adherence level could be a contradiction to the suspicion of non-adherence. In fact, it demonstrates that averaging medication intakes with a single number is not sufficient to identify individuals who struggled with medication intake. Thus, the most challenging part might be to recruit the suspected non-adherent patients because they might be reluctant to be monitored or do not want to admit deviant behaviour.
Little is known about the non-adherence level in heart failure patients that might be critical. An adherence threshold has been determined only for a handful of clinical outcomes.31 Wu et al defined a relevant cut-off point for adherence to heart failure treatment.29 Patients with adherence levels above 88% had fewer clinical events and better health outcomes. However, adherence is a timely dynamic behaviour and cannot be easily summarised in a single number. On the one hand, 90% adherence can be translated into missing one dose every 10 days, which is without consequences for most treatments. On the other hand, 90% adherence also means missing a whole week of intakes during a 10-week monitoring period, which might be more troublesome. Therefore, instead of dichotomising patients into adherent and non-adherent depending only on a threshold, we present raw data as a dot chart and four different adherence metrics. In addition, we consulted pharmacological parameters of the drug and applied clinical judgement when evaluating intake behaviours. Thus, the final appraisal for a patients’ adherence to be adequate or inadequate is the result of a complex evaluation.
The span of NT-proBNP values and adherence levels in our study was extensive. Although our sample was small with six patients, we assume a potential relationship between adherence and NT-proBNP level: the patient with the most elevated NT-proBNP value and uncontrolled heart failure had the lowest adherence value and vice versa. NT-proBNP is a valuable biomarker for GPs to target heart failure treatment.16 Hardly anything is published about how deviant intake behaviour affects this biomarker. Dovancescu et al found nearly doubled NT-proBNP values in patients who omitted heart failure medication for 48 hours on purpose.32 This increase was present even before weight gain was measurable. Therefore, critical NT-proBNP levels could be valuable for tailoring adherence assessments and identifying patients who deviate from prescribed pharmacotherapy.
In our feasibility study, all pharmacist-linked activities were performed by the investigator (FD) who is a pharmacist by training with expertise in clinical pharmacy. Involving more community pharmacies will be essential to implement AMoPac in the healthcare setting. Pharmacies have low-threshold access to their patients, ensure continuity of care and can intervene to enhance medication adherence.33 An interprofessional, team-based care approach has been shown to improve the quality of care.34 However, community pharmacists will need to undergo specific training prior to perform data analysis. Such training is currently not available in Switzerland. As a temporary solution, the adherence analysis and interpretation could be outsourced to a specialised institution (eg, university research groups or clinical pharmacists) who delivers consistent quality. The community pharmacy would receive the adherence analysis and could then deliver the adherence feedback and counselling session with the patient. Besides GPs and pharmacists, additional healthcare providers such as nurses can be included in the AMoPac concept to ensure optimal outcomes. GPs’ comments on interprofessional cooperation diverged widely in the interviews. GPs with a licence to self-dispense medication were eager to make their own decisions rather than having someone interfering from the pharmacy. From this expected reaction, we conclude that interprofessional cooperation needs to be reinforced, especially in rural areas. Nevertheless, self-dispensing GPs also agreed with the usefulness of recommendations from the adherence report.
Strengths and limitations
Our study has several strengths. First, stakeholders’ participation was taken into consideration. We included GPs at every stage of the development of AMoPac and retrieved their opinion. Patients were also invited to make comments on the study design. Patients were satisfied with the study procedure and appreciated the tailored feedback on their intake behaviour. Second, we used electronic monitoring to assess medication adherence, which is the best evaluated method to measure the success of treatment implementation. Third, the number of participating GPs (N=11) in the interviews was adequate to deliver trustful results. Guest et al found that 11–14 participants are sufficient for qualitative research to reach thematic saturation in rather homogeneous groups.35 Fourth, we recruited a sample of six general surgeries. This was sufficient for a feasibility study to identify the technical problems and test our study design.36
We acknowledge some limitations. First, the participants (GPs and patients) in our study were from the German-speaking part of Switzerland only. Therefore, no general conclusion to other languages or cultures is possible. However, we could catch opinions from GPs in different working situations, including self-dispensing GPs. Second, we cannot exclude selection bias of patients. It is known that more motivated and health aware people are more likely to participate in studies. Nevertheless, three patients deviated from ideal intake behaviour. Although they were aware of the monitoring, they struggled with medication management and intake. Third, electronic monitoring has its known limitations. Pushing a button simultaneously with medication intake requests an additional action from the patient, which can add complexity to the therapy compared with just removing a tablet from the packaging and taking it. Thus, it is possible that our study measures were underestimating intake. However, corresponding NT-proBNP values may contradict this affirmation. Fourth, we experienced technical issues with the transmission of adherence reports into the GPs’ EHR. To overcome this issue, we sent the reports via encrypted email. This represents a standard technical solution most GPs in Switzerland use to transfer patient-related documents. The use of already established methods was the only feasible way to overcome this barrier to feasibility of the intervention. Finally, the community pharmacies were represented by one study pharmacist. In case of deployment of the intervention in practice, interested pharmacists would need training. Even if knowledge and resources are currently available in community pharmacies for new services, training could represent a barrier to feasibility of the intervention. Especially, time shortage might represent the biggest issue. Recruiting several pharmacists and train them was not possible within the resources for this study.
Outlook
Our feasibility study aimed to prepare a larger study investigating the usefulness of AMoPac. Further, the impact of AMoPac on clinical outcomes will be investigated.
Conclusion
We developed AMoPac as a comprehensive tool including a pharmaceutical-clinical report, tested it for feasibility in a real-world scenario, and showed that the package is accepted and appreciated by all stakeholders. GPs described the process altogether as effortless and complimented the clarity and relevance of the adherence report. Although a generalisation is not possible, it is striking that few EHR providers and GP surgeries seem prepared for the smooth integration of external documents in Switzerland.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Northwestern Switzerland EKNZ ID: 2019-01248. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank all GPs and patients for their valuable input and participation in our studies. We also want to thank Andreas Haenny and Selina Barbati, who were of great help in transcribing and coding interviews.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to this study. FD: guarantor, IA, AZ and FD: study design and execution, FD: carried out interviews and data analysis, IA and SA: conceptualisation and supervision, FD: preparation of the manuscript, AZ, IA, SA and FD: read, reviewed and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.