Article Text

Abstract
Blood culture contamination (BCC) is a significant quality and safety issue in hospitals, as it leads to increase in unnecessary testing, admissions, antibiotic exposure and cost. This study is the first study on the BCC rates in Armed Forces Hospital Jizan (AFHJ), Saudi Arabia. The main goal of our quality improvement (QI) project was to reduce BCC rate in AFHJ from 7.5% to international benchmark (<3%) after January 2021 as well as to reduce the negativity rate. This study was conducted in AFHJ (KSA) including two major steps: first, development and implementation of QI interventions to reduce BCC and negativity rate in the AFHJ. Second, evaluation of the effectiveness of these interventions. The intervention was developed through QI methodologies, including fishbone diagramming and the plan–do–study–act cycle. Intervention effectiveness was evaluated using an interrupted time series analysis. Clear survey questionnaires were made and distributed to participants to get preaudit results.Then we started the education programme depending on the preaudit results. Soft copy of written steps of blood collection procedure and indication was done and sent to nurses and physicians. After that, direct observations of nurses involved in the process were conducted. Finally, post-training assessment using previous survey questionnaires was performed to get postaudit results. During the baseline period (preintervention period), 7.5% from blood culture were contaminated, compared with 1.8% during the intervention period (postintervention period). Rate of negative blood culture was reduced from 96% to 91%. Overall improvement of knowledge and awareness of the nurses and physicians clearly noted after intervention implementation. Fortunately, we have noted that the budget of microbiology would be reduced by 10%–12% as a result of our interventions. By standardising blood culture collection methods, optimising blood volume and nurses’ education, we were able to develop a best practice for blood culture collection and to reduce BCC and negativity rate to a sustainable low rate at our hospital.
- Education
- Antibiotic management
- Audit and feedback
- Communication
- Compliance
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Most hospitals are suffering from blood culture contamination (BCC) issue, which affects the patient treatment plan.
WHAT THIS STUDY ADDS
The most effective tools for succeeding such project were education and effective communication between the microbiology department and other departments.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The BCC cannot be eliminated but can be reduced to the international benchmark (<3%). Monitoring and evaluation system should be a continuous process for the sustainability of such project.
Problem
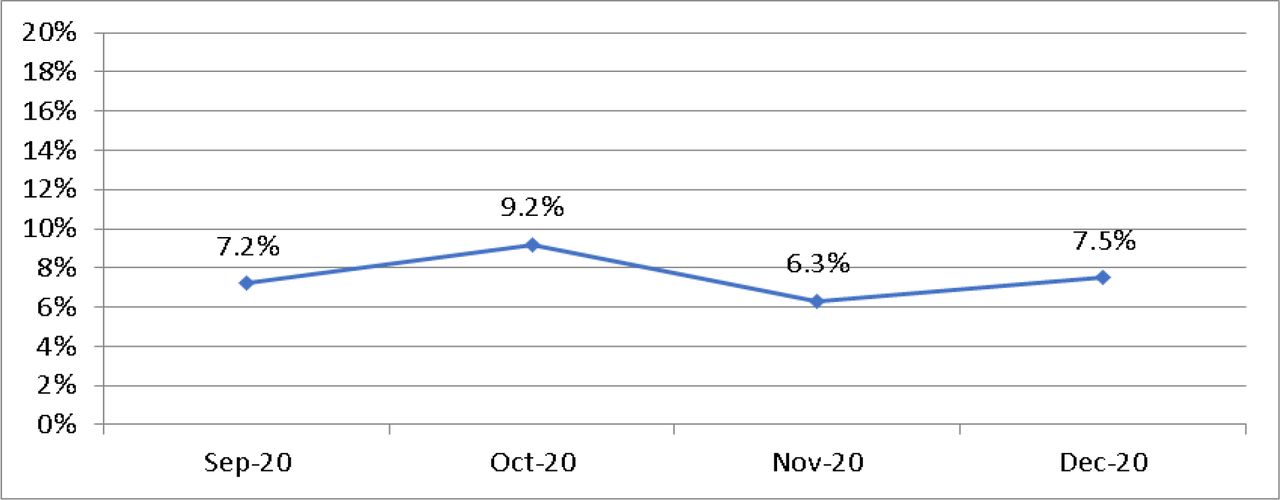
Blood culture contamination (BCC) is a significant quality and safety issue in hospitals as it leads to increase in unnecessary testing, admissions, antibiotic exposure and cost. During the baseline period from September 2020 to December 2020, BCC is sharply increased, reaching an average of 7.5% (figure 1), causing dissatisfaction from treating physicians, microbiology technologists as well as patients. The rate of the negative blood culture is 96%, and this high rate indicates unnecessary ordering of such test by treating physicians.

Blood culture contamination rate before intervention (mean=7.5%).
Background
The blood culture is a critical tool for detecting the dangerous presence of living organisms in the bloodstream. A positive blood culture can suggest a definitive diagnosis, enable the targeting of therapy against the specific organisms in question and provide prognostic value. Like any test, however, false-positive results can limit the utility of this important tool. In blood cultures, false positives arise due to contamination, which occurs when organisms that are not actually present in a blood sample are grown in culture.1
BCC is defined as the recovery of normal skin flora from blood culture which entered during sampling but actually not circulating in the patient blood. BCC is a significant quality and safety issue in hospitals as it leads to increase in unnecessary testing, admissions, antibiotic exposure and cost. BCC issue is further complicated in recent years due to the increasing use of central venous catheters and other indwelling vascular access devices. Interpretation of culture results for patients with these devices in place is particularly challenging because while these individuals are at increased risk of bacteraemia, such results may also indicate culture contamination or colonisation of the line.2–4
The financial impact of BCC has been described in several studies. Measured in costs or charges, there is compelling evidence that the financial impact of BCC is significant. Bates et al found that contaminant results, compared with true-negative results, were independently associated with increased subsequent laboratory charges (20% increase) and intravenous antibiotic charges (39% increase).5–7
In a subsequent prospective study focused on BCC caused by coagulase-negative staphylococci, Souvenir et al reported that almost half of the patients with a false-positive result were treated with antibiotics, often with vancomycin. Thuler et al found that 26% of children with false-positive cultures who were initially evaluated as outpatients were subsequently admitted to the hospital based on initial culture results.2 8 Therefore, the aim of our quality improvement (QI) project was to reduce BCC rate in Armed Forces Hospital Jizan (AFHJ) from 7.5% to <3.0% after January 2021.
Objectives
To reduce the BCC rate in AFHJ from 7.5% to international benchmark (<3%) and to reduce the negativity rate.
To standardise the procedure of blood collection for culture.
To improve knowledge and awareness among all healthcare workers involved in this process.
To maintain and save laboratory and hospital resources because false blood culture results lead to wasting of valuable laboratory resources and the unnecessary use of antibiotics.
Design
Clear survey questionnaires were made and distributed TO participants to get preaudit results to assess the knowledge and awareness of nurses in the wards, intensive care units (ICUs) and emergency rooms (ERs) about the blood culture procedure before starting any training or education to get preaudit results to simply detect the area of defect that need more training and education.
Education and training programmes depending on the preaudit results (power point lectures, direct personal training for the nurses in each department and verbal discussion with them about the difficulty in implementing the ideal blood culture collection procedure) that lead to better understanding and implementation of the proper procedure of blood culture collection.
Soft copy of written steps of blood collection procedure and indication was made and sent to nurses and physicians to increase their knowledge and awareness about such procedure, which lead to BCC and negativity rate reduction.
Direct observations of nurses involved in the process to increase the sense of importance of this procedure and responsibility of each participant.
Post-training assessment using previous survey questionnaires to get postaudit results to alert us about some defects in some areas of this procedure, which lead us to re-educate and observe again those nurses who had such defects to reduce the possibility of collecting contaminated blood culture to the minimum.
Continuous monitoring of BCC and negativity rate to ensure the reduction in the contamination and negativity rates.
Blood culture results have been monitored to observe if the previous interventions have succeeded to reduce contamination rate along with measuring the financial impact on it. A prospective collection of the BCC rate per month will give us insight in the effectiveness of the proposed interventions. To estimate the financial impact of BCC, we calculate the cost of all the items used in the blood culture collection and processing as well.
Baseline measurement
We collected the number of blood culture per month then contamination and negativity rates calculated in addition to the calculation of cost of the tests. We used line chart to monitor the BCC rate per month. Negative rates of blood culture have been calculated as well. Retrospective collection of data was from electronic system and microbiology logbook. In addition, awareness of nurses percentage regarding blood culture procedure was calculated.
Continuous quality measures
Continuous quality measures include permanent weekly meeting with the head nurse to assess and facilitate the flow of proper blood collection procedure; onsite training and corrective action, if necessary; and continuous monitoring of blood culture results to do re-education in case of any BCC detected.
Strategy
AFHJ is a 70-bed capacity hospital with an average blood culture sample of 1315 per year. The microbiology department provides service 24 hours, 7 days, for all patients using this facility. This study included two major steps: first, development and implementation of QI intervention to reduce BCC and negativity rate in the AFHJ; second, evaluation of the effectiveness of this intervention. The intervention was developed through QI methodologies, including fishbone diagramming (root cause analysis (RCA)) and plan–do–study–act (PDSA) cycles.
Three cycles were conducted of PDSA cycles in order to improve the BCC rate. These have been grouped into the following themes: standards of practice (PDSA1), engagement and education (PDSA2), and feedback and learning (PDSA3).
PDSA1
The initial meeting was held with the head of microbiology, the head nurse, and the head of ICU and ER to discuss the reasons behind the BCC and acceptable methods to resolve this issue. The recommendations from this discussion were to start with a questionnaire survey to assess the knowledge and awareness of nurses in the wards, ICU and ER about the blood culture procedure to get the preaudit results to simply detect the area of defect that needs more training and education. Education and training programmes were developed based on the preaudit results, which provide better understanding and implementation of the proper procedure of blood culture collection.
PDSA2
A soft copy of written steps of the blood collection procedure and indication was made and sent to the nurses and physicians. Direct observations of the nurses involved in the process were conducted. Post-training assessment was conducted to get postaudit results, which lead us to re-educate and observe again those nurses who still had defects in some areas in the procedure.
PDSA3
This includes continuous monitoring of BCC and negativity rate to ensure the reduction in the contamination and negativity rate and sharing of this information with the head nurse and the heads of the ICU and ER. A retrospective collection of the BCC rate per month will give us clear insight on the effectiveness of the proposed interventions.
Intervention effectiveness was evaluated using an interrupted time series analysis comparing contamination and negativity rates prior to and after implementation of the intervention. RCA (figure 2) was used by the project team to determine the main causes for increased BCC (>3%) as well as brainstorming session to propose the corrective actions and interventions.
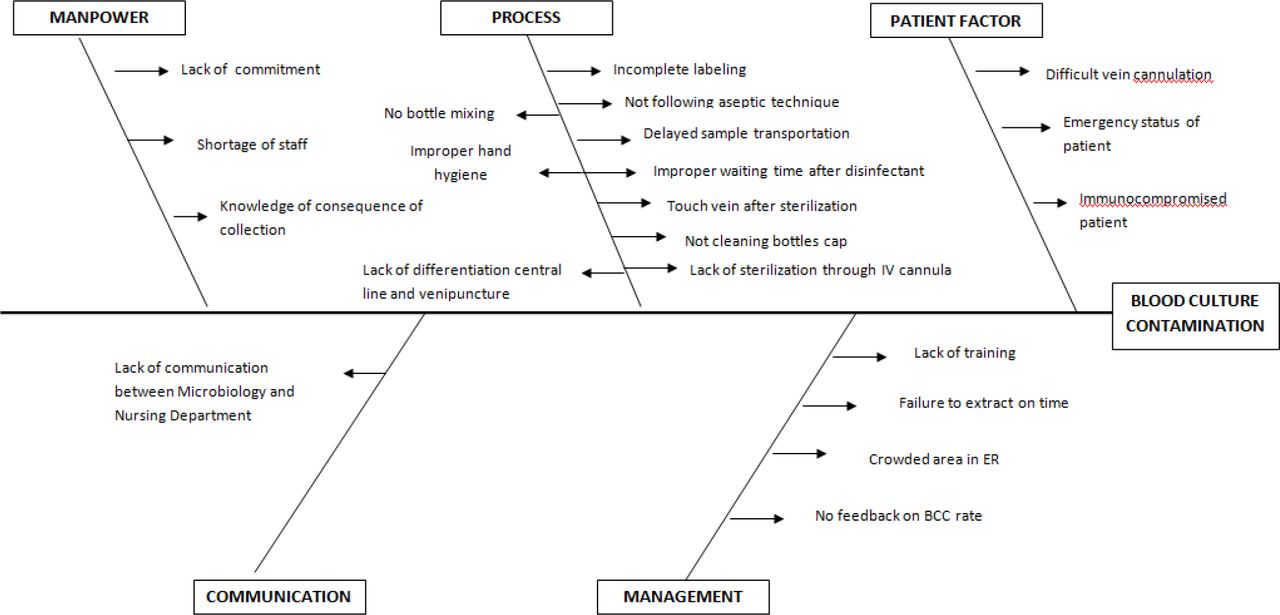
Root cause analysis for increased BCC. BCC, blood culture contamination; ER, emergency room.
Set up survey questionnaire
The team has made a survey composed of 13 clear questions to assess the knowledge and awareness of nurses in the inpatient wards, ICU and ER about the blood culture procedure before and after interventions (box 1). These questions cover almost all the areas regarding blood culture collection procedure and participants’ answer will be corrected simply as correct or wrong answer. Codes for these questions were formulated as shown in table 1. These codes would be used during data analysis as each code indicates one specific question.
Survey questionnaire form used in this project.
Blood Culture Collection Survey
Department……………………Job Title…………………
Instructions:
Read all the questions carefully then answer them based on your current knowledge and experience.
Cell phone and computer are not allowed.
Allowed time for completion the survey is 30 minutes.
Q.1/ Arrange the steps of blood culture collection procedure in the correct order:
Identify the patients by asking them to state their name and age then compare their response to the written request.
Choose the appropriate vein by touching skin.
Clean draw site in circle motion about 5 cm using 70% isopropyl alcohol and allow air dry for 30 seconds.
Wash your hand (hand hygiene) first then wear new gloves.
Insert needle and draw enough blood volume.
Clean draw site in circle motion about 5 cm using 2% tincture iodine or betadine and allow air dry for 1 minute.
Immediately transfer unclotted blood into blood culture bottle.
Clean draw site using 70% isopropyl alcohol after collection procedure.
Answer………………………………
Q.2/ Yes and NO question, please write Yes or No at the end of each sentence:
Is it necessary to wash your hand before wearing gloves?
Choosing the vein before antiseptic procedure.
Is it necessary to change needle after drawing blood and before injecting blood into bottle?
Is it necessary to disinfect top of bottle before injecting blood into bottle using alcohol?
Is it necessary to disinfect top of bottle before injecting blood into bottle using iodine?
Do you check bottle for clarity before injecting blood?
Blood sample for culture must be drawn before any lab test.
Q.3/ Briefly answer the following questions CLEARLY:
What you will do if you need to touch draw site again after antiseptic procedure?
What you will do if you find bottle turbid before injecting blood on it?
What is the best time for blood collection for culture?
If antibiotic treatment started before collection of blood, when do you must collect blood for culture?
State appropriate blood volume for adult and pediatric in each bottle?
Code formulation for survey questions
Set up blood culture collection procedure
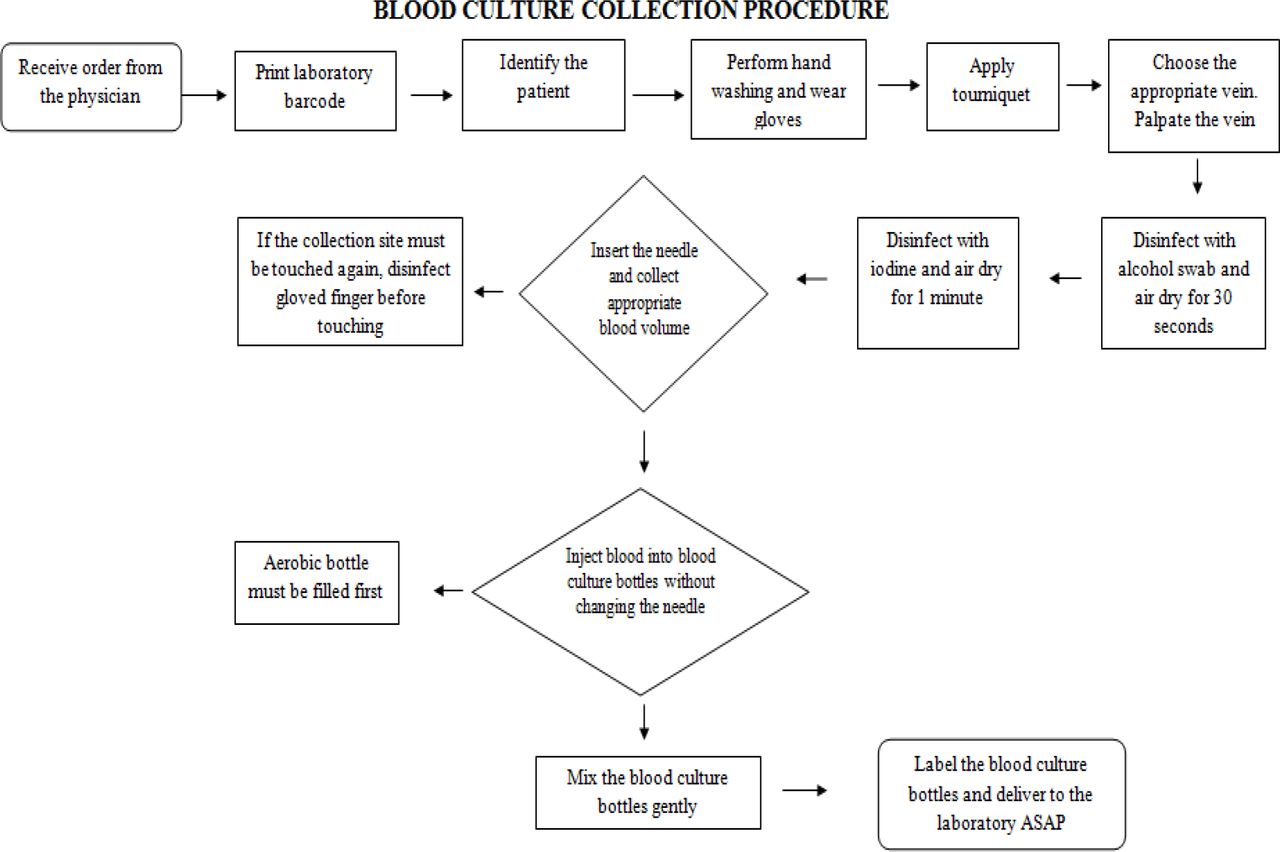
Blood culture collection procedure has been made and distributed in two forms. One form was clear instructions written in the best correct order of the procedure (box 2), and the second form was as a flowchart (poster) to make it easy for the nurses to understand and follow (figure 3).
Written instructions of blood culture collection procedure.
Instructions of Blood Culture Collection Procedure
Identify the patients by asking them to state their name and age then compare their response to the written request.
Blood sample for culture must be drawn before any lab test.
Blood for culture must be collected when patient febrile and before starting antibiotic but if the antibiotic has been started, collect the sample before the second dose.
Prepare phlebotomy items and blood culture bottle.
Remove plastic flip on top of the bottle and disinfect top of bottle using 70% isopropyl alcohol.
Check the bottle for clarity and any bottle showed turbidity must be discarded.
Wash your hands (hand hygiene) first then wear new gloves.
Choose the appropriate vein by touching skin before antiseptic procedure.
Clean draw site in circle motion about 5 cm using 70% isopropyl alcohol and allow air dry for 30 seconds.
Clean draw site in circle motion about 5 cm using 2% tincture iodine or betadine and allow air dry for 1 minute.
If the draw site must be touched again disinfect gloved fingers before touching.
Insert needle and draw enough blood volume then immediately transfer unclotted blood into blood culture bottle without changing needle to prevent blood from exposure to air and contamination. Shake gently after putting blood. Note (Aerobic bottle filled first and lable properly)
Blood volume depend on type of used bottle and age of patient so always follow manufacturer instructions but usually it is recommended 8-10 ml in each adult bottle and 1-3 ml in each pediatric bottle.
Usually 2 or 3 blood culture set must be cultured with intervals of 1 hour or less if the treatment cannot be delayed.
Finally clean the draw site from iodine using 70% isopropyl alcohol because many patients are sensitive to iodine and iodine leave stain on clothes.

Flowchart of the blood culture collection procedure. ASAP, as soon as possible.
Premeasurement results
Preaudit evaluation was started before interventions and corrective actions. Preaudit of proper blood culture collection was conducted by microbiology staff as well as the head nurse of each involved department to assess knowledge and awareness of nurses regarding blood culture collection procedure using a survey questionnaire composed of 13 questions, and each question has its own code as displayed in table 1. Negative rates of blood culture before intervention have been calculated and found to be 96%.
Response rate for education and survey questionnaire of each department
From figure 4, we noted that the response rate in all involved departments was higher than 50%, with the least response rate noted in ER.

Response rate for the education and survey questionnaire of each department. ER, emergency room; ICU, intensive care unit.
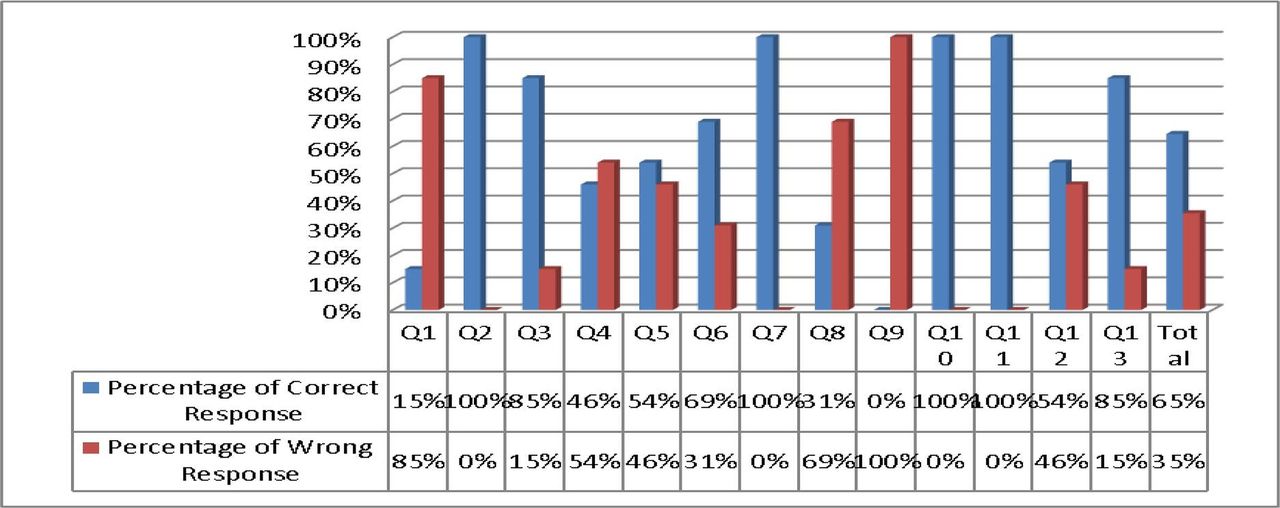
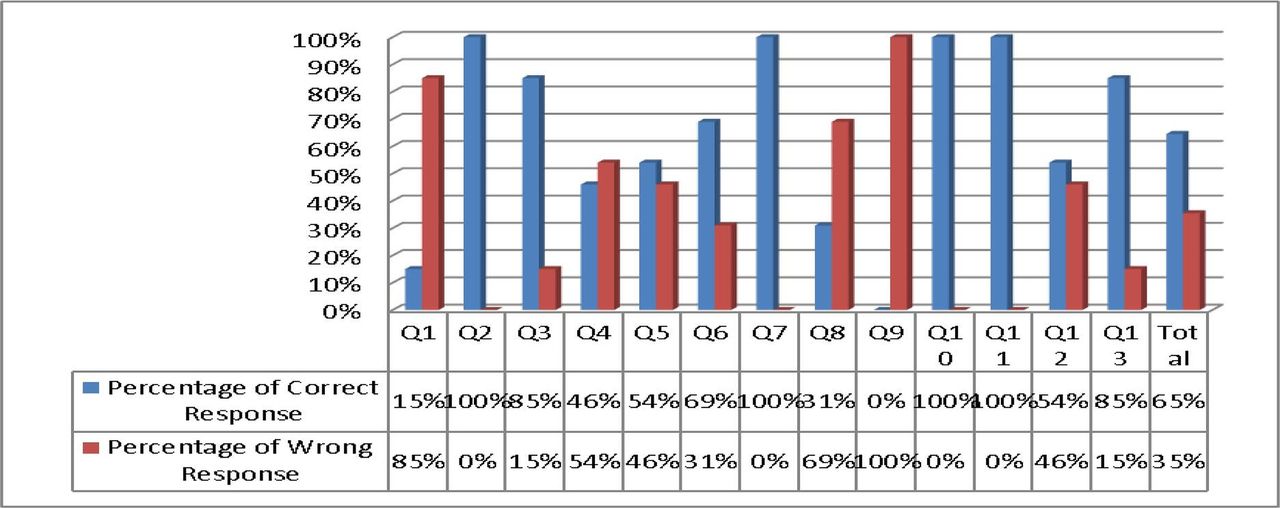
Response of blood culture collection survey before intervention in the emergency department
From figure 5, we noted that 60% of ER participants respond correctly but 40% respond wrong, and this result explains increasing BCC rate.

Response to the blood culture collection survey before intervention in the emergency department.
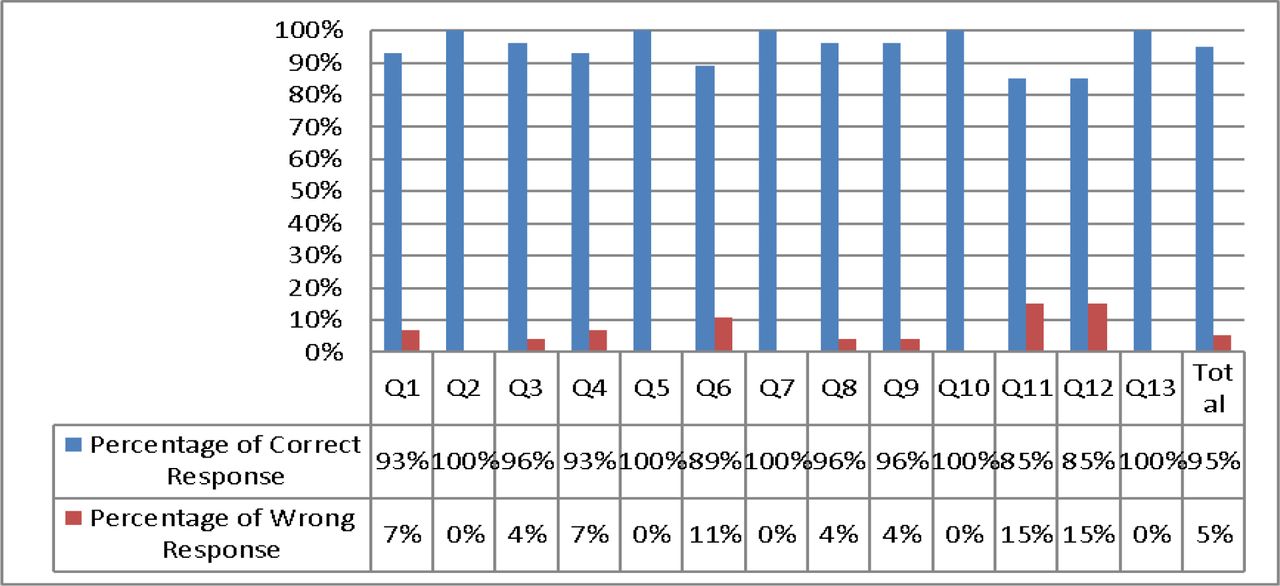
Response of blood culture collection survey before intervention in ICUs
From figure 6, we noted that 65% of ICU participants respond correctly, but 35% respond wrong, and this result also explains increasing BCC rate.
Response to the blood culture collection survey before intervention in intensive care units.
Response of blood culture collection survey before intervention in inpatient wards
From figure 7, we noted that 61% of participants from inpatient wards respond correctly, but 39% respond wrong, and this result also explains increasing BCC rate.

Response to the blood culture collection survey before intervention in the inpatient wards.
Postmeasurement result
Postaudit was started 3 weeks after starting of interventions and corrective actions. Postaudit of proper blood culture collection was conducted by microbiology staff as well as the head nurse of each involved department to check the improvement in this practice using the same criteria used for preaudit evaluation regarding such procedure.
The BCC rate retained back to the international benchmark (<3%) as well as improvement of the awareness of ordering this test which impacts the cost positively. During the baseline period from September 2020 to December 2020, 36 out of 481 who had blood culture tests (7.5%) were contaminated, compared with 15 out of 834 (1.8%) during the intervention period, which is started in the beginning of January 2021, saving microbiology budget an estimated average of 10%–12% in one year. Negative rates of blood culture after intervention have been reduced from 96% to 91%, and this result indicates that physician awareness about blood culture indications has been improved.
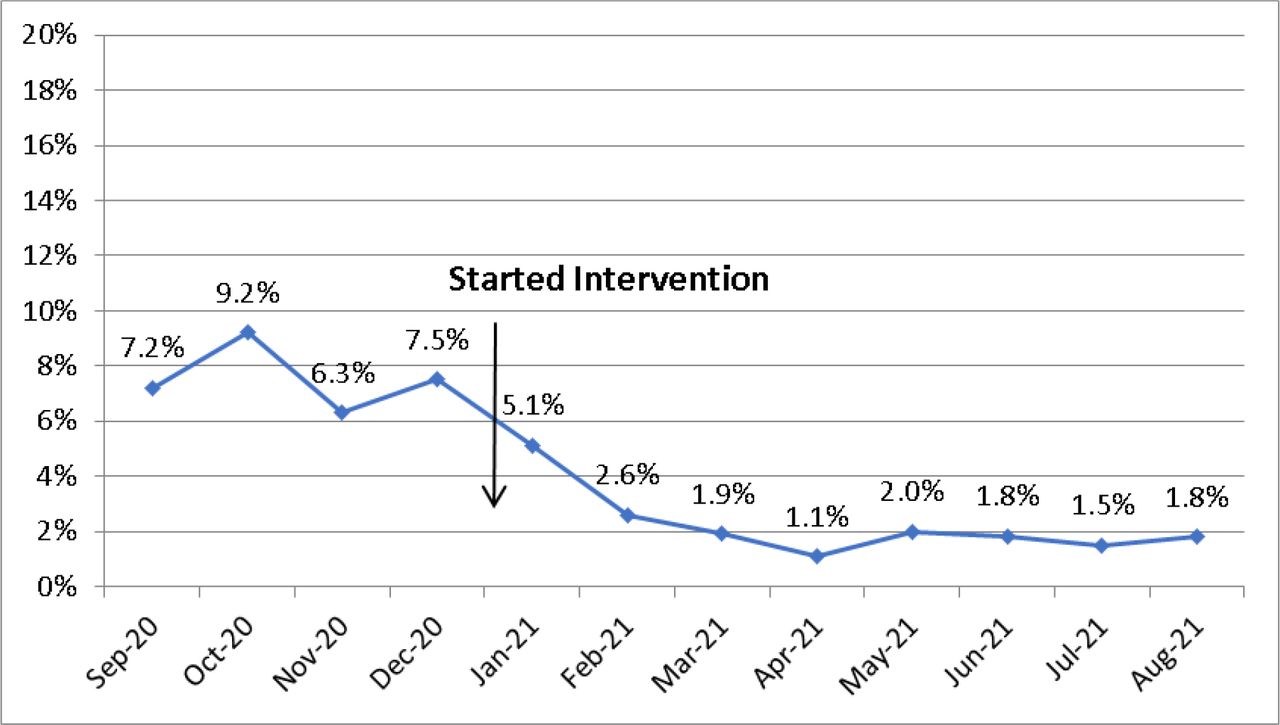
BCC rate per month after intervention
BCC rate during the intervention period reduced to the international benchmark (<3%) as shown in figure 8.

Blood culture contamination rate per month after intervention (,ean=1.8%).
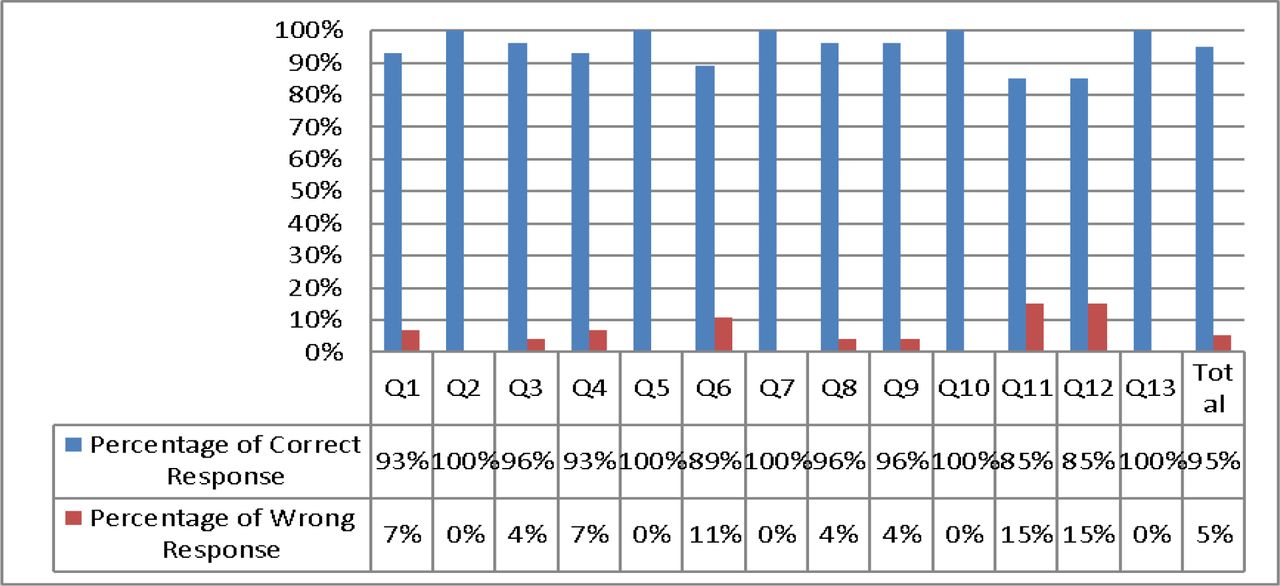
Response of blood culture collection survey after intervention in the emergency department
From figure 9, it is clearly noted that most of the ER participants respond correctly (95%) and only a few of the participants (5%) respond wrong, and this result explains great reduction of the BCC rate.
Response to the blood culture collection survey after intervention in the emergency department.
Response of blood culture collection survey after intervention in the ICU
From figure 10, it is clearly noted that most of the ICU participants respond correctly (97%) and only a few of the participants (3%) respond wrongly, and this result explains great reduction of the BCC rate and the success of the education and training programme.
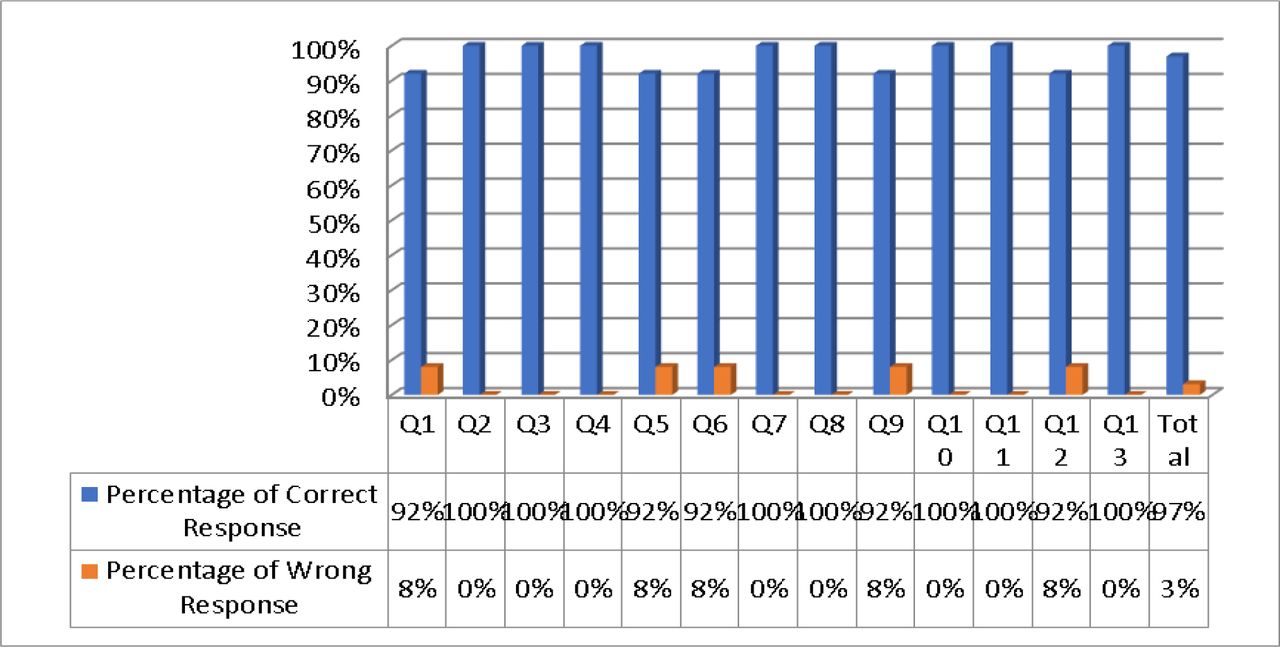
Response to the blood culture collection survey after intervention in the intensive care unit.
Response of blood culture collection survey after intervention in inpatients wards
From figure 11, it is clearly noted that most of the wards participants respond correctly (96%) and only a few of the participants (4%) respond wrongly, and this result explains great reduction of the BCC rate and success of the education and training programme.
Response to the blood culture collection survey after intervention in inpatient wards.
Comparison of premeasurement and postmeasurement results
Here, we summarise all the results of preaudit and postaudit results to make it easier for the reader to notice the difference between them as well as viewing the successful of the implemented interventions.
Comparison of BCC rate per month before and after intervention
From figure 12, we noted that since the interventions have been started, the BCC rate reduced to our target the international benchmark (<3%) (p value of 0.001). The confidence interval (CI) before intervention was (CI 6.012 to 8.048) and after intervention (CI 1.519 o 2.241).
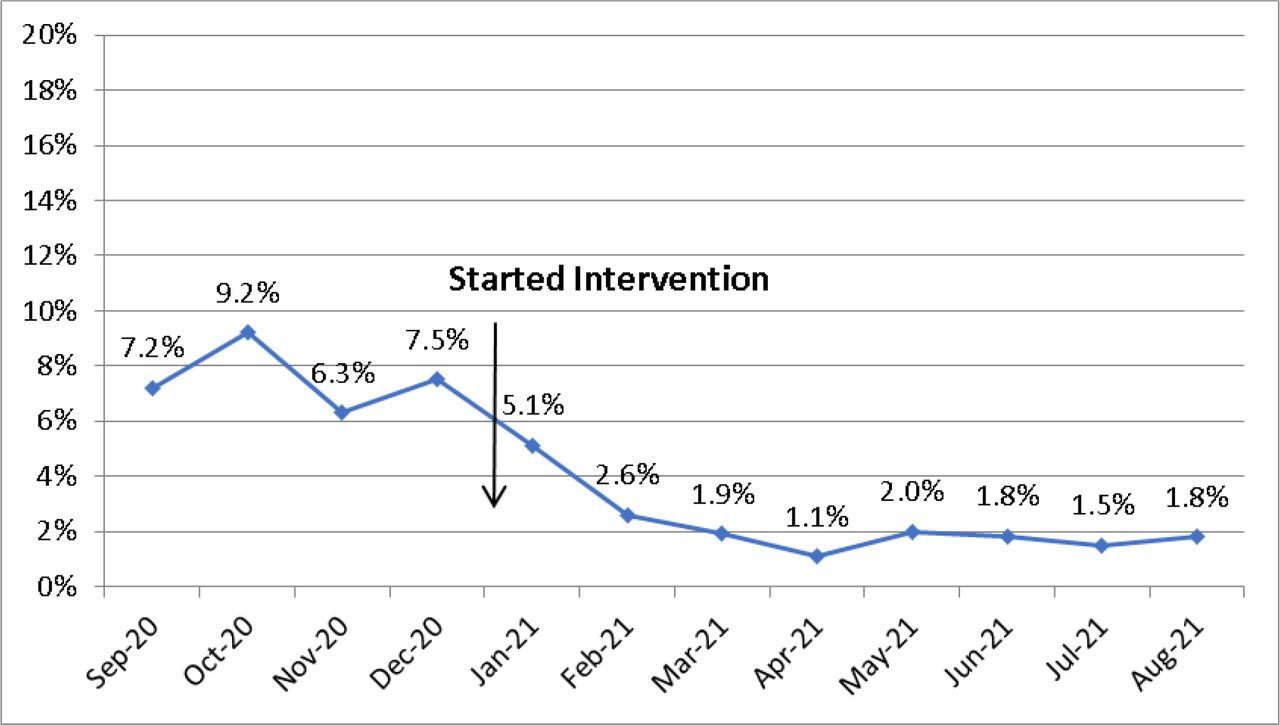
Comparison of blood culture contamination rate per month before and after intervention.
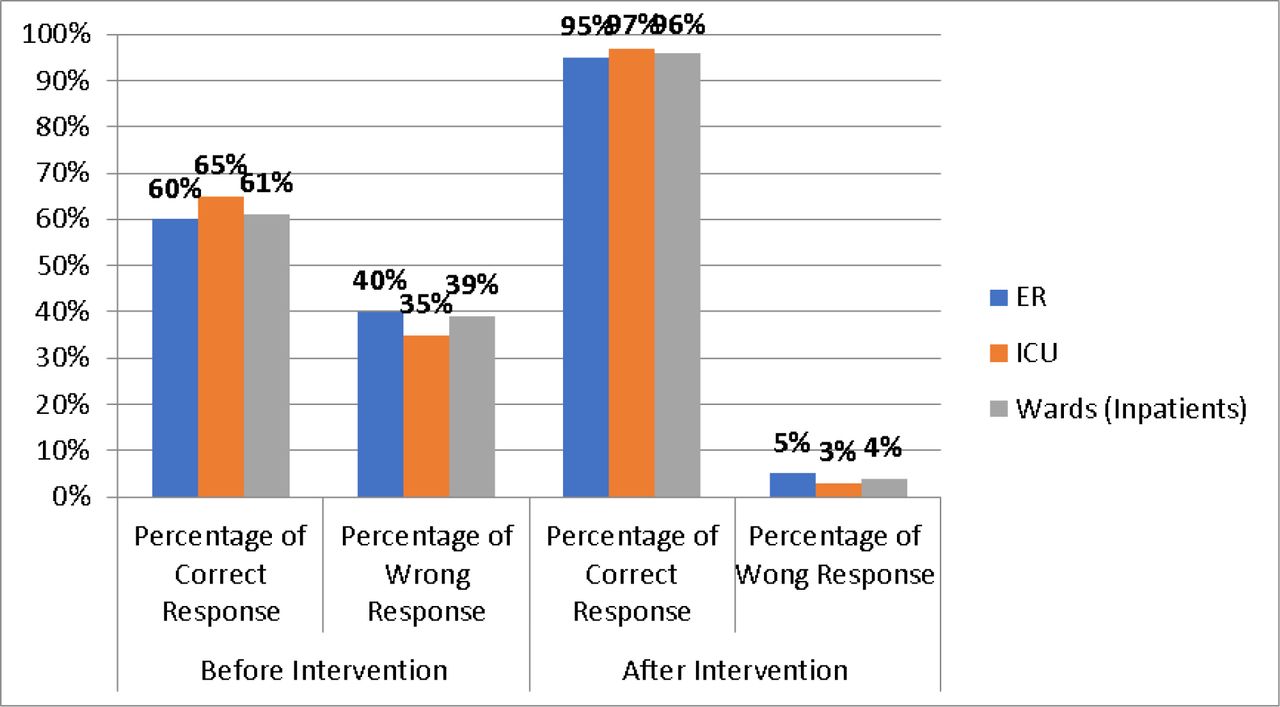
Average of correct and wrong responses of blood culture collection survey before and after intervention in each department
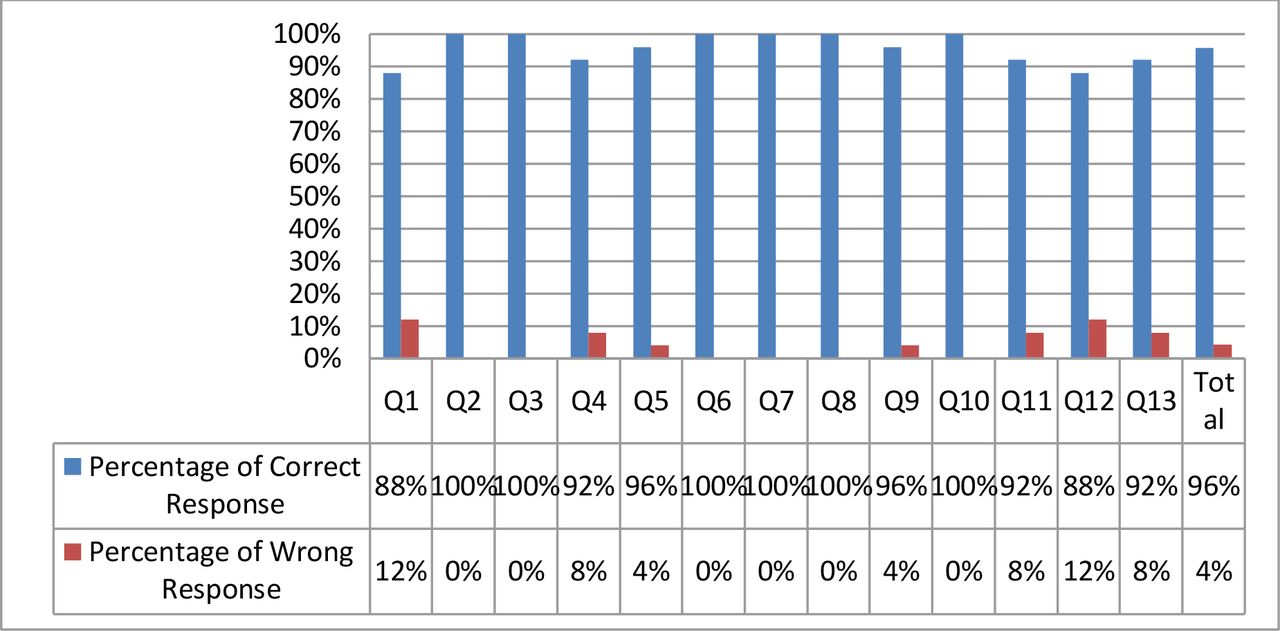
Briefly, table 2 and figure 13 show the averages of participants’ responses before and after interventions to give the reader a full idea about the success of our intervention programme in this project.
Average of correct and wrong responses to blood culture collection survey before and after intervention in each department

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Average of correct and wrong responses to the blood culture collection survey before and after intervention in each department. ER, emergency room; ICU, intensive care unit.
Comparison of blood culture negativity rate before and after interventions
Negative rate of blood culture before intervention was 96% and reduced after interventions to 91%, and this indicates that the physician’s awareness about blood culture indications has been improved.
Results summary
Overall improvement of knowledge and awareness of nurses in the ER from 60% to 95%, a total of 35% improvement rate.
Overall improvement of knowledge and awareness of nurses in ICU from 65% to 97%, a total of 32% improvement rate.
Overall improvement of knowledge and awareness of nurses in inpatient wards from 61% to 96%, a total of 35% improvement rate.
Overall reduction of BCC from average of 7.5% to 1.8%, a total of 5.7% reduction rate.
Overall reduction of blood culture negativity rate from an average of 96% to 91%, a total of 5% reduction rate.
Saving microbiology budget an estimated average of 10%–12% in 1 year.
Lessons and limitations
The BCC cannot be eliminated but can be reduced to the international benchmark (<3%). In our project, we have found that the most effective tools for succeeding this project were survey questionnaire, education and effective communication between the microbiology department and nursing. The second effective tool was to establish communication between our department and the medical departments to meet the goals of our project and to ensure the sustainability of laboratory services. Microbiology technologists have become more aware about the problem and how to communicate with the nursing department. The in charge of nursing department supported this project by enforcing the nurses to implement an ideal blood culture collection procedure. Good technique is sufficient to reduce the BCC and introducing sterile gloving techniques are not necessary. Optimal use of the blood culture by physicians lead to reducing the use of blood cultures in patients with a very low likelihood of bacteraemia, which result in higher positive blood culture rate and reduced costs associated with contamination.
Limitations
Hiring new nurses after intervention period who were not engaged in the effective training on the blood culture collection procedure lead to slight increase in the BCC rate. Therefore, we were able to train all the new junior nurses by activating the mandatory induction programme, which includes training on the proper blood culture collection procedure. Number of retaining nurses from vacations who missed the education and intervention procedure had negative impact on the project time due to repetition of such education programme for them. Unfortunately, there was no medical statistics available in our hospital. Therefore, we could not calculate the soft cost of medication, care and other resources used for patients who stay longer due to BCC issue.
Unexpected benefit
Reduction in the budget of the microbiology department was estimated to be 10%–12% per year as a result of BCC reduction.
Increase in the nurses’ satisfaction due to decrease in patient complaints as well as physician complaints and dissatisfaction.
Patient hospitalisation days were reduced as a result of our interventions, which lead to saving hospital resources and less pressure on the nurses in the wards.
Conclusions
BCC is a complex, challenging problem that requires a multidisciplinary approach. Well-conceived and effectively implemented strategies are important for reconciling sometimes-contradictory requirements of individual patient care, population health and effective resource allocation.
By standardising blood culture collection methods, optimising blood volume and nurses’ education, we were able to develop a best practice for blood culture collection and reduce BCC and negativity rate to a sustainable low rate at our hospital.
Our QI efforts are ongoing, and with order entry changes and further education, we anticipate our BCC rates will continue to decrease.
Monitoring and evaluation system should be a continuing process implemented by the microbiology department to document the improvement and success of this project.
Our team recommended that all new nurses should be oriented and trained on blood culture procedure before starting work.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Project intervention did not affect patient safety and quality of medical care. Also, it did not add any burden on the hospital budget or required any financial support.
Acknowledgments
We thank the hidden soldiers who helped in the success of this project (Ms Meiaad Ali Hindi, Ms Jamilah Saleh Gazwani, Mr Mahmoud Dugdugi and Mr Moataz Abu Faris) who supported us by all means.
Footnotes
Twitter @N/A, @Hesham9700
Contributors MAA was the team leader, guarantor and main author. AD designed the education programme and wrote and edited the manuscript. HGA-M responsible for the training programme/observation of training outcomes. HNH was involved with data collection and management. JS contributed with data collection and management. AA-B was involved with data management and nurse training. SE and AA-F were involved with the training of the physicians.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.