Article Text

Abstract
Length of stay (LOS) is a significant contributor to overall patient outcomes for patients undergoing liver transplantation. This study documents a quality improvement project aiming to reduce the median post-transplant LOS for liver transplant patients. We instituted five Plan–Do–Study–Act cycles with the goal of reducing LOS by 3 days from a baseline median of 18.4 days over 1 year. Balancing measures such as readmission rates ensured any decrease in stay was not associated with significantly increased patient complications. Over the 28-month intervention period and 24-month follow-up period, there were 193 patients discharged from hospital with a median LOS of 9 days. The changes appreciated during quality improvement interventions carried over to sustained improvements, with no significant variability in LOS postintervention. Discharge within 10 days increased from 18.4% to 60% over the study period, with intensive care unit stay decreasing from a median of 3.4–1.9 days. Thus, the development of a multidisciplinary care pathway, with patient engagement, led to improved and sustained discharge rates with no significant differences in readmission rates.
- Healthcare quality improvement
- Surgery
- Statistical process control
- Quality improvement
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
As the number of patients on the liver transplant waitlist increases, it is crucial to optimise liver transplants workflow efficiency in order to increase the feasibility and capacity for procedure and address the impact of chronic liver disease. There are no formal quality indicators for postliver transplantation processes, but length of stay is a well-supported measurement of how similar systems operate.
WHAT THIS STUDY ADDS
This study demonstrates an example of applying the Plan–Do–Study–Act quality improvement technique to decrease length of stay in postliver transplant population, with the exceptional results of a decrease in mean duration of post-transplant stay from 18.4 days to 9 days over the course of five cycles, with sustained results postintervention.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
By providing an example of how to apply quality improvement principles to length of stay in transplant setting, this study provides context for healthcare sites to consider employing similar strategies to develop a workflow to address length of stay. It also provides foundational support for continued research in length of stay reduction and suggestions for metrics to enhance the comprehensive nature of intervention evaluation.
Introduction
For patients with end-stage liver disease, the only curative option often available is liver transplantation (LT). LT volume continues to grow to meet the needs of the patient population, with 8906 transplants completed in 2020 in America, a record high.1 However, by the end of the year, there remained over 11,000 patients on the waitlist in need of LT.1 With the strain placed by a mismatch between donor pool and supply, it is critical that completed LT’s involve appropriate protocols to optimise patient outcomes and efforts are made for programmes to operate as high-quality health systems.
There are no formal guidelines regarding quality measures for LT to be used to assess the strength of an LT programme. The estimated operative costs of LT in Canada range from over US$$26 000 for in-province to over US$33 000 for out-of-province transplants when accounting for physician billing modifiers. Although the factors associated with the operative costs are difficult to address, the postoperative aspect of transplantation offers an opportunity to improve the patient experience and decrease the overall cost of LT.2 Over the past decade, there has been significant developments regarding quality-of-care measurements that can be applied to this field, and length of stay (LOS) has been considered as a potential benchmark indicator for LT quality, given its current use as a quality benchmark in medicine. There is some precedent for the benefit of targeting LOS, with a shorter LOS not only increasing procedure volumes, but also resulting in improved patient outcomes with fewer surgical complications.3 4 Furthermore, LOS post-LT has been considered a potential quality indicator for transplantation.5 Regarding factors impacting LOS, significant predictors of prolonged hospital stay (>8 days) include preoperative factors such as hospital admission, previous transplant, postoperative factors such as intensive care unit (ICU) admission, ventilator dependance, surgical site infection and intraoperative factors such as cold ischaemic time.6 In terms of capacity for improvement, the postoperative environment is best suited for targeted intervention to while retaining appropriate patient outcomes. Thus, our study focuses on reducing LOS post-LT with post-transplant interventions through a quality improvement (QI) workflow.
A benchmark LOS ≤18 days post-LT has been previously suggested in a multicentre study, however, individual centres have been able to achieve an LOS between 8 and 11 days. The London Health Sciences Centre (LHSC) had a median LOS of 18 days post-LT prior to completion of this project. In this project, we aimed to reduce LOS days by 3 days over a 28-month period using the model for continuous improvement.7
Methods
Context
The QI project was conducted at LHSC located in London, Ontario, Canada. The multiorgan transplant programme (MOTP) at LHSC performs 65–70 LT per year. We developed a multidisciplinary QI team, which consisted of relevant staff that are involved in the MOTP workflow. This includes transplant hepatologists, transplant surgeons, multiorgan transplant unit head nurse, nurse practitioners, social workers, physiotherapists and registered dietitians. Initial planning stage of project was initiated in July 2017 with a focus on addressing areas improvement regarding LOS. Patient workflow for post-transplant consists of transition to ICU, followed by discharge to MOTP unit. Regarding QI methodology, we chose to use the model for continuous improvement and instituted five Plan–Do–Study–Act (PDSA) cycles.
Aim statement
The aim of this project was to reduce the median LOS post-transplant from 18.4 days to 15.4 days (3 days) over a 1-year period.
Interventions
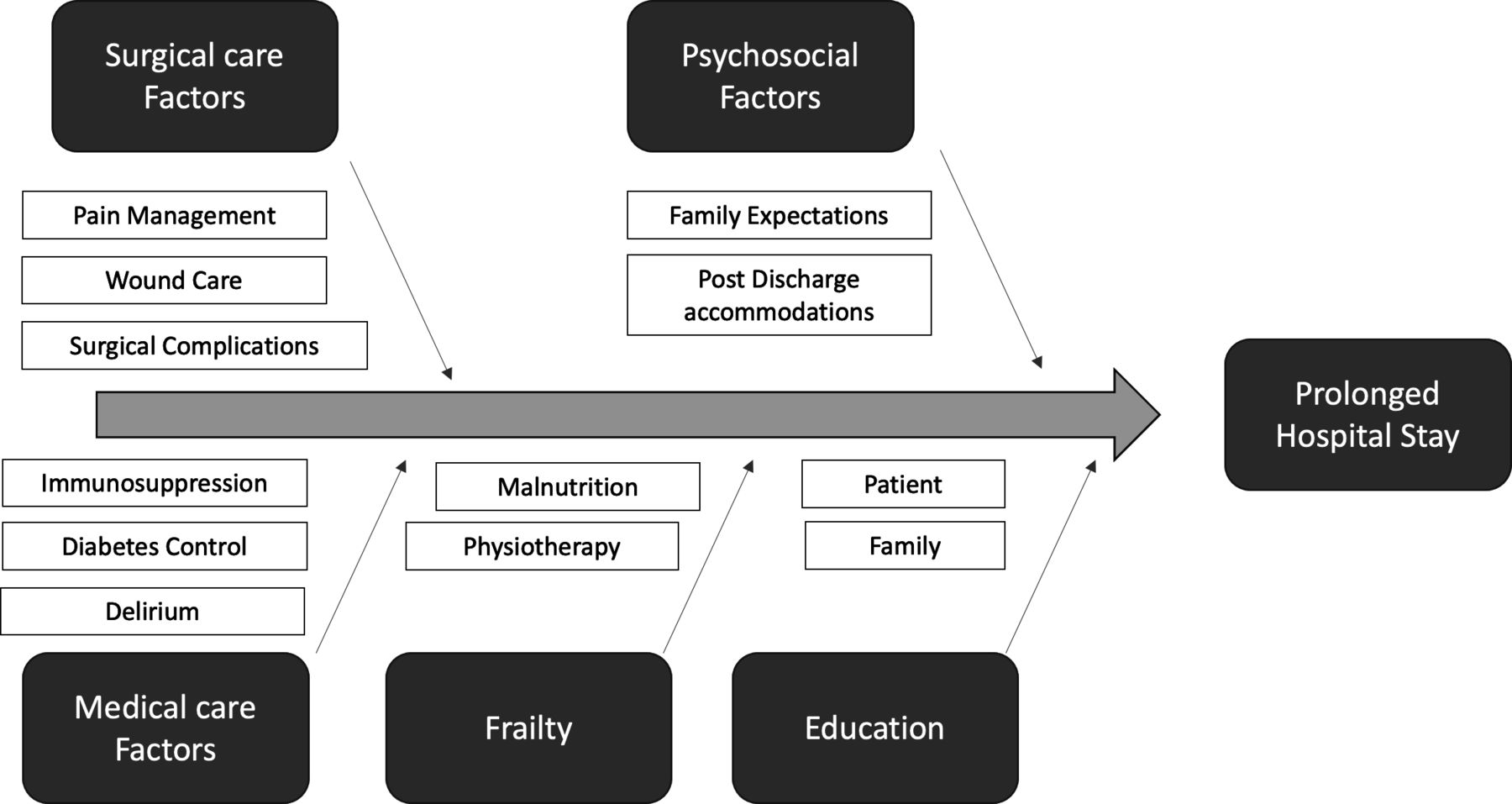
Prior to beginning the QI project, we completed a root cause analysis and identified factors associated with LOS as shown in an Ishikawa diagram (figure 1). We identified five core areas of focus, including surgical care factors, psychosocial factors, medical care factors, frailty and education. Our team met monthly to review data and evaluate feedback needed to help guide future PDSA cycles. PDSA cycles were then disseminated to all care providers during monthly Quality Assurance and Performance Improvement rounds. Overall, there was a 100% adherence to attendance (not including excused absences) for PDSA cycle review and planning meetings.

Ishikawa (fishbone) diagram showing factors related to prolonged hospital stay.
The first PDSA (n=23) cycle was started on August 2017–February 2018 and focused on educational sessions among LT team members and other specialists involved in the management of LT patients. We highlighted key post-LT factors including medical, surgical, psychosocial (including education) and frailty. This session was conducted through a presentation assembled by QI leads which outlined relevant factors and how they relate to patient care postoperatively. Content was sourced from completing a search for relevant literature regarding these factors, with the presentation involving a discussion regarding these studies and providing an overview of our existing protocols for post-transplant care and how they relate to these factors of patient health.
The second PDSA cycle (n=9) started on February 2018–April 2018 and involved an LT clinical pathway started from day 0 to day 10 after post-LT. This was initially developed following our monthly meetings based on stakeholder input regarding the optimal clinical pathway for LT post-transplant workflow. The clinical pathway outlined the specific expectations regarding management for LT patients and the necessary referrals for consultations and allied health professional involvement that should be completed within the first 10 days, attempting to increase compliance to timely integrated care. For further detail, this has been provided in (online supplemental file 1). Some of the components of this clinical pathway that were set out included physiotherapy involvement on postoperative day (POD) 0 for assessment and progression to movement, nurse involvement for medication teaching on POD 1, surgical fellow involvement on POD 2 to remove foley, and access to a registered dietician to ensure a feeding plan was initiated shortly after LT. Once our initial patient pathway was completed, no further changes were made to it during dissemination . Roll-out involved a patient path being placed in patient rooms, as well as on the nurse’s flow sheet for reference. For staff that consistently work in the MOTP, one-on-one conversations were had to engage them in the study, with the involvement of a nurse education from the MOTP. Regarding additional allied healthcare staff, it was sent as an email.
Supplemental material
The third PDSA cycle (n=14) started on April 2018–July 2018 involved instituting a clinical order set in our electronic medical records. We recognised that for our interventions to be effective there needed to be appropriate uptake by the medical professionals involved in decision making for ongoing management of patient care. The clinical order set integrated orders that were part of patient management into a grouped set for increased efficiency and streamlined workflow. As was the case in cycle development throughout project, stakeholder input was involved in generating order set. Further, this cycle also involved a clinical informatician. Decisions regarding content of order set were confirmed with senior author after drafting based insight from stakeholders. For further detail regarding the order set generated by our team, please refer to online supplemental file 2. The purpose of developing this workflow was to increase the utility of the pathway, as an easier to use pathway was more likely to be adhered by involved stakeholders. Use of order set was assessed through study’s family of measured variables and impact on LOS as seen in run chart.
Supplemental material
The fourth PDSA cycle (n=37) started July 2018–April 2019 as we recognised that patients and family members expectations were at times discordant with the goals of the medical team for assessing for earlier discharge given the perceived grandiosity of LT. For example, patient families would often prefer patients remained in the hospital for longer feeling this was directly related to the patient’s recovery. Furthermore, patient’s families would often also suggest modifications to the patient’s discharge plan to develop a plan that may be more convenient for home-planning but difficult to coordinate such as a patient discharge being delayed from Friday to Monday. We felt we could manage these expectations with a patient oriented clinical pathway. Our patient-oriented clinical pathway involved an education-focused intervention, occurring prior to the LT itself. This clinical pathway focused on educating family members regarding our model for care and the criteria for discharge, along with the benefits of early discharge and the process of assessment prior to discharge to improve confidence in our model. The patient education intervention was delivered each time in a standardised manner by a nurse educator who worked with MOTP. If the interaction was occurring between another member of the medical team and the patient’s family—the MOTP nurse would remain to observe. Through this involvement, the nurse practitioner was able to help guide conversations towards the educations focused protocol if deviated and help support consistency between interactions.
The fifth PDSA cycle (n=30) started in April 2019–Dec 2019 as we recognised there were often logistic barriers for discharge. These barriers were often associated with processes involved in patient preparation post-LT for management as a LT patient, such as poor adherence to medication, limited understanding of diabetes management and no preplanned discharge transport. Rather than direct a specific individual for each specific need, we developed a list of goals for patient postoperative education and discharge planning that was distributed to the team as well as the MOTP charge nurse. These included goals such as improving patient understanding of medication and initiating supports for medication delivery if required (such as blister packs), as well as developing a plan for discharge disposition prior to initiating procedural workflow. Thus, the focus of this cycle was to adapt the role of MOTP charge nurse to identifying these gaps in compliance through daily involvement in morning rounds, at which point the charge nurse would be able to highlight needs to be addressed by the remainder of MOTP team.
Family of measures
Prior to initiation of study, the team agreed on the essential family of measures. The primary outcome measure for this study is the LOS post-LT, defined as the duration (in days) from day of admission to ICU post-LT until the day of discharge from the MOTP inpatient unit. We did not evaluate whether patients were repatriated to hospital, home or other long-term care units (such as the geriatric rehabilitation unit) as this was dependent on other external factors, such as bed availability, and majority of patients were discharged directly from the MOTP unit to home. A secondary outcome measure was ICU LOS, defined as duration from the day of admission to ICU and transfer to the MOTP inpatient unit. Primary balancing measure for this project was readmission rate, recorded as 30-day and 90-day rates, with the goal of ensuring that patients who were being discharged through our workflow were not facing increased complications. Readmission rate was defined as the number of recipients readmitted to LHSC following discharge after LT divided by the total number of patients discharged. Comparison of readmission rates was done through two-sample z test of proportions. Data collection was done retrospectively to ensure safety was always maintained and to avoid premature discharges. Fidelity measures for the study included attendance to meetings regarding review and planning, based on the PDSA cycle structure.
Baseline analysis
Our baseline data collection took place between January 2015 and August 2017. We captured data regarding initial date of transfer to ICU post-LT, the date of transfer from ICU to the MOTP inpatient service and the date of discharge. We also captured any 30-day or 90-day readmissions required for patient, as part of our balancing measures. Of note, there was a single special-cause variation event associated with the baseline for this project, which was an outlier, representing a month with an n=1 including a patient with a prolonged stay of 71 days postoperative, and thus was not accounted for when confirming baseline stability of variation.
Statistical analysis
Mean per-month LOS was plotted on a Statistical Process Control (SPC) Chart using QI Macros.
Results
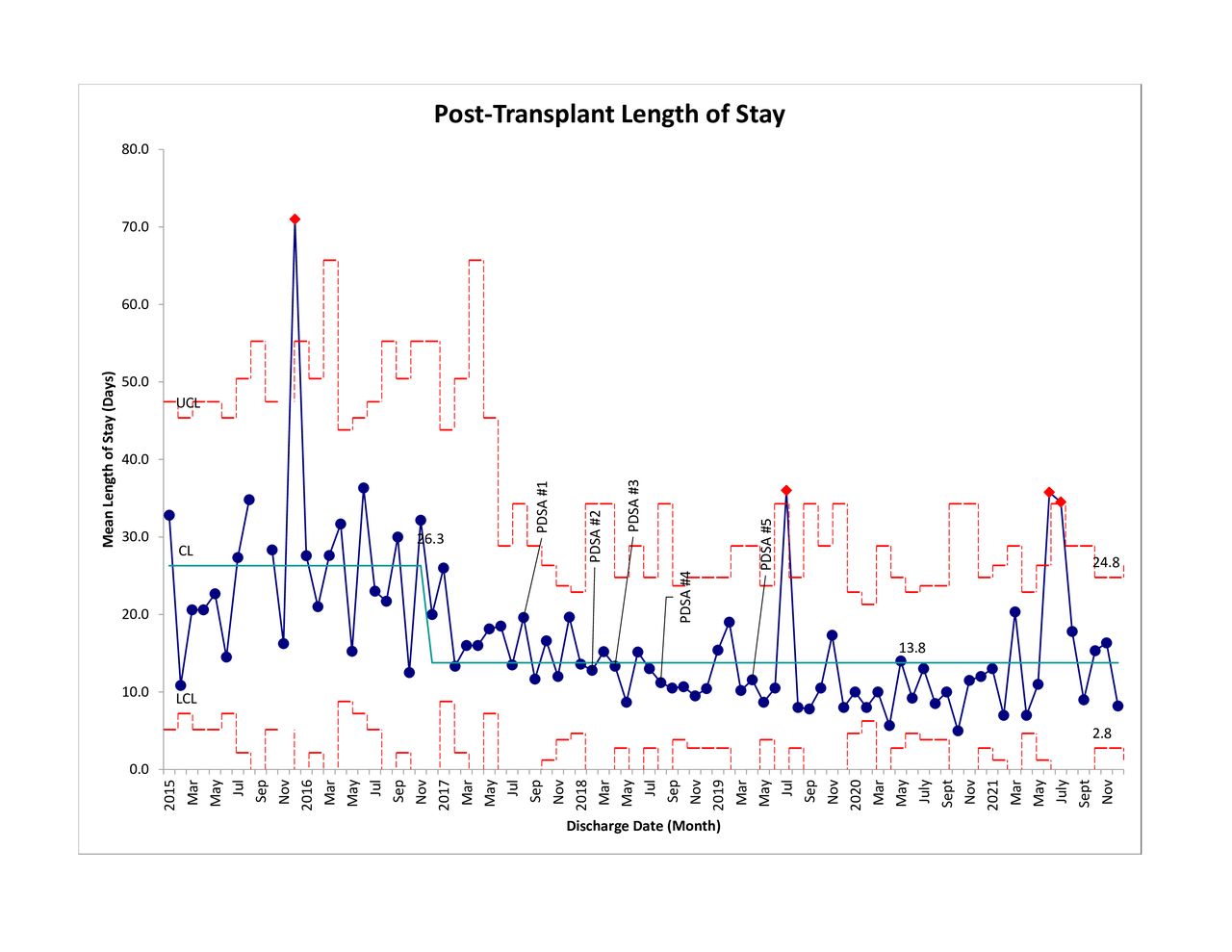
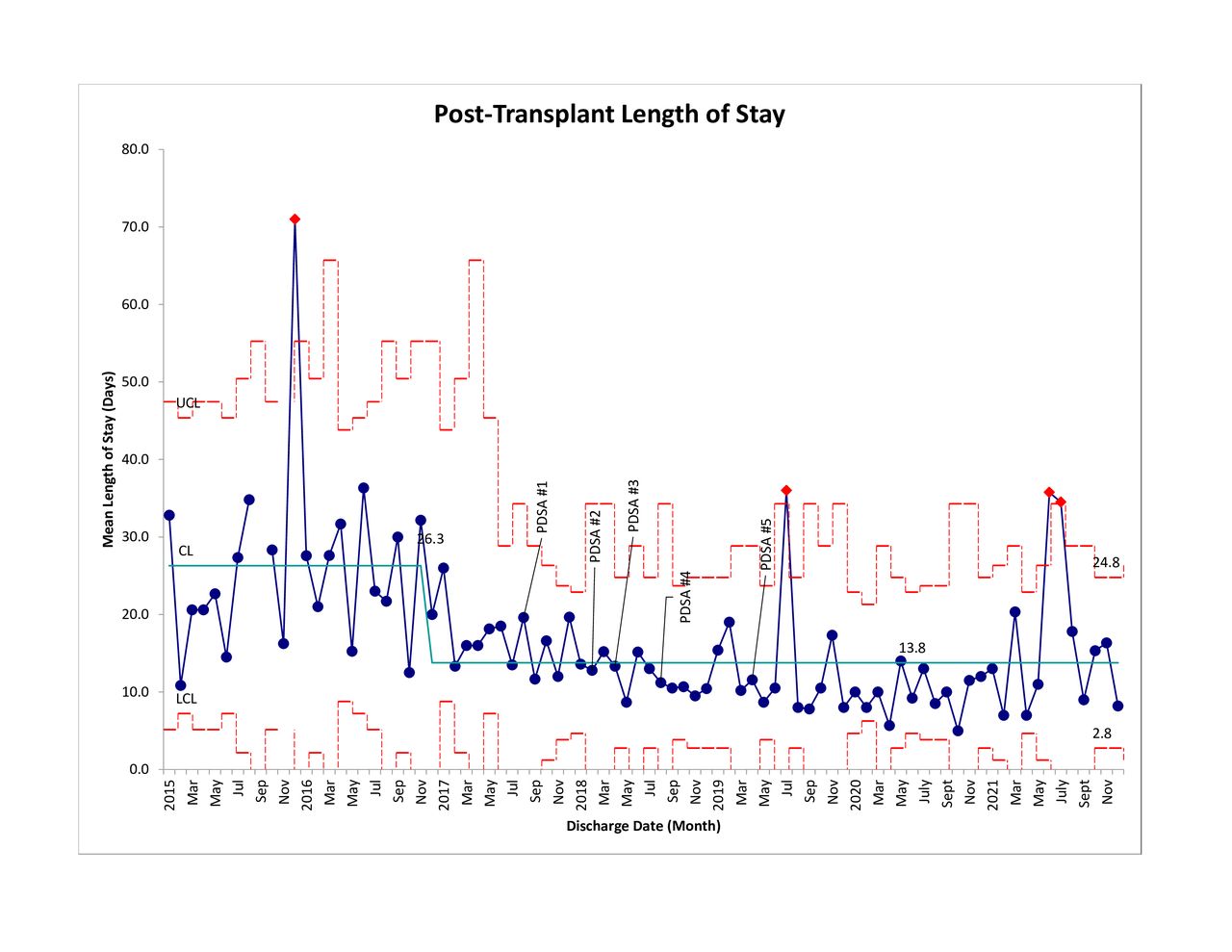
Results were plotted on an SPC chart (figure 2). Prior to our QI inititative, the median LOS post-LT (n=130) between January 2015 and August 2017 was 18.4 days. Over a 28-month period during which PDSA cycles were completed, 113 LT patients were discharged from the hospital with a median LOS of 9.0 days. The median sample size for each month was 4 (IQR 3–5). The LOS post-LT was sustained for 24 months after the PDSA cycles were completed, over which 80 LTs occurred. The 30-day and 90-day readmission rates, used as balancing measures, were determined to be 19.0% and 25.6%, respectively, compared with 15.4% and 22.7% in baseline assessment period, with no significant difference with p>0.05. Preintervention, discharge within 10 days occurred in 18.4% of patients but increased to 60% over study period. ICU LOS also decreased throughout study period from a median of 3.4 days preintervention to 1.9 days.
{kind=link}
{kind=link}
Statistical process control chart demonstrating monthly mean LOS at baseline observation period, during Plan–Do–Study–Act (PDSA) cycles, and postquality improvement intervention in long-term observation. Demonstrates upper control limit and lower control limit. LOS, length of stay.
Discussion
Over the course of this study, using the model for continuous improvement, we were able to decrease and sustain the median post-LT LOS by 9.0 days with no significant increases in readmission rates at 30 and 90 days. This project offers an example of the feasibility of initiating such QI projects at LT centres with an account of potential stakeholders and ideas for driving change in a sustainable and practical manner.
The SPC chart identifies an interesting trend, suggesting change to the underlying process began in March 2017, preceding the initial PDSA cycle in August 2017. This is a known limitation of this study, and there is no definitive explanation for this phenomenon but, we surmise changes were associated with an influential surgical member joining the transplant team around this period. We believe the addition of staff is unlikely to be the primary driver of the changes seen as each staff will only rotate on-service every 4 weeks. Moreover, it is unlikely such sustainability is consistent with a single staff change as it continues to persist throughout intervention and postintervention whether staff was on service or not. Furthermore, there was a high compliance rate for team involvement in PDSA cycles, with strong fidelity measures increasing the likelihood for our intervention to be associated with changes appreciated in study. We believe the most likely cause for the efficacy of our interventions is the multifaceted approach which was applied and the high degree of compliance. As we had built interventions to target different touch points of care, we were gradually able to build a culture of change where majority of staff were cognizant of the goals and aware of the evidence supporting the utility of maintaining these behaviours. Regarding individual cycles, it is likely the cycles that adjusted workflow, such as PDSA cycle 3, were more likely to result in a sustainable change in comparison to education-based cycles as they generated a lasting product. This is consistent with existing research reviewing measures for QI improvement in Hepatology, which demonstrate workflow-associated changed are more frequently successful, whereas education-based initiatives are less likely to generate sustainable impacts.8
A common limitation regarding QI projects is the Hawthorne effect, and previous studies have demonstrated a return to mean values often occurs between 10 and 15 observations after the initial change is made.9 In comparison, the decrease in LOS in our study was maintained over a 24-month follow-up period, with no significant change in median LOS. While some special-cause variation occurred, this is expected with a small sample size and a population with highly variable data, given patient potential to decompensate postoperatively, resulting in prolonged stays. Additionally, we believe that future studies should consider additional measurements and direct formalised feedback to assess the efficacy of educational interventions, as this was not included within our family of measures. Further, we did not account for measures specific to the patient perspective. LOS has been evaluated as a factor in patient satisfaction, with recent surgical studies demonstrating prolonged LOS associated with decreased patient satisfaction and likelihood of recommending hospital to others.10 Although this would suggest that being decreasing LOS would result in increased patient satisfaction, we did not confirm this through our work and this should be considered in future studies to develop a comprehensive evaluation of the utility of the initiative.
By using the model for continuous improvement, we were able to decrease the median LOS post-LT by 9.0 without significantly impacting 30-day and 90-day readmission rates. Our study demonstrates a promising proof-of-concept regarding the application of QI principles to addressing LOS in post-LT patients. Our intention on the onset of study was to develop a model that is feasible and practical. Interventions were generated as to mitigate costs for the home programme and relied on optimising existing processes. Thus, this model can be considered for application to other areas of surgical management as it has a low opportunity cost for execution. It also demonstrates an approach that does not require a large team with QI knowledge, as majority of our cycles required only a QI lead with understanding of the field, and remainder of the team having minimal training in QI. For centres with a low number of staff with formal training, this can be reassuring and encourage them to consider applying their own QI initiatives using their insight into workflow and factors impacting patient care.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This project was classified as a QI investigation based on the requirements listed in the Tri-Council Policy Statement, thus, ethics approval was waived by local research ethics board. Patient confidentiality was protected throughout, and all data analysed was deidentified.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @agob2007
Contributors Study design: AA, CW and MB. Data analysis: YS, AA, AG, CW and MB. Manuscript writing: YS, AA, AG and MB. Editing/review: YS, AA, ET, AT, KQ, AS and MB. Study Guarantor is MB.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.