Article Text

Abstract
Anaesthesia is associated with the routine use of volatile anaesthetic agents, all of which are potent greenhouse gases in varying degrees. Desflurane, in particular, has a high global warming potential and in recent years, there has been a global movement to reduce or remove its usage entirely from operating theatres. We work in a large tertiary teaching hospital in Singapore with deeply entrenched practices of using desflurane to facilitate high turnover of operating theatre cases. We launched a quality improvement project to (1) reduce the median usage of desflurane by 50% (by volume), and (2) reduce the number of theatre cases administering desflurane by 50% over a period of 6 months.
We collected baseline data to determine departmental monthly median usage of desflurane. We then deployed sequential quality improvement methods to educate staff and to eliminate misconceptions, as well as to promote a gradual cultural change.
We successfully reduced monthly median desflurane usage from 31.5 L to 12.2 L per month (61.3% reduction) within our targeted time frame. We also achieved a reduction in the number of theatre cases using desflurane by approximately 80%. This translated to significant cost savings of US$195 000 per year and over 840 tonnes of carbon dioxide equivalents saved.
Healthcare is a resource intensive industry. Anaesthetists are well placed to play an important role in reducing healthcare-related carbon emissions by choosing anaesthetic techniques and resources responsibly. Through multiple Plan-Do-Study-Act cycles and a persistent, multifaceted campaign, we achieved a sustained change in our institution.
- anaesthesia
- quality improvement
- PDSA
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Desflurane is a harmful greenhouse gas with a much higher global warming potential than other commonly used anaesthetic agents. It is popular in contemporary clinical practice due to its favourable pharmacokinetic properties, particularly in facilitating rapid emergence from anaesthesia.
WHAT THIS STUDY ADDS
There is increasing evidence showing that desflurane does not produce statistically significant improvements in patients’ recovery profile or anaesthetic-related respiratory complications compared with other anaesthetic agents. Our project demonstrated that systematic and successive application of quality improvement methods can be effective in reducing desflurane usage.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our study resulted in environmental benefits and substantial cost savings to our institution. We hope that our methodology can be applied to other local and foreign healthcare clusters, as part of the global movement towards sustainable and environmentally conscious anaesthetic practice.
Problem
Desflurane is a commonly used modern inhalational anaesthetic agent that debuted into clinical practice in the 1990s. Along with sevoflurane, it quickly gained popularity and displaced other inhalational agents such as isoflurane and enflurane due to its fast onset and offset of action with minimal adverse pharmacokinetic and pharmacodynamic effects. At the time, desflurane and sevoflurane were touted as more environmentally friendly agents due to their completely fluorinated molecular structure. This meant that they had low ozone depleting potential compared with their chlorine-containing counterparts.1
We have since discovered that this is not true. Both sevoflurane and desflurane are greenhouse gases through absorbing infrared radiation of different wavelengths and releasing them as heat energy. Complete fluorination of their molecules renders them less flammable and less reactive as the C-F bond is very stable; however, the process inadvertently makes them harder to break down in the environment. Desflurane, in particular, has a high global warming potential with a GWP100 (global warming potential over 100 years) of 2540. Its carbon footprint is up to 40 times higher compared with sevoflurane. Using an hour of desflurane at one minimum alveolar concentration at a fresh gas flow rate of 2 L/min is equivalent to driving 650 km in a car. In the same patient, if sevoflurane was used, this distance would be reduced to 13 km. It also lingers in the atmosphere much longer, 14 years versus 1.1 years for sevoflurane.2
Background
We launched a quality improvement project (QIP) to reduce departmental usage of desflurane to primarily reduce our carbon emissions and to secondarily improve theatre cost-effectiveness. Our hospital is a large 1200-bed tertiary teaching hospital in Singapore which provides service in every surgical subspecialty including cardiothoracic, transplant, paediatric, trauma and orthopaedic surgery. Our theatre activity consists of approximately 25 000 general anaesthesia cases per year. Usage of desflurane was high with its perceived benefit in facilitating rapid turnover of theatre cases.
Before the project was launched, departmental usage of desflurane and sevoflurane was 369 and 352 L per annum, respectively (based on pre-pandemic data in 2019). This translated to 1400.6 and 77.1 tonnes of carbon dioxide equivalents (CO2e) per annum generated for each of them. This was in contrast to UK hospitals’ average desflurane and sevoflurane usage: 110 and 291 L per annum, respectively (based on 2018 data).3 The costs of desflurane and sevoflurane per annum was US$340 500 and US$124 200, respectively. Financially, reducing desflurane usage by 50% could theoretically save our hospital US$150 000 per annum.
Methods
The quality improvement (QI) team consisted of a group of anaesthetists (from senior consultants to residents), a pharmacist and a neutral facilitator. The project was carried out over three phases, from March 2021 to April 2022. Ethics approval was deemed not required as data was collected as part of a QIP. Our primary objective was to reduce desflurane usage by 50% (by volume) over a period of 6 months. Our secondary objective was to reduce the number of theatre cases using desflurane by 50% over a period of 6 months.
Phase 1: pre-intervention phase
We collected data from the Department of Pharmacy to determine baseline median monthly usage of desflurane, sevoflurane and propofol (in volumes) over the year of 2019 and from October 2020 to April 2021. We deliberately avoided data collection from January to September 2020 as the number of theatre cases were disproportionately low due to the COVID-19 pandemic. We further collected baseline data over a week in March 2021, targeting all general anaesthetic cases performed in our hospital. It showed:
440 general anaesthetic cases, out of which 55 case notes were missing
Out of the remaining 385 cases—51% used sevoflurane, 31% used desflurane and 18% used total intravenous anaesthesia (TIVA).
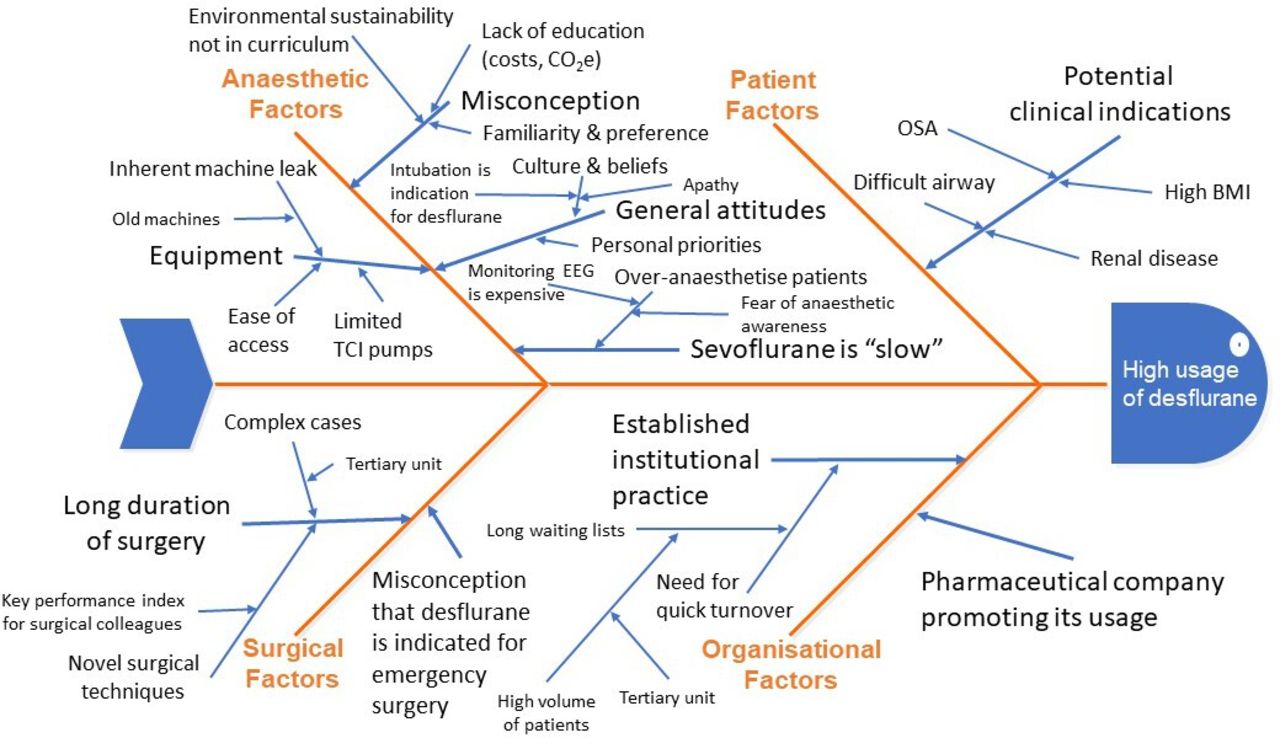
At the QI team meeting, we discussed the stakeholders’ expectations (box 1) and mapped out the current patient’s perioperative pathway. We performed a root cause analysis and constructed a fishbone diagram based on identified patient, anaesthetic, surgical and organisational factors that led to high desflurane usage (figure 1).

Fishbone diagram identifying affinity factors that lead to high desflurane usage. BMI, body mass index; CO2e, carbon dioxide equivalents; EEG, electroencephalogram; OSA, obstructive sleep apnoea; TCI, target-controlled infusion.
Stakeholders’ expectations
Patients
Every healthcare professional should take responsibility in providing an environmentally friendly and sustainable healthcare service, while upholding an excellent standard of care.
Staff
Staff would like to deliver a patient-centred service, with reasonable efficiency. They would prefer to avoid working overtime by minimising unexpected delays, as well as avoiding patient complications.
Organisation
As a public sector hospital, the organisation has a duty to the people, country and Intergovernmental Panel on Climate Change to reduce its carbon footprint in line with the Singapore Green Plan 2030 and the Paris Climate Agreement. It would seek to optimise patient flow while maximising profit margins.
As three times less sevoflurane is required to keep patients anaesthetised, it is financially more tangible to use it routinely compared with desflurane, which provides little benefit except in patients with certain medical conditions.
Potential patient factors identified for high desflurane usage included high body mass index (BMI), obstructive sleep apnoea and difficult airway. These patients are at a higher risk of perioperative respiratory complications and desflurane was perceived to be beneficial with its ability to produce rapid onset and offset of anaesthesia. Within our department, some clinicians choose to use desflurane in patients with renal impairment to avoid the theoretical risk of sevoflurane-induced nephrotoxicity. Some anaesthetists also favour desflurane for emergency theatre cases to facilitate quick theatre turnover in the context of high volume emergency theatre lists.
We further used the Pareto analysis to determine the top three causative factors and planned our interventions to specifically target these factors:
Lack of education
General attitudes
Ease of access.
Phase 2: interventions
We used the Model for Improvement and conducted three Plan-Do-Study-Act (PDSA) cycles.
PDSA cycle 1 (April–May 2021)
Our initial plan was to educate and to raise awareness. Prior to our intervention, we conducted a baseline survey to determine general attitudes within the operating theatre department. We received 225 responses (including theatre nurses and allied healthcare professionals). A total of 98.7% of survey participants stated that they were willing to put in additional effort to provide more environmentally sustainable healthcare. We delivered a ‘Like Desflurane? Let’s Refrain!’ talk with a quiz to discuss the environmentally harmful effects of desflurane and to provide a comparison between our hospital and other local and foreign institutions.
This intervention led to a decrease in monthly desflurane usage from 31.2 L to 19 L. A post talk survey showed that 60% of survey participants had either reduced or stopped using desflurane completely since the talk. We received 45 responses to the survey (out of 80 talk participants), of which 55.5% were consultant grades and above. The majority of survey participants indicated that they felt anaesthetists should be role models and lead the way towards delivering a greener healthcare service. Following the talk, we launched a ‘Greening the Operating Theatre’ bulletin in the cluster newsletter to consolidate knowledge and to provide information to those who missed the talk.
PDSA cycle 2 (May–June 2021)
We decided to obtain international opinion regarding environmentally sustainable anaesthesia to further raise awareness. We invited an esteemed speaker (Dr Tom Pierce, Environmental Advisor to the President, Royal College of Anaesthetists) to speak about this topic in the context of Singapore. We hypothesised that launching other ‘Greening the Operating Theatre’ initiatives concurrently might foster a culture change more effectively by creating a more immersive experience. We proposed and initiated a series of other changes in operative theatres, including waste segregation for recycling and replacing single use cups and cutlery in the pantry. We worked with the multimedia department to produce virtual banners and screensavers to publicise our movement and to nurture a sense of collaboration. We formed an informal environmental group within the department to encourage others to participate and to contribute ideas.
We intended to propose relocating desflurane vaporisers from operating theatres to inactive anaesthesia rooms to restrict its easy access. We presented this idea at the anaesthesia department Senior Staff Meeting and received mixed reactions, with some citing that this demonstrated a lack of trust and could compromise a clinician’s authority. At the same meeting we also proposed developing a consensus guide for the use of desflurane. The department voted against producing a prescriptive guide, partly to maintain clinicians’ judgements and to avoid its unnecessary usage. They did, however, come to an agreement on its top three clinical indications: high BMI (BMI more than 30 kg/m2), obstructive sleep apnoea and prolonged surgery (more than 4 hours).
In this PDSA cycle, our monthly desflurane usage initially increased from 19 L to 25 L, and subsequently fell to 11.5 L. The temporary increase might have been a reflection of pushback that our campaign received. We conducted another survey post presentation. We received 45 responses (out of 65 meeting attendees), with 33.3% of survey participants voting against relocating desflurane vaporisers from operating theatres to non-operational anaesthesia rooms.
The QI team listened to feedback and adopted a gentler approach to retain morale and to promote a gradual cultural change. At another Senior Staff Meeting, we suggested unplugging the desflurane vaporisers instead when not in use to reduce electricity consumption. We continued to publish ‘Greening the Operating Theatre’ bulletins as a regular quarterly newsletter to update the department on the results of our project and to serve as an educational tool. We also recorded a series of webinars with Dr Tom Pierce to broadcast them in future departmental teaching sessions.
PDSA cycle 3 (July–August 2021)
We continued to seek methods to sustain the changes that we had achieved. We introduced attractive stickers on the anaesthetic machines to highlight the GWP100, CO2e and costs of sevoflurane versus desflurane. We proposed to the National Chief Examiner to incorporate examination questions on environmentally sustainable anaesthesia in the residents’ exit examinations. We accompanied this with ad hoc tutorials given to senior residents on topics related to sustainability. We delivered another departmental talk regarding the concept of minimum alveolar concentration to drive the transition towards using sevoflurane and TIVA. We also worked with other parties to procure more target-controlled infusion pumps and dedicated TIVA lines to minimise barriers to conducting TIVA.
Our median monthly desflurane usage stayed low at 12.3 L. We began receiving negative feedback from a pharmaceutical company regarding our low procurement rates. We held firm and welcomed the discussion of potentially introducing vapour capture technology to recapture and reprocess desflurane.
Phase 3: post-intervention phase
This phase took place between September 2021 and April 2022. We continued to monitor monthly usage of desflurane and assessed the impact of our interventions. The patient’s perioperative pathway was modified to include consideration of environmental impact when formulating an anaesthetic plan. It also included recommendations to reduce total fresh gas flow rates and total volatile anaesthetic usage as guided by depth of anaesthesia monitoring devices.
We collected data over another week in September 2021, targeting all general anaesthetic cases to determine if our secondary objective was met. In the near future, we plan to conduct an anonymised patient survey to investigate patients’ opinions regarding environmentally sustainable healthcare and their preferred type of anaesthesia.
Results
We achieved our primary objective within 3 months after the intervention phase began (see figure 2). Monthly median desflurane usage was sustainably reduced from 31.5 L to 12.2 L per month (61.3% reduction) over a period of 12 months (from May 2021 to April 2022). The results remained the same after adjusting them per capita. The volume of desflurane used per 1000 cases reduced from 16.7 L to 7.2 L per month (57% reduction).

{kind=link}
{kind=link}
Impact run chart demonstrating the reduction in desflurane usage. CO2e, carbon dioxide equivalents; OT, operating theatre; PDSA, Plan-Do-Study-Act; RCoA, Royal College of Anaesthetists.
Interestingly, departmental usage of sevoflurane also decreased from a median of 31.5 L to 27.8 L per month (11.7% reduction) over the same time frame. We propose that this was due to a departmental shift towards using low-flow anaesthesia. Operating theatre usage of TIVA increased as demonstrated by increased theatre median usage of large 50 mL propofol vials from 2022.5 vials to 2427.5 vials per month (20% increment).
A 1-week analysis repeated in September 2021 showed:
392 general anaesthetic cases, out of which 62 case notes were missing
Out of the remaining 330 cases—66% used sevoflurane, 6% used desflurane and 28% used TIVA
We achieved a reduction in the number of theatre cases using desflurane by approximately 80%.
Our QIP resulted in US$197 500 less spent on desflurane over the 12 months from when intervention strategies began. Taking into account the reduction in median usage of sevoflurane (further cost savings of US$7500) and the increment in median usage of TIVA including large propofol vials and other consumables (an added expense of US$15 000), we achieved overall cost savings of US$190 000. We did not include the cost of depth of anaesthesia monitoring devices as these equipment are widely available and their consumables are not charged to our department. We do recognise that modified electroencephalogram strips constitute the bulk of TIVA running costs; however, such costs dwarf in comparison to that of administering desflurane. From a carbon footprint standpoint, our QIP amounted to approximately 840 tonnes of CO2e saved, which is equivalent to driving 6 million kilometres in a small car or going around the planet Earth 150 times.
Discussion
Desflurane has long held the purported benefits of maximising operating theatre turnover while concurrently affording low perioperative complication rates, particularly in high-risk patient populations. It provides a stable and rapid onset and offset of anaesthesia by virtue of its unique physicochemical properties: a low blood gas partition coefficient (0.42), coupled with minimal liver metabolism (0.02%).
However, there is now a growing body of evidence that calls into question the validity of its clinical indications, given its high costs and high GWP100. A 2005 meta-analysis comparing postoperative recovery after sevoflurane and desflurane anaesthesia reported that patients were extubated a mere 1.3 min sooner following desflurane anaesthesia (duration of anaesthesia ranging from 19 min to 3.1 hours). This did not translate to any significant difference in time spent in the post-anaesthesia care unit.4 In a 2020 randomised trial comparing bispectral index (BIS)-guided sevoflurane and desflurane anaesthesia in obese patients, there was no difference in time to extubation (9.2 min vs 10 min for sevoflurane and desflurane, respectively, p>0.05); while patients in the sevoflurane group achieved baseline preoperative mini-mental state examination scores 11 min sooner than the desflurane group (40 min vs 51 min, p=0.001).5
Comparing postoperative outcomes, a 2020 randomised trial comparing short-acting anaesthetic agents (desflurane–remifentanil combination) and standard agents (sevoflurane–fentanyl combination) did not find a significant difference in postoperative apnoea–hypopnoea index scores up to the third postoperative night.6 More than 80% of patients in both groups had a formal diagnosis of obstructive sleep apnoea, based on the preoperative polysomnography apnoea–hypopnoea index. A 2021 single-centre cohort study incorporating data from over 100 000 cases of general anaesthesia using sevoflurane and desflurane did not demonstrate a reduced risk of postoperative respiratory complications following desflurane anaesthesia (adjusted OR 0.99, 95% CI 0.94 to 1.04, p=0.598). This was demonstrated even after propensity matching and subgroup analysis in morbidly obese patients and patients at elevated risk of respiratory complications.7 Together, these studies are consistent with our belief that the titration and timing of anaesthetic administration are more important than the choice of anaesthetic agent itself. Finally, there has been no evidence of nephrotoxicity caused by inorganic fluoride or compound A generated from sevoflurane metabolism. This was most recently studied in a 2017 meta-analysis, which showed that low-flow sevoflurane anaesthesia does not alter renal function, even in patients with pre-existing renal disease.8
The results that we achieved from our QIP is in parallel with efforts in other centres elsewhere in the world. In the UK, the Greener National Health Service programme is committed towards achieving net-zero carbon emissions; and has reported a significant reduction in desflurane usage, from 23.1% in 2018–2019 to 10.3% in 2020–2021.9 Individual centres have performed better than others, with complete removal of desflurane vaporisers and nitrous oxide cylinder manifolds at Freeman Hospital, Newcastle, since December 2021.10 In the USA, the American Association of Anaesthesiologists has published guidelines on environmental sustainability for anaesthetic practice,2 and many hospitals have since reduced or eliminated the use of desflurane in their operating theatres, along with adopting various other measures to mitigate the negative environmental impact of their anaesthetic practice.11 12
Many professional organisations have published similar guides on the delivery of a greener healthcare service, including the World Federation of Societies of Anaesthesiologists (WFSA) and the Australian and New Zealand College of Anaesthetists.13 14 The WFSA consensus statement proposes seven broad principles of environmentally sustainable anaesthesia. These include the use of environmentally preferable medications and equipment, incorporating environmental sustainability principles within formal anaesthesia education, and anaesthetists leading such activities within their healthcare organisations. Most recently, the Association of Anaesthetists has published an action guide with recommendations specifically targeted at reducing pollution from inhalational anaesthetic agents.15 An anaesthetic impact calculator has also been developed and made available as a free smartphone application, which can help clinicians calculate and compare the carbon dioxide equivalents of different anaesthetic plans with varying flow rates.16
Collectively, these guidelines provide a useful reference in developing carbon-neutral anaesthetic practices. However, it is clear that there is no ‘one size fits all’ approach. Our QIP used multipronged strategies, starting from educational interventions and regular surveys to observe trends; to more radical suggestions to limit access to desflurane. We observed a degree of pushback and we understand that this is due to a sense of infringement on one’s clinical practice. In retrospect, we realised that adopting an inclusive approach earlier would have retained goodwill and allowed us to better achieve our objectives. For example, sharing our QIP results regularly in the departmental bulletins helped to promote a sense of collective responsibility. We were able to creatively suggest an alternative option when one intervention was met with resistance, to continue to push forward with our ‘Greening the Operating Theatre’ agenda. Our campaign inspired ‘buy in’ because we engaged in multiple initiatives concurrently and adapted our strategies according to responses from the involved members of the healthcare team. We adopted both top-down and bottom-up approaches to ensure that any change we achieved will be sustainable. We actively sought out ways to encourage the use of other greener anaesthetic techniques. The limitations of our project included a small survey sample size and we encountered costing changes during the period of our QIP. We interpreted the survey results with care and used them to monitor trends. We took costing changes into account when calculating cost savings generated.
Conclusion
Our project comes amidst the growing recognition that clinicians can do more to alleviate the burden of climate change. Sequential application of QI methods across three PDSA cycles allowed us to consistently reduce median monthly desflurane usage by more than 50%. This project has promoted our institution as one that pioneers the path in delivering sustainable and environmentally-friendly healthcare in Singapore, and we hope other local institutions will follow suit.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We are grateful to acknowledge the help and advice given to the team by Dr Eric Lee, Dr Danny Lim, Dr Will Loh, Dr Eugene Liu, Dr Agrawal Rohit Vijay, Dr Tom Pierce, Dr Nanthini Pillay, Dr Cheah Xiao Li, Dr Lui Yee Lin, Dr Kevin Tan, Ms Ng Jia Min and Dr Chinnadurai Amutha.
Footnotes
Twitter @peikee1985
Contributors PKP - guarantor. KSA, ZKL, BSWN, PKP—all authors contributed to: study conception, study design, implementation of quality improvement Plan-Do-Study-Act cycles, data collection and analysis, manuscript writing, manuscript revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.