Article Text

Abstract
There is a need to optimize SARS-CoV-2 vaccination rates amongst healthcare workers (HCWs) to protect staff and patients from healthcare-associated COVID-19 infection. During the COVID-19 pandemic, many organizations implemented vaccine mandates for HCWs. Whether or not a traditional quality improvement approach can achieve high-rates of COVID-19 vaccination is not known. Our organization undertook iterative changes that focused on the barriers to vaccine uptake. These barriers were identified through huddles, and addressed through extensive peer outreach, with a focus on access and issues related to equity, diversity and inclusion. The outreach interventions were informed by real-time data on COVID-19 vaccine uptake in our organization. The vaccine rate reached 92.3% by 6 December 2021 with minimal differences in vaccine uptake by professional role, clinical department, facility or whether the staff had a patient facing role. Improving vaccine uptake should be a quality improvement target in healthcare organizations and our experience shows that high vaccine rates are achievable through concerted efforts targeting specific barriers to vaccine confidence.
- COVID-19
- Attitudes
- Quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
There is a need to optimise SARS-CoV-2 vaccination rates to protect staff and patients from healthcare-associated COVID-19 infection.1–4 To maximise COVID-19 vaccine uptake, many organisations implemented vaccine mandates, where healthcare workers (HCWs) were required to be vaccinated or face disciplinary actions up to and including termination.5–7 In Italy, mandatory COVID-19 vaccination among HCWs achieved vaccination rates of 89%–97.5%. Some recognised downsides of a mandate are staff shortages due to termination and concern that a mandate might disproportionally affect HCWs based on sociodemographic characteristics.8 9
Whether or not a traditional quality improvement (QI) approach can achieve high-rates of COVID-19 vaccination is not known. Our organisation undertook iterative interventions, short of a full vaccine mandate, with the goal of maximising HCW vaccine uptake. Our organisation is a multifacility academic centre that includes an acute care hospital, long-term care facility, rehabilitation hospital and specialised orthopaedic hospital. Following initial access to COVID-19 vaccine supply 9 December 2020, we convened a QI team on 31 December 2020 that included leadership from quality and patient safety, occupational health and safety, infection prevention and control, as well as communications and stakeholder relations. Initial problem characterisation efforts included cross-referencing groups of HCWs who were immediately eligible for COVID-19 vaccination with their historic influenza vaccination rates to guide QI efforts. We also conducted semistructured interviews with staff conducting vaccine booking calls to understand reasons for declining vaccination. HCW denominators were kept up to date by occupational health and safety and vaccination based on proof of receipt. However, for study purposes, we used a fixed HCW denominator from the onset of the campaign to calculate vaccine uptake. Real-time vaccine uptake was used to focus on areas with lower rates. Research ethics board review was not required based on institutional criteria for projects focused on improvement in quality of care.
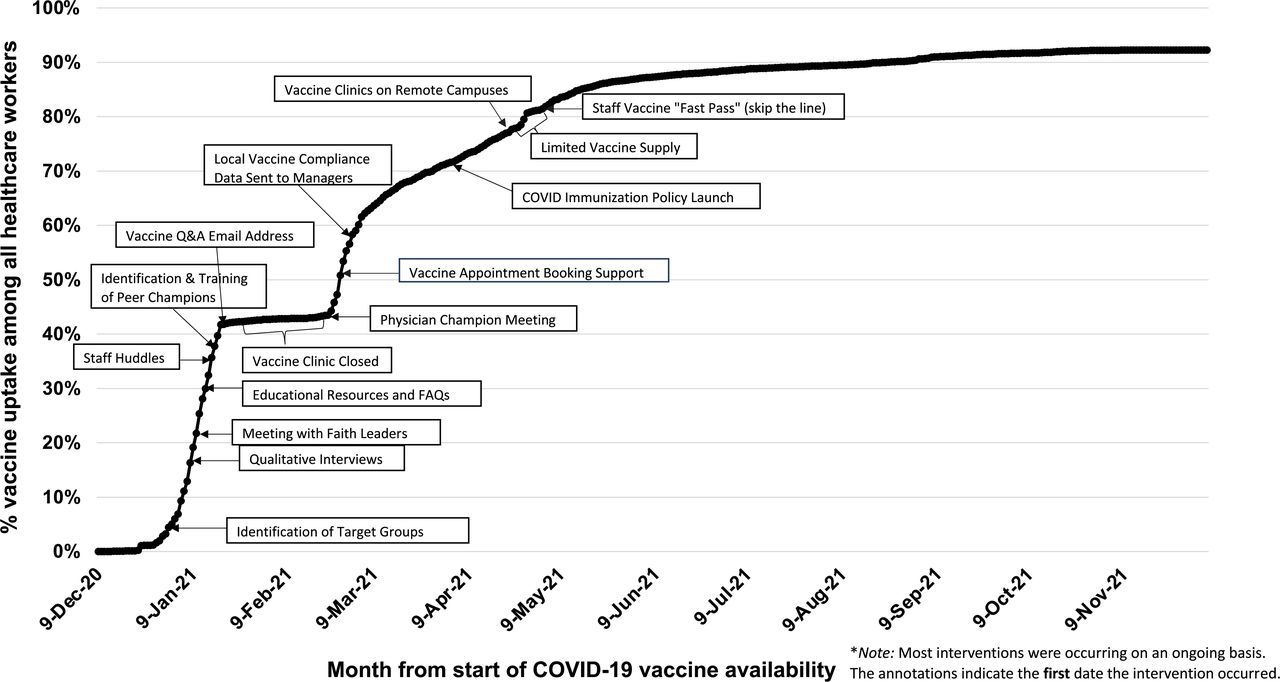
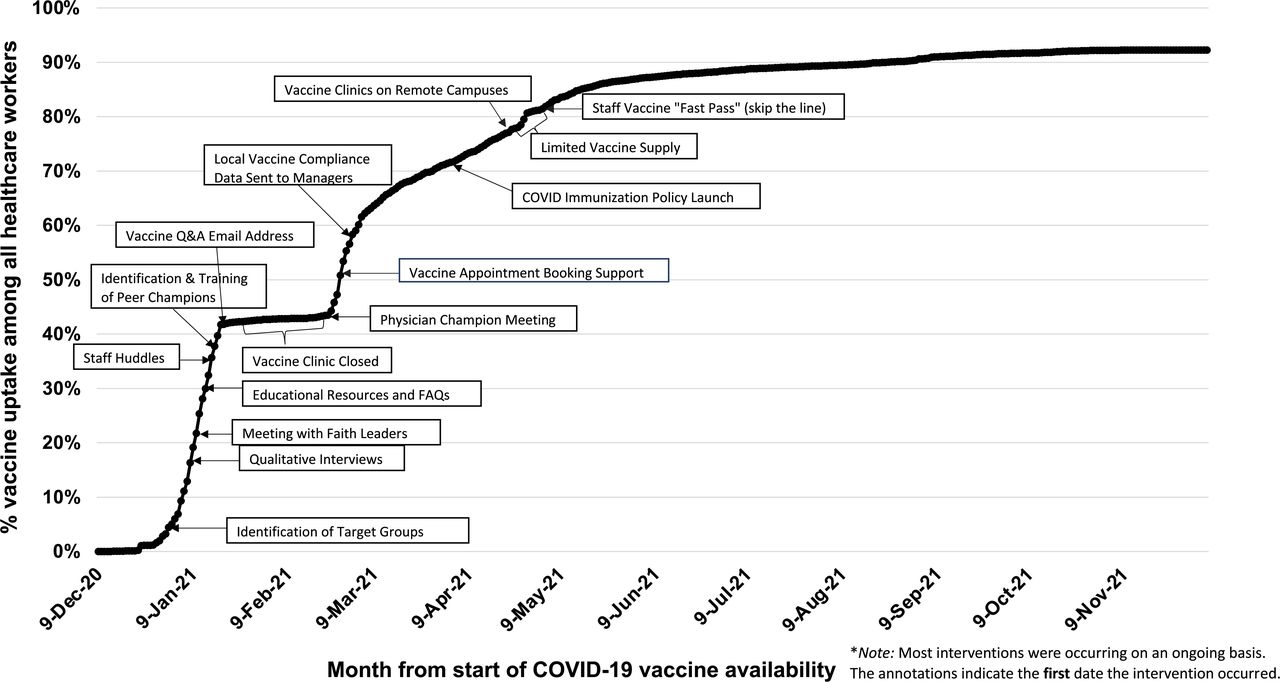
Table 1 summarises QI interventions used to overcome barriers to COVID-19 vaccination uptake. These included education and local peer outreach, development of a peer champion programme, local staff huddles, a staff-only email address for individual concerns and iteratively updated education resources. Examples included addressing perceptions of risk for staff of childbearing age, specific concerns of racialized staff and staff with a history of a vaccine complication. To address issues related to equity, diversity and inclusion, our team liaised with faith leaders, ensured diverse representation in our peer champions, had multilanguage education materials available and facilitated a ‘COVID conversation’ for black staff led by the hospital’s Anti-Racism Task Force. Access to vaccination was improved by helping staff navigate online appointment systems, creating dedicated vaccination clinics at remote campuses and a ‘fast pass’ to receive vaccination without an appointment and minimal wait times. Following the initial QI interventions, on 4 April 2021 we implemented a COVID-19 immunisation policy, where staff were required to complete one of three options: receive the COVID-19 vaccination, provide approved medical exemption or complete an online learning module.10
Summary of quality improvement (QI) interventions used to overcome barriers to COVID-19 vaccination uptake
Figure 1 depicts the change in vaccine uptake over time, indicating when the various interventions were implemented. There was no vaccine supply between 30 January and 15 February 2021 and limited supply 24 April–2 May 2021. The vaccine rate reached 92.3% (9436/10225) by 6 December 2021. Vaccine uptake by professional role, clinical department, patient interaction (ie, patient facing or not patient facing) and facility (ie, acute care, long-term care and rehabilitation) achieved minimum vaccination rates of 91% and maximum of 95%. For the same time period, the vaccine rate in the province of Ontario for individuals age 18–69 years was 89%.11 Overall compliance to the immunisation policy was 95.3%, including 92.3% choosing vaccination, 3.0% completing the module and declining vaccination and 0 demonstrating verified medical exemption. Among the non-compliant staff, only 130 (1.3%) were full-time staff.
{kind=link}
Depicts the change.
A strength of our study is that these interventions were developed based on identifying and addressing underlying barriers to vaccine confidence, as identified by staff, rather than relying on education alone. Many of the barriers to vaccine confidence that we addressed have been identified in prior qualitative studies regarding the COVID-19 vaccine.9 12 13
A significant limitation of our study is the potential for confounding due to the observational design and lack of a control group. In particular, public health measures beyond institutional policies may have influenced vaccine uptake significantly, including the introduction of vaccine passports in some public spaces in September 2021. However, vaccine rates already reached 90% across our organisation by the time this measure was introduced. In addition, our reported vaccine rate is likely an underestimate because we used a fixed denominator that included part-time staff and staff that left the organisation during our study period. The intensity of our vaccine campaign is also a limitation since it required significant resources and would be difficult to replicate across all healthcare institutions.
Our experience shows that seeking out specific barriers, promoting peer-to-peer discussions and providing individual counselling may be more effective than traditional educational vaccine campaigns. Whether or not this QI approach can be effective in sustaining high rates of COVID-19 periodic booster doses requires further long-term evaluation.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank Hazel Baillie for her contributions to this paper.
Footnotes
Contributors All authors were involved in performing the work described in the manuscript. AW and JL drafted the manuscript. All authors were involved in discussing the results and commenting on the manuscript. AC, VW and NT had a primary role in data collection and analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JAL has received payment for expert testimony requested by hospitals of the Ontario Hospital Association, Seneca College, and Ministry of the Attorney General of Ontario. No other competing interests declared.
Provenance and peer review Not commissioned; externally peer reviewed.