Article Text

Abstract
Background Even though the immediate postpartum period is a golden time and a great opportunity to provide long-acting reversible contraceptives to prevent unintended pregnancy, its utilisation is very low in Ethiopia. Quality of care in postpartum long-acting reversible contraceptive provision is thought to be an issue for this low utilisation. Thus, continuous quality improvement intervention is necessary to increase the use of postpartum long-acting reversible contraceptives at Jimma University Medical Center.
Method A quality improvement intervention to offer long-acting reversible contraceptive methods to immediate postpartum women at Jimma University Medical Center was initiated in June 2019. To study the baseline prevalence of long-acting reversible contraceptive use at Jimma Medical Centre over 8 weeks, we reviewed postpartum family planning registration logbooks and patients’ charts. Based on the baseline data, the quality gaps were identified, prioritised and change ideas were generated and tested over another 8 weeks towards achieving the immediate postpartum long-acting reversible contraceptive prevalence target set.
Result This new intervention resulted in an average increase in immediate postpartum long-acting reversible contraceptive methods use from 6.9% to 25.4% by the end of the project intervention. The major barriers to low long-acting reversible contraceptive use were lack of attention from hospital administrative staff and quality improvement teams on the provision of long-acting reversible contraceptives, lack of training of healthcare providers on postpartum contraception and unavailability of contraception commodities at each postpartum service delivery points.
Conclusion and recommendations The immediate postpartum long-acting reversible contraceptive use at Jimma Medical Centre was increased by training of healthcare providers, availing contraception commodities through administrative staff involvement, weekly audit and feedback on contraception use. Thus, training of the newly hired healthcare providers on postpartum contraception, involvement of hospital administrative staff, regular audits and feedback on contraception use is necessary to increase postpartum long-acting reversible contraception uptake.
- Continuous quality improvement
- Health services research
- Women's health
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Making the long acting reversible contraceptives (LARCs) commodities accessible 24/7, training healthcare providers and monitoring increased the postpartum LARCs.
WHAT THIS STUDY ADDS
Change ideas used in this study can be tested on a large scale in other health facilities for possible scale-up.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Establishing a continuous quality improvement (CQI) team helps to identify bottlenecks in providing LARCs.
Generating change ideas for the bottlenecks through CQI principles can result in increasing LARC uptake.
Introduction
Based on the mini 2019 Ethiopian Demographic and Health Survey analysis, the use of modern family planning is low. Overall, 41% of currently married women are using a modern method of family planning, and 1% are using a traditional method. Among the currently married women, the most commonly used methods are injectables (27%), implants (9%), intrauterine devices (IUD) (2%) and pills (2%).1 When we come to immediate postpartum family planning (IPPFP), it is even worse and out of a quarter of postpartum women who were counselled on contraception, only 13.6% received the contraceptive methods.2 As a result, the immediate postpartum long-acting reversible contraceptives (LARCs) use in sub-Sharan Africa (SSA) varies from 2% to 14%3 in general, and its use in Ethiopia varies from 11% to 17%4 5 in particular.
The unintended pregnancy rate remains higher, ranging from 64 to 91 pregnancies per 1000 women in developing regions compared with 35 pregnancies per 1000 women in developed regions.6 Waiting at least 24 months before attempting the next pregnancy was recommended as it is found to be a healthy time for pregnancy and as a result reduce the risk of adverse maternal, perinatal and infant outcomes.7 8 To decrease these risks, access to immediate LARCs is essential.8 9 LARCs are the ideal contraceptive methods for the prevention of the harmful consequences of unintended pregnancies in most women and adolescents as they are safe, effective and reversible.10 11 About 190 million women of reproductive age worldwide who want to avoid pregnancy do not use any contraceptive method and the unmet need for family planning in SSA is one of the highest, ranging from 20% to 26%.12 LARCs, which consist of implants and IUD, are the most effective modern family planning methods in tier one in addition to vasectomy and tubal ligation.13 14 Almost all postpartum women are medically eligible for LARCs.15 These methods have multiple advantages over other reversible methods as they do not require maintenance and their duration of action is long, ranging from 3 to 10 years once in place.16
The prevalence of LARCs use in SSA is one of the lowest, at 13.86% (11.18% for implant and 2.68% for IUDs).17 According to a United Nations study of 2015, worldwide, 57% of married women are using a modern form of contraceptives; and a recent study of 2019 showed, that only 15.5% of women worldwide use IUDs, and only 3.4% use subdermal implants. The common reasons for low uptake include misperceptions about the safety and efficacy of LARCs, perceived lack of consumer demand, inadequately trained providers and the relative complexity of providing LARCs compared with short-acting methods.18
Rapid population growth remains a major concern in many SSA countries.19 Women rely primarily on traditional and short-acting contraception, which is prone to incorrect or inconsistent use and failure.9 19 20 This leads to high maternal morbidity and mortality attributed to unintended pregnancies, short birth intervals and a higher risk of obstetric complications.21
A study in East Africa, in 2012, shows that access to FP services is particularly low among rural, less educated and poorer women. Furthermore, availability, perceived costs, lack of provider skills and misperceptions about modern contraceptives and their risks and benefits are barriers to uptake.22
A study done in Kenya in 2014, noted that only 3.4% and 9.9% of women seeking family planning methods use IUCD and implants, respectively. In Kakamega County, particularly, the report indicated that only 1% of the women use IUCD. This is very low given the advantages associated with LARC. Different reasons have emerged as to why the uptake is low but with no data to back up the statement.23
It is believed that health coverage and access to care have increased over the past decades, however, due to the poor quality of care, different sexual and reproductive healthcare targets could not be achieved, and as a result, associated morbidity and mortality could not be reduced. Even though LARCs commodities are free of charge and available in our hospital, it is only located at the family planning clinic in the outpatient department. As a result, the family planning commodities are not accessible to immediate postpartum women. Furthermore, there is a high turnover and lack of motivation among trained healthcare providers on family planning to provide immediate postpartum LARCs.
This study aimed to assess all fundamental barriers to immediate postpartum LARCs use and determine the effect of continuous quality improvement (CQI) using a plan–do–study–act (PDSA) based quality improvement model to increase the use of postpartum LARCs at Jimma University Medical Center (JUMC).
We presented here the changes made to increase the observed low utilisation of immediate postpartum LARCs use with the aim to increase from the baseline (6.9%) to CQI using the PDSA cycle to 30%.
Methods
Study area
A CQI on immediate postpartum LARCs use was conducted in the department of obstetrics and gynaecology, maternity and labour ward of JUMC, which is located 354 km the Southwest of Addis Ababa. JUMC is one of the oldest teaching hospitals in Ethiopia with an 800-bed capacity and a catchment population of over 15 million people.
Study design
CQI strategy using the PDSA cycle was conducted in two phases.
Baseline
The past 2 months’ baseline data were collected from 1 March 2019 to 30 April 2019, to determine the baseline immediate postpartum LARCs’ prevalence and exit interviews were conducted on 100 postpartum mothers, 10 midwives and 10 residents to identify the quality gaps. We identified an immediate postpartum LARCs use baseline average of 6.9% among the deliveries from 1 March 2019 to 30 April 2019, before the intervention.
Intervention
First, based on the analysis of the baseline data, we observed that the LARCs’ services at JUMC were not accessible to immediate postpartum women and as a result, postpartum LARCs use is very low. This observation led the gynaecology and obstetrics department to address these quality gaps through the establishment of a quality improvement team composed of a Gyn/Obs department head, Gyn/Obs resident, midwife and maternity service coordinator under the hospital’s quality improvement committee.
Second, the quality improvement team has prioritised the problems identified from baseline using a prioritisation matrix24–26 (table 1), generated change ideas and implemented the change ideas to see the progress of immediate postpartum LARCs’ uptake using monitoring, auditing and feedback tools over the next 8 weeks (1 June 2019 to 31 July 2019) (figure 1).
Prioritisation matrix
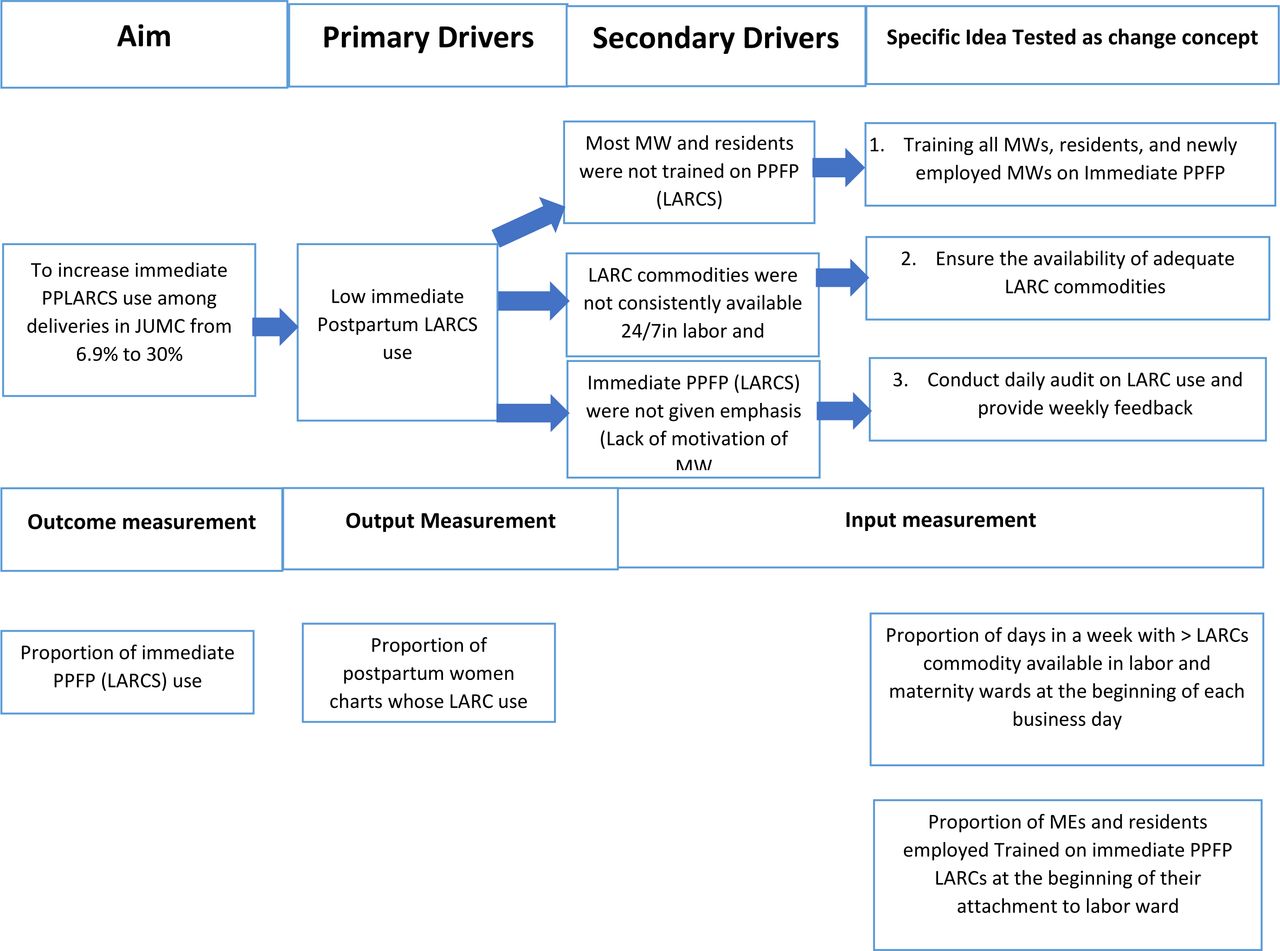
Drivers diagram on postpartum LARCs use in JMC. JMC, Jimma Medical Centre; JUMC, Jimma University Medical Center; LARCs, long-acting reversible contraceptives; PPFP, postpartum family planning; PPLARCs, postpartum LARCs.
Third, training of healthcare professionals (midwives and residents) on total quality of care concepts and family planning with a special focus on post partum, and availing LARCs at each service delivery point 24/7 was done. Data collection tools were developed and included in the maternal cards and midwives and residents were motivated to collect these data sources daily for weekly audits and feedback as well as monthly reports. The staff was encouraged to be motivated by skills they acquired during the training and intervention, providing an improved quality continuum of care and observing the improved outcomes of the CQI.
Numerator
Number of postpartum women who had received counselling and accepted a long-acting reversible contraception method.
Denominator
A total number of admitted postpartum women during the intervention period who are a candidate/eligible for LARCs use.
Intervention
Continuous QI using PDSA model.
Strategy
We conducted two PDSA cycles to evaluate the implementation and incorporate feedback during this CQI.
PDSA cycles 1
The first PDSA cycle, 1 May 2019 to 31 May 2019, focused on training the staff (residents and midwives) on the LARCs method with special emphasis on counselling, availing LARCs commodities, protocols and data collection tools, and motivating, midwives and residents to satisfy the clients’ need regarding their chosen family planning method.
LARCs and total quality of care training
Training on overall family planning with a special focus on postpartum contraception and total quality of care principles was organised and given by obstetricians and gynaecologists, and midwives who had training of trainers (TOT) from the national federal ministry of health and WHO on three rounds. The trainers were providing similar training for the ministry of health and other international non-governmental organisations. It was given using the national family planning and quality of care guidelines. Didactic training was carried out on client assessment, medical eligibility, counselling, family planning method—IUD and Implant, postinsertion care, management of side effects and complications from postpartum IUCD, infection prevention and total quality of care. The training was 3 days of theoretical and 5 days of onsite demonstration with competency assessment using the national checklist.
Out of 45 midwives working in labour and maternity wards, only 2 of them had training on LARCs previously. The training was given to 39 midwives and, 51 residents in obstetrics and gynaecology. Finally, both the midwives and the residents completed the training with a minimum competency score of 75%.
PDSA cycle 2
This PDSA cycle focused on the implementation and monitoring of the implemented change ideas to increase the postpartum LARCs counselling and uptake from 1 June 2019 to 31 July 2019. All postpartum clients were counselled on postpartum contraceptives by the trained midwives and residents based on informed consent, voluntary decision-making and all family planning options. Clients who agreed based on counselling were offered the Immediate postpartum LARCs of their choice and supportive supervision was provided to motivate the LARCs’ provision. Checklists were prepared for daily monitoring of implemented change ideas (availability of LARCs commodities, trained professional on-site), for weekly audit and feedback for 8 weeks. Data on immediate postpartum LARCs counselling and provision were collected daily from clients’ charts and client interviews at discharge. Completeness of the data was checked regularly, and the result was analysed for weekly audit and feedback. Newly faced quality gaps during the implementation of change ideas were discussed and addressed during weekly audits and feedback.
Postintervention sustainability of immediate postpartum LARCs use
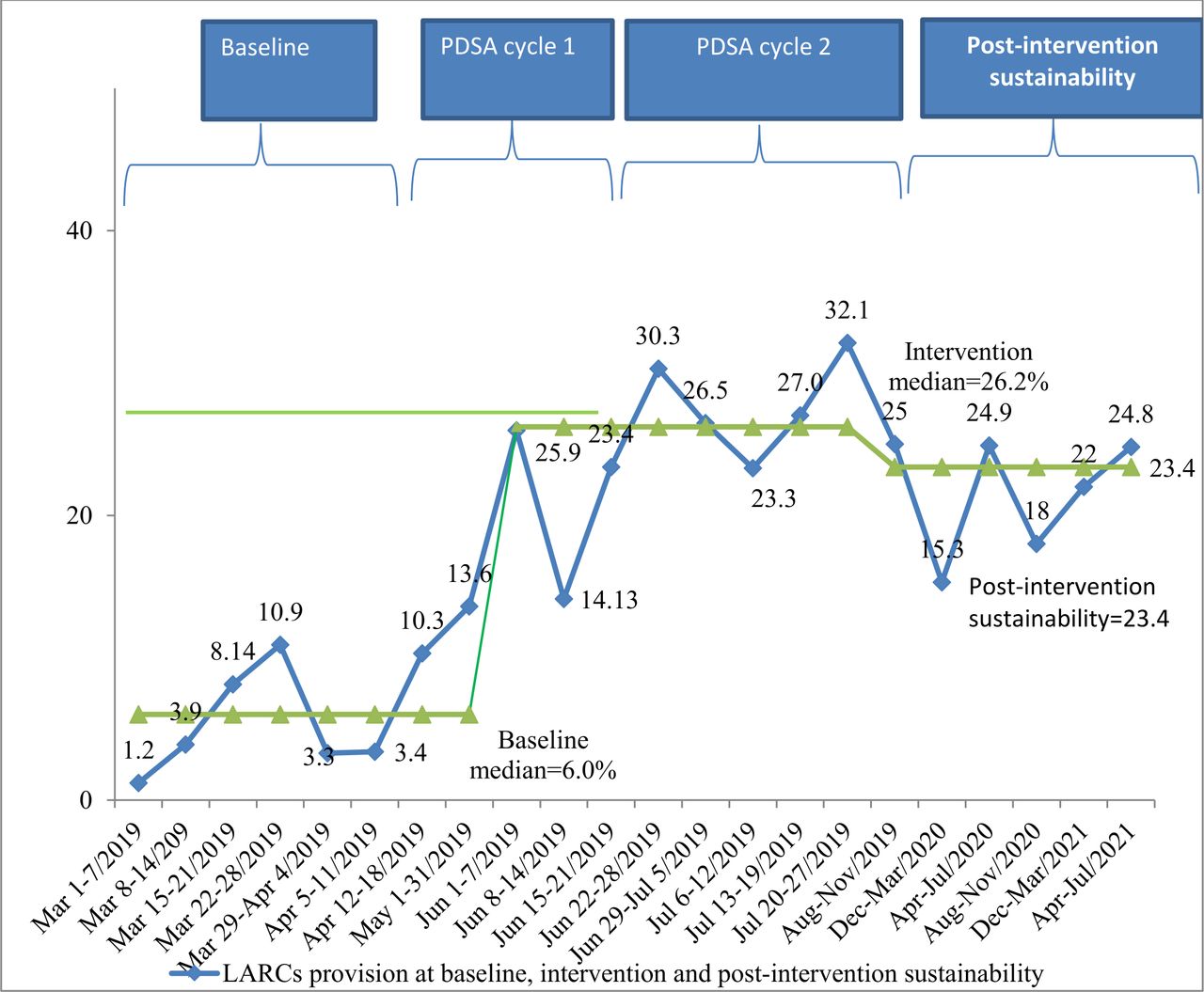
We have analysed the 2 years trends of LARCs uptake after intervention from 1 August 2019 to 31 July 2021, to see the sustainability of the LARCs uptake after the intervention period. For this analysis, we have used the data from the immediate postpartum logbooks, IPPFP monthly report (figure 2).
{kind=link}
{kind=link}
An average of 6.9% at baseline, 25.37% postintervention and 23.4% postintervention sustainability of postpartum women choose LARCS at JUMC 2019. JUMC, Jimma University Medical Center; LARCs, long-acting reversible contraceptives; PDSA, plan–do–study–act.
Data processing and analysis
The consistency and completeness of data was checked by the principal investigator and code was given to the necessary parts of information. Data were edited and entered into EpiData V.3.1 and then exported to SPSS V.20 for cleaning and analysis. Tables, run charts and figures were used to depict the findings. To conclude the shift in baseline (change), we considered six or more consecutive points above the baseline median. We have used the Standards for QUality Improvement Reporting Excellence (SQUIRE) guideline 2.0 to prepare the manuscript.27
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
Baseline
Out of 798 deliveries seen over 8 weeks before the baseline survey, 789 mothers were candidates for counselling and offering of LARCs excluding those for whom Bilateral tubal ligation and total abdominal hysterectomy were done. Of these, only 55 (6.9%) postpartum mothers were provided with LARCs, out of which implant was provided for 45 (5.6) and IUD was for 10 (1.3%) mothers (figure 2).
A total of 100 immediate postpartum mothers who gave birth at JUMC were randomly selected for exit interviews (table 2). From our study, 68 (68%) of the current pregnancies were unplanned, 59 (59%) mothers were para 2–4 and 71 (71%) have 3 and above alive babies. Nearly 95% of mothers who plan to have their next baby has plan to postpone their pregnancy beyond 2 and more years. Eighty-seven per cent of mothers were ever heard about LARCs methods, and 50 (57.5%) were counselled about LARC during ANC visits. Of the current participants, 35 (40.2%) were provided with Implants and only 2 mothers were provided with IUD.
Reproductive information, knowledge and utilisation of immediate postpartum mothers at JUMC (March and April 2019)
Among the reasons why the immediate postpartum women did not use LARCs were, fear of side effects in 17 (26.9%), husband disapproval in 13 (20.6%) and taking after 6 weeks of delivery in 11 (17.5%). The other reasons were no trained healthcare providers and no commodities available at the labour and maternity service delivery units (table 2).
In addition to a mother exit interview, we also interviewed healthcare providers to know the challenges they face while offering contraceptives to postpartum mothers. Only 2 out of 45 midwives and none of the 51 residents working at the labour and maternity ward of JUMC were trained on contraception or LARCs. A total of 20 randomly selected midwives and residents were interviewed considering the saturation of information in our qualitative study. From this, 9 (45%) of health providers involved in an interview has no training and 7 (35%) of them did not provide LARCs due to the unavailability of the commodities at the needed time in labour and maternity wards.
Interventions
PDSA 1
A total of 39 midwives and 51 obstetrics and gynaecology residents were trained on LARCs and total quality of care principles using national guidelines. The quality improvement team communicated to the responsible bodies in the hospital (head midwives, pharmacy heads and hospital managers) to avail LARCs (IUD and implants) at labour and maternity wards in lockers prepared for this purpose as a result. The trained health professionals were motivated by the quality team to counsel, provide LARCs and ensure the availability of postpartum contraception or LARCs commodities.
PDSA 2
Daily monitoring of the presence of LARCs commodities at the respective place was made and every 2 weeks 84 Implants and 56 IUDs were being brought from the pharmacy store. Then counselling and provision of the LARCs to immediate postpartum mothers at both the labour and maternity ward started from the fourth day of the second-round training, the day the onsite demonstration was started. Monitoring of the daily activities using the prepared checklists was started the same day with counselling and offering of LARCs. Audit and feedback with the healthcare providers and the quality team were done every week. During these times, the overall weekly activities were summarised with their identified challenges. Then the discussion was done on those challenges and solutions were proposed to address the challenges. Accordingly, in the first 2 weeks of intervention, the main reasons most women refused to take LARCs were due to fear of side effects and husband disapproval. Subsequently, we addressed the fear of side effects with effective counselling and involvement of their husbands during the counselling whenever they needed them for decisions.
The total number of postpartum women counselled for LARCs was highly dependent on the total number of deliveries that occurred each week and the run chart changes with each number of mothers who gave birth at JUMC.
The overall 8 weeks intervention of LARCs provision is presented by the run charts and the new challenges being identified and some measures taken each week were also pointed out in the boxes on the graph during each weekly audit and feedback. There was one mother who expelled the IUD after 45 min of insertion as she developed a postpartum haemorrhage. Then she was counselled and provided with an implant at discharge.
During the project, there was no problem with the availability of the commodities as per the daily need (stock out), and it was being checked daily and was brought from the store pharmacy every 2 weeks and kept in the locker prepared for it.
There were 832 deliveries conducted at JUMC during this intervention period; out of which 820 (98.6%) women were candidates for counselling and provision of LARCs. A total of 480 (58.54%) were counselled on LARCs, out of whom 208 (25.37%) were provided with LARCs. The average percentage from base line to intervention were went from 6.9% to 25.37% of mothers discharged with immediate postpartum LARCs.
From the total LARCs provided, IUD accounts for 95 (11.59%), which increased by 8.92% times from the baseline (1.3%), and implants accounted for 113 (13.78%) from the baseline (5.3%) which increased by 2.6% times. Compared with the baseline prevalence of LARCs use, monitoring and auditing significantly increased the use of LARCs during the intervention period; the shifts of all the eight consecutive points of the run charts are above the median of the baseline LARCs use and all run series points are above the baseline median showing significant LARCs use improvement during the intervention periods (figure 2).
After intervention, we try to see 2-year data from logbook and sustainability data show an average 23.4% of women discharged home with LARCS (figure 1).
Barriers to LARCs use for immediate postpartum mothers
The provision of LARCs during the intervention period increased from the baseline gradually with ongoing auditing and feedback, and monitoring of the introduced change ideas. During this intervention period, 105 (12.8%) postpartum mothers preferred to take LARCs after 6, and of these mothers were appointed to family planning clinics, 79 (6.9%) women preferred to take it at the nearby health centre.
Discussion
The study showed that the baseline prevalence of LARCs use at JUMC over 8 weeks before intervention was only 6.9%. Of these, implant accounts for 5.6% and IUD accounts for 1.3%.
Our finding is similar with the recent study from Ethiopia about the proportions of LARCs methods use but low with regard to the immediate postpartum LARCs use, which is 21.3%.28 Low utilisation of LARCs is also reported by the United Nations which showed, that only 15.5% of women worldwide use IUDs, and only 3.4% use subdermal implants. The common reasons for low uptake include misperceptions about the safety and efficacy of LARCs, perceived lack of consumer demand, inadequately trained providers and the relative complexity of providing LARCs compared with short-acting methods.29 Our study finding was also comparable with a study done in one of the Kenyan Hospitals, which showed a low prevalence of LARCs due to the barriers like; lack of staff skills in counselling and provision of LARCs, poor community awareness of LARCs and lack of family planning commodities in the maternity ward.23
This study shows that 68% of the current pregnancies were unplanned, and nearly 95% of mothers who plan to have their next baby has the plan to postpone their pregnancy beyond 2 and more years. Though the unplanned pregnancy rate is higher in our baseline study compared with a previous study in Ethiopia (68% vs 27.2%), the plan to postpone pregnancy beyond 2 years is more or less similar (95% vs 84%).28
According to this study the reasons why the immediate postpartum women did not use LARCs were fear of side effects in 26.9%, husband disapproval in 20.6% and taking after 6 weeks of delivery in 17.5% which is also similar to the previous study in Ethiopia.28
Intervening in those identified gaps, through CQI; training the healthcare providers about the facts and benefits of LARCs to improve their skills in both counselling’s and providing the method, availing IUD and Implants at the points of care, mobilising the hospital quality improvement teams and weekly audit and feedback, our intervention gradually increased the percentage of women using immediate postpartum LARCs at JUMC from 6.9% to 25.37% over 8 weeks. This has an important role in reducing the high maternal mortality rate in the country by preventing unplanned pregnancies, which is one of the big challenges of the hospital.
Our finding is similar to a quality improvement strategy to offer LARCs methods to immediate postpartum women at a university hospital in rural Haiti in 2016. This new strategy produced an average improvement of Immediate postpartum LARCs from 5% to 32% of women delivering at the hospital, accepting a long-acting method (including bilateral tubal ligations) by the end of the project and which has proved sustainable at an average of 20% to date.30
The study done in Kenya Nairobi in 2018, over 16 weeks, showed that the percentage of women using LARCs increased from 17% noted in the baseline study to 83%. The improvement is likely to have been due to the implementation of the options that were derived from the decision matrix. These included changing the process flow to enable integration of services, health education to both health workers and the community and applying the 5 s to improve the arrangement of the environment which enabled the health workers to document their work easily and also facilitated easy client flow and finally the training of the health workers to improve on their skills in both counselling and providing the method.23 Even though the intervention process had a similarity, the achievement of the study in Kenya was much greater than our study result; the reason for this might be the difference in the commitment of healthcare providers to counselling and provision of LARCs, the sociodemographic characteristics of postpartum mothers and the duration of intervention.
Even though it did not clearly state the baseline prevalence of LARCs use, the study done in five crisis-affected countries; Chad the Democratic Republic of the Congo, Djibouti, Mali, and Pakistan showed that the use of LARCs increased to 61% over 2.5 years by (1) competency-based training, (2) supply chain management, (3) systematic supervision and (4) community mobilisation to raise awareness and shift norms related to family planning.31 This study has similarities with our study in terms of interventions made to increase LARCs use.
Limitations and strengths of the study
The strengths of the study are that those commodities were availed at each service delivery point throughout the intervention period. The study showed how much could be achieved with minimal manipulation of the process through CQI intervention. In addition, the obstetrician and gynaecologists, midwives who had TOT were involved to train the health providers, and the hospital managers were involved in the quality improvement which is essential for the scale-up and sustainability of the project.
The limitations are that training provided to healthcare providers did not include all staff working at the labour and maternity unit. The satisfaction and discontinuation rate of LARCs were not followed and assessed for those mothers who took this contraceptive.
Conclusion
The project interventions have proven sustainable over time as evident in our results. Overall, through CQI intervention, the uptake of LARCs use was increased from 6.9% at the baseline to 25.37% over another 8 weeks of the intervention period. JUMC should, therefore, sustain and continue using this CQI as a learning CQI project over a long period to see its effect in increasing immediate postpartum LARCs uptake. In addition, the change ideas used in this study should be tested over a long period in multiple facilities to see the outcome for further scale-up to other health institutions.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Jimma University Institutional review Board. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The staff of gynaecology and obstetrics deserves acknowledgment.
Footnotes
Contributors DAS made substantial contributions to conception and design, data management and quality, or analysis and interpretation of data. ZA contributes to the conception and design, and preparation of the manuscript. DAS, LSD, GTD and ZA were involved in the analysis and interpretation of data and revising the manuscript critically for important intellectual content. ZA is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.