Article Text

Abstract
Aims Variable rate intravenous insulin infusion (VRIII) is used perioperatively to maintain normoglycaemia in patients with diabetes who are undergoing surgery. The aims of this project were as follows: (1) to audit the extent to which perioperative prescribing of VRIII for diabetic vascular surgery inpatients at our hospital meets established standards and (2) to use the results of the audit to guide improvement in the quality and safety of prescribing practices and reduce VRIII overuse.
Methods Vascular surgery inpatients who had perioperative VRIII were included in the audit. Baseline data were collected consecutively from September to November 2021. There were three main interventions: a VRIII Prescribing Checklist, education of junior doctors and ward staff, and electronic prescribing system updates. Postintervention and reaudit data were collected consecutively from March to June 2022.
Results The number of VRIII prescriptions totalled 27 in preintervention, 18 in postintervention and 26 in reaudit periods. Prescribers used the ‘refer to paper chart’ safety check more frequently postintervention (67%) and on reaudit (77%) compared with preintervention (33%) (p=0.046). Rescue medication was prescribed in 50% of postintervention and 65% of reaudit cases compared with 0% preintervention (p<0.001). Intermediate/long-acting insulin was appropriately amended more often in the postintervention versus preintervention period (75% vs 45%, p=0.041). Overall, VRIII was appropriate for the situation in 85% of cases.
Conclusions The quality of perioperative VRIII prescribing practices improved following the proposed interventions, with prescribers more frequently using recommended safety measures such as ‘refer to paper chart’ and rescue medication. There was a marked sustained improvement in prescriber-initiated adjustment of oral diabetes medications and insulins. VRIII is occasionally administered unnecessarily in a subset of patients with type 2 diabetes and may be an area for further study.
- Surgery
- DIABETES MELLITUS
- Quality improvement
- Checklists
- Patient safety
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is significant complexity surrounding diabetes management perioperatively and this is associated with frequent medication errors involving insulin—a high-risk drug carrying potentially serious consequences if inappropriately used.
WHAT THIS STUDY ADDS
This project demonstrated improvements in the quality and safety of perioperative prescribing for patients with diabetes through interventions involving education, technology and a ward-based checklist. Initially deployed on a single ward, there has been great interest locally in adopting these tools to support prescribers in other departments. There is also scope for wider-reaching effects in other hospitals.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This report adds to our understanding of the challenges inherent in variable rate intravenous insulin infusion prescribing and describes a possible means to effect positive change.
Introduction
Variable rate intravenous insulin infusion (VRIII) is used perioperatively to maintain normoglycaemia in patients with diabetes who are undergoing surgery. The importance of achieving a normoglycaemic state in this population is emphasised by a substantial body of evidence linking dysglycaemia to increased rates of morbidity and mortality following surgery.1–5 In recognition of the clear benefits of maintaining good glycaemic control in hospital inpatients, numerous guidelines and consensus statements have been published, however, the issue is vast and intricate. Not all patients with diabetes require insulin infusion perioperatively; multiple factors including diabetes type, duration of starvation period, HbA1c, capillary blood glucose and urgency of the operative intervention must be taken into account for each patient to determine whether VRIII is indicated.6 Moreover, patients’ regular oral diabetes medications and insulin must be withheld or amended appropriately while on VRIII and until eating and drinking normally. There is significant complexity surrounding diabetes management perioperatively but it is important that patients are only on an insulin infusion when necessary and that essential medication changes are made to optimise diabetic control and thus avoid unnecessary patient harm.
Errors with insulin are both high risk and exceedingly common. Insulin has been identified as a ‘high-alert medication’ by the Institute for Safe Medication Practices.7 Indeed, insulin is one of a small number of specific medicines that account for the majority of fatal and serious outcomes when misused.7 It has a narrow therapeutic range such that administration of too much or too little insulin can cause hypoglycaemia or hyperglycaemia, respectively—both of which have the potential to lead to coma and death.8 9 Given the explicitly reported dangers of insulin misuse, the frequency of such errors is unacceptably high. The National Diabetes Inpatient Audit (NDIA) revealed that 30% of inpatient drug charts surveyed contained at least one medication error and 18% had at least one insulin error.10 A multitude of factors are known to contribute to the prevalence of insulin errors, and these include variety (eg, of strengths; formulations; delivery devices) and the individualisation of regimens to achieve optimal diabetes control in each patient.11 Where even routine inpatient diabetes management can be complex and vulnerable to medication error, it follows that perioperative VRIII could be high risk for errors as the process requires that accurate and timely changes be made to regular insulin and oral diabetes medicines. Although there is evidence to suggest that VRIII is sometimes used unnecessarily in patients with diabetes,12 there is a paucity of data describing adherence to VRIII prescribing guidelines.
Members of the multidisciplinary team on our vascular surgery ward raised concerns that VRIII was being overprescribed and that the necessary adjustments to regular insulin and oral diabetes medications when commencing VRIII were not always meeting established standards. Therefore, a project was designed with the following aims: (1) to audit the extent to which perioperative prescribing of VRIII for diabetic vascular surgery inpatients at our hospital meets the standards set by the Joint British Diabetes Societies for Inpatient Care Group (JBDS-IP) and (2) to use the results of the audit to guide improvement in the quality and safety of prescribing practices and reduce VRIII overuse for vascular surgery patients with diabetes.
Methods
Context
This quality improvement project was carried out in a 27-bed vascular surgery ward within a large teaching hospital and one of the largest vascular units in the UK. In this hospital, all routine prescriptions including patients’ usual insulin and oral diabetes medications are populated on eMeds (an electronic medication management system). However, some complex intravenous infusions such as perioperative VRIII are prescribed on paper charts. It is local protocol that paper prescription charts are referenced on eMeds using a ‘dummy drug’, which serves as a prompt for eMeds users to review the corresponding paper chart.
Data collection
Inpatients on the vascular surgery ward who had perioperative VRIII prescribed during their admission were included in the audit. Baseline data were collected consecutively from September to November 2021. Data were obtained from PPM+ ("Patient Pathway Manager" electronic health record), eMeds and VRIII paper prescription charts into a template that was developed based on the project objectives. The main objectives were:
1. Compare perioperative VRIII prescribing practices on the vascular surgery ward to the national guideline established by the JBDS-IP. Relevant data points collected were as follows:
Was the VRIII paper chart prescription referenced on the patient’s electronic medicines chart (eMeds) using the ‘refer to paper chart’ dummy drug?
Were appropriate treatments for hypoglycaemia management pre-emptively prescribed on the eMeds chart when VRIII was commenced?
Were all regular diabetes treatments (insulin and tablets) amended or withheld appropriately when commencing VRIII and while the patient was on VRIII?
2. Evaluate whether vascular surgery patients with diabetes, who received VRIII perioperatively, met the criteria for commencing VRIII. Relevant data points collected were as follows:
Diabetes type (type 1 vs type 2 diabetes).
Number of missed meals.
Glycated haemoglobin test, HbA1c, within 3 months preoperative.
Capillary blood glucose before commencing VRIII.
Emergency surgery (defined as having been performed within 24 hours of admission).
The project team members agreed that data collection would stop after approximately 25 VRIII prescriptions as this number was evaluated to provide a reliable snapshot of current prescribing practices on the ward.
Interventions
There were three main interventions: a VRIII Prescribing Checklist (online supplemental appendix 1), education of junior doctors and ward staff, and eMeds system updates. The Prescribing Checklist contains a list of the indications for perioperative VRIII and a step-by-step guide through the prescribing tasks that must be completed to safely commence VRIII. This was developed in a collaborative approach by doctors and pharmacists based on local National Health Service Trust and JBDS-IP guidelines.6 It was created to function as a concise summary of the lengthy JBDS manual and made pragmatically relevant for our local doctors. The overall goal was to reduce prescribing errors—both those due to missing key steps and those due to lack of logistical ‘know-how’. Laminated copies of the Prescribing Checklist were displayed prominently in the ward junior doctor’s office and on drug trolleys. The project was also presented at various local meetings including junior doctor induction, ward safety meeting and our departmental clinical governance meeting (in order to raise general awareness of the importance of adhering to perioperative VRIII guidelines and the Prescribing Checklist). The final area of intervention was an eMeds update. Changes included: (1) insertion of a reinforcing message about making appropriate changes to the patient’s insulin and other regular diabetes medicines when prescribing VRIII, (2) automating the addition of rescue medication on selection of the ‘refer to paper chart’ dummy drug and (3) rephrasing biphasic insulin descriptions to reduce confusion with other intermediate-acting insulins. The interventions were designed and implemented over a 3-month period from December 2021 to February 2022.
Supplemental material
Postintervention data
Postintervention data were collected consecutively from March to April 2022 using the same inclusion criteria, data sources and template as per our baseline data collection. The project team members agreed that postintervention data collection would stop when the junior doctors collectively rotated out of vascular surgery as this group had received targeted education about VRIII prescribing.
Reaudit
Reaudit data were collected consecutively from May to June 2022 to observe VRIII prescribing practices on the vascular surgery ward following rotation of a new cohort of junior doctors into the department, which occurs routinely every 4 months. The VRIII Prescribing Checklist and eMeds updates remained in place, however, the junior doctors did not receive targeted education. Rather, a short talk on VRIII prescribing was incorporated into the induction session for junior doctors newly rotated into vascular surgery as this was perceived by the audit team to be a more sustainable educational intervention in the long term. For clarity, a project timeline is included in online supplemental appendix 2.
Supplemental material
Analysis
Statistical analysis was performed in IBM SPSS Statistics (Version 27). Cochran’s Q test was performed to assess the proportion of VRIII prescribing steps successfully completed across preintervention, postintervention and reaudit study periods. P values of <0.05 were deemed statistically significant.
Patient and public involvement
As the project was centred on investigating prescriber adherence to established specialist guidelines using electronic health records and prescribing systems, it was not fitting to involve patients and the public in the design, conduct or reporting of the project.
Results
Group characteristics
In the preintervention period, there were 27 perioperative VRIII prescriptions for 23 individual patients, the difference accounting for some patients requiring more than one procedure during admission. In the postintervention period, there were 18 prescriptions for 17 patients. In the reaudit period, there were 26 prescriptions for 22 patients. Across all groups, type 2 diabetes was more common than type 1 diabetes (79% vs 21%). The average glycated haemoglobin test (HbA1c) within 3 months of operation was 83 mmol/mol (range: 41–152). The average starting capillary blood glucose was 9.2 mmol/mol (range: 3.2–22.4).
Was VRIII appropriate for the situation?
According to JBDS-IP guidelines, there are five scenarios in which perioperative VRIII is indicated:
Type 1 diabetes+more than 1 missed meal.
Type 1 diabetes+has not received background insulin.
Type 2 diabetes+more than 1 missed meal+capillary blood glucose >12 mmol/mol.
Type 1 or 2 diabetes+HbA1 c >69 mmol/mol.
Type 1 or 2 diabetes+emergency surgery.
Overall, VRIII was appropriate for the situation in 85% (60/71) of cases. VRIII was indicated for the majority of patients included in the study (76%, 47/62) on the basis of poorly controlled disease alone; that is, HbA1C >69 mmol/mol. There was no significant difference in the proportion of unnecessary prescriptions between the preintervention (19%, 5/27), postintervention (28%, 5/18) and reaudit (4%, 1/26) groups (p=0.102). Every VRIII prescription made inappropriately was for type 2 diabetics with HbA1c <69 mmol/mol and starting capillary blood glucose <12 mmol/mol.
Starvation periods and operation delays
In the preintervention period, 13 of 23 patients (57%) experienced at least one cancellation. Invariably, these patients were starved for the day and then had their operation cancelled in the evening (ie, rearranged for the following day) due to a high volume of acute theatre cases. Patients experienced an average of three missed meals on the day an operation was cancelled and two missed meals on the day an operation was performed. There were four occasions where just one meal was missed before surgery.
In the postintervention period, 7 of 17 patients (41%) experienced at least one cancellation. Patients experienced an average of 1.7 missed meals on the day an operation was cancelled and 1.6 missed meals on the day an operation was performed. There were ten occasions where just one meal was missed before surgery.
In the reaudit period, 5 of 22 patients (23%) experienced at least one cancellation. Patients experienced an average of 2.1 missed meals on the day an operation was cancelled and 1.7 missed meals on the day an operation was performed. There were eight occasions where just one meal was missed before surgery. Overall, in the postintervention and reaudit cohorts, there were fewer cancellations, cancellations were made earlier in the day and more patients were operated on earlier in the day compared with the preintervention cohort.
Prescribing practices
The ‘refer to paper chart’ dummy drug on eMeds was prescribed on 9 of 27 occasions (33%) in the preintervention period, on 12 of 18 occasions (67%) in the postintervention period and on 20 of 26 occasions (77%) in the reaudit period (figure 1). Intravenous glucose as a rescue medication was never prescribed alongside VRIII in the preintervention period but was prescribed on 9 of 18 occasions (50%) in the postintervention period and on 17 of 26 occasions (65%) in the reaudit period (figure 2). The increased frequency of prescribing of the ‘refer to paper chart’ dummy drug and rescue medication was statistically significant (p=0.046 and p<0.001, respectively). Altogether, 8 patients experienced hypoglycaemia (defined as CBG <4.0 mmol/mol) while on VRIII (2/23 patients in preintervention period, 3/17 postintervention and 3/22 reaudit). One patient in the preintervention period, two in the postintervention period and one in the reaudit period required intervention with supplemental glucose.

The ‘refer to paper chart’ dummy drug was prescribed more frequently in the postintervention (12/18, 67%) and reaudit (20/26, 77%) periods than in the preintervention period (9/27, 33%).

Prescription of intravenous glucose as a rescue medication increased from 0% in the preintervention period to 50% in the postintervention period and then to 65% in the reaudit period.
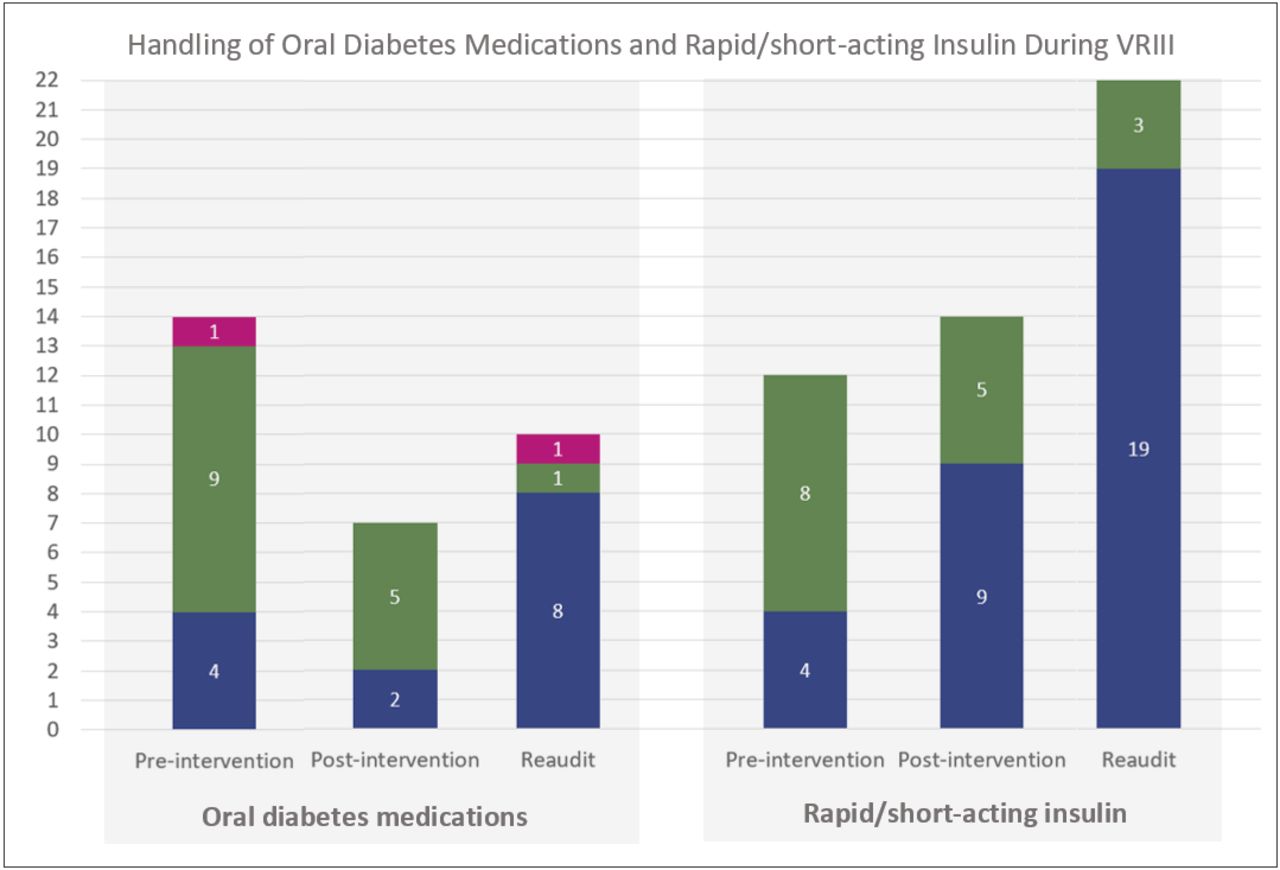
In the preintervention period, oral diabetes medication was appropriately withheld during VRIII on 13 of 14 occasions (93%)—either by nursing staff at the time of administration (9/14, 64%) or by a doctor on the prescription chart (4/14, 29%) (figure 3). There was one occasion where metformin was administered inappropriately during VRIII. In the postintervention period, oral diabetes medication was appropriately withheld during VRIII on all 7 occasions—either by nursing staff at the time of administration (5/7, 71%) or by a doctor on the prescription chart (2/7, 29%). In the reaudit period, oral diabetes medication was appropriately withheld on 9 of 10 occasions (90%)—either by nursing staff at the time of administration (1/9, 11%) or by a doctor on the prescription chart (8/9, 89%). There was one occasion where linagliptin was administered inappropriately during VRIII. There was no significant difference in the proportion of oral diabetes medication appropriately withheld across the three study periods (p=0.602).
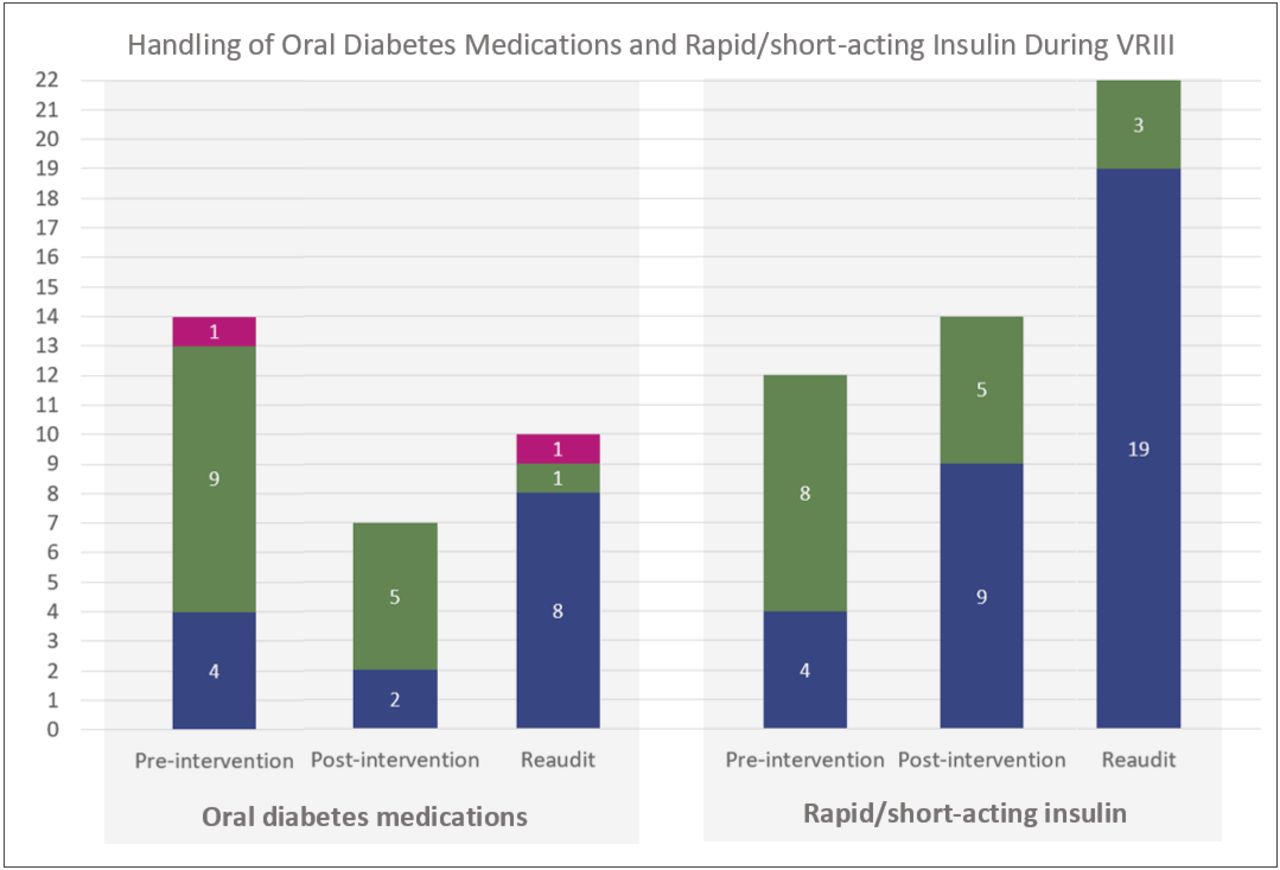
Data labels represent the number of instances in each category—withheld by a doctor on the prescription chart (blue), withheld by nursing staff at the time of administration (green), given inappropriately during VRIII (pink). VRIII, variable rate intravenous insulin infusion.
Rapid/short-acting insulin was appropriately withheld on every occasion in the preintervention, postintervention and reaudit periods. In the preintervention period, rapid/short-acting insulin was withheld more often by nursing staff at the time of administration (8/12, 67%) than by a doctor on the prescription chart (4/12, 33%). In the postintervention and reaudit periods, rapid/short-acting insulin was withheld more often by a doctor on the prescription chart (9/14, 64% and 19/22, 86%, respectively) than by nursing staff at the time of administration (5/14, 36% and 3/22, 14%, respectively).
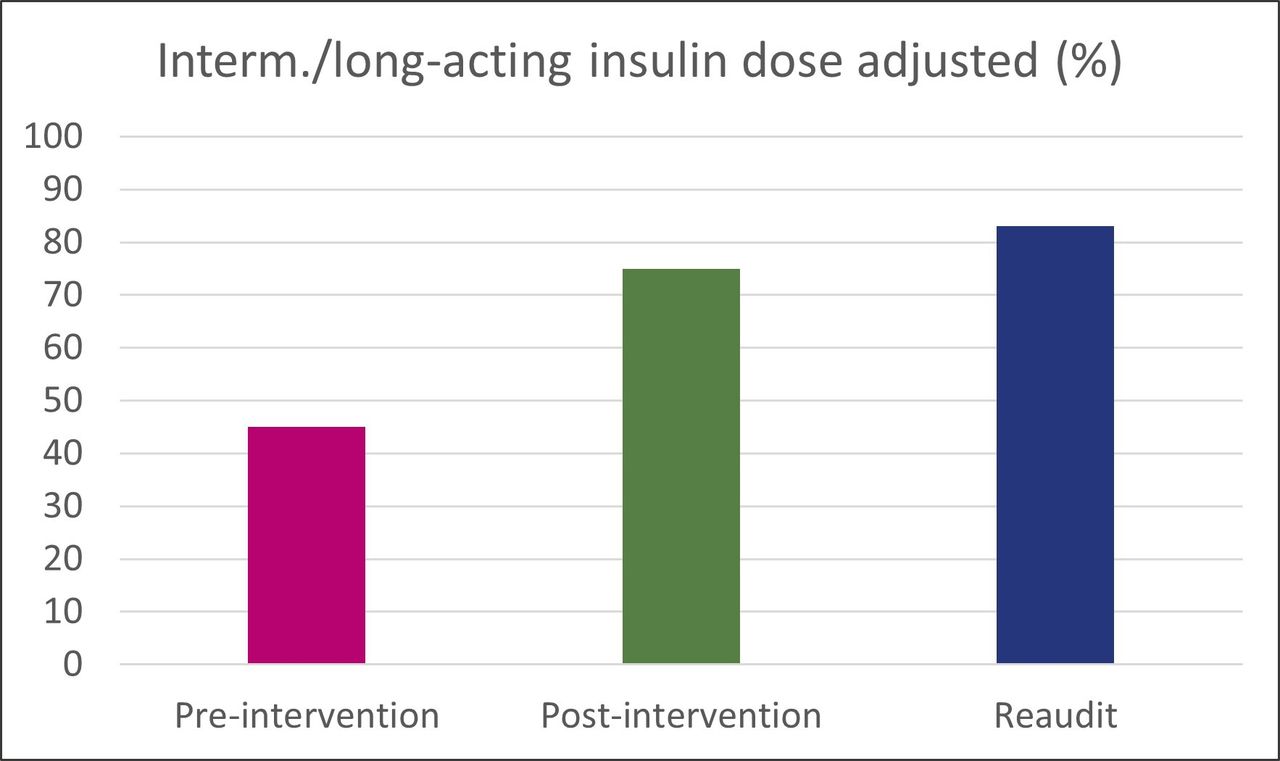
Intermediate/long-acting insulin was appropriately reduced to 80% of the patient’s normal dose during VRIII on 5 of 11 occasions (45%) in the preintervention period, on 9 of 12 occasions (75%) in the postintervention period, and on 5 of 6 occasions (83%) in the reaudit period (figure 4). Improvement in the frequency of intermediate/long-acting insulin dose adjustment was statistically significant (p=0.041). Most of the time where intermediate/long-acting insulin was not appropriately amended, the full dose was given. On one occasion in each of the preintervention and reaudit periods, the long-acting insulin was completely withheld during VRIII.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intermediate/long-acting insulin doses were appropriately amended to 80% of the patient’s normal dose more often in the postintervention period (9/12, 75%) and reaudit period (5/6, 83%) than in the preintervention period (5/11, 45%).
Discussion
Perioperative VRIII prescribing practices improved following interventions, with prescribers more frequently utilising recommended safety measures such as ‘refer to paper chart’ and rescue medication. More consistent application of the ‘refer to paper chart’ dummy drug not only intended to raise ward staff awareness of which patients were on VRIII but also led to improvements in prescribing of rescue glucose, as these two actions were linked on the electronic prescribing system during the intervention period. As demonstrated in this study, supplemental glucose is occasionally required to correct hypoglycaemia during VRIII, making this an important step with regard to patient safety when commencing an insulin infusion. There was a marked improvement in prescriber-initiated withholding of rapid/short-acting insulins and adjustment of intermediate/long-acting insulin doses. Reaudit following rotation of a new cohort of junior doctors into the department demonstrated not only a sustained change but further improvements across all areas of perioperative VRIII prescribing (online supplemental appendix 2). This finding may be accounted for by two key considerations: (1) the inclusion of a short talk on VRIII prescribing in the junior doctor induction session between the postintervention and reaudit periods, and (2) each project period coincided with rotation of progressively more experienced junior doctors into the department. Our vascular surgery ward was staffed with newly qualified doctors during the preintervention period, those with at least 4 months of junior doctor experience in the postintervention period, and at least 8 months experience in the reaudit period. It is not possible to determine, however, how much of the doctors’ previous rotations involved VRIII prescribing.
Although the VRIII Prescribing Checklist was expressly designed with an abridged list of indications, prescribers continued to commence infusions for patients with relatively well-controlled type 2 diabetes and a low capillary blood glucose. In this context, the protocol should be to monitor capillary blood glucose hourly during the starvation period and initiate VRIII only if the level rises above 12 mmol/mol. It is possible that, with monitoring, the blood glucose level may have risen above this threshold therefore necessitating VRIII, but at the time it was commenced, strictly speaking it was not indicated. According to the NDIA, the rate of VRIII overuse is approximately 6%,12 notably less than the 15% of inappropriate prescriptions reported in this work. Our findings may stem from inadequate prescriber understanding of the indications for VRIII or a lack of prescriber confidence to not start an insulin infusion for a patient with diabetes being starved for surgery. Pending further research in this area, additional interventions to educate and empower prescribers may lead to a reduction in such unnecessary insulin infusions. On the other end of the spectrum, VRIII underuse is seldom reported in the literature and deserves investigation as a patient safety issue. A recommendation for future iterations of this or similar studies would be to expand the inclusion criteria to all patients with diabetes who underwent surgery to determine whether there are patients not started on perioperative VRIII despite meeting JBDS-IP guidelines for it.
Diabetic vascular surgery patients on our ward experienced prolonged starvation periods and frequent delays in surgery and this was predominantly attributed to high caseload pressures on acute theatres. The gold standard, as published in the JBDS-IP guidelines, is for patients with diabetes to have priority on a daily operating theatre list. Only 4 of 23 patients (17%) were listed first in the preintervention period, although this increased to 10 of 17 patients (59%) in the postintervention period. Overall, there were shorter starvation periods and fewer cancellations in the postintervention and reaudit periods. The explanation for this is unclear but is likely multifactorial. During the intervention phase, audit findings were shared at the Vascular Surgery Governance Meeting, which served to raise awareness of key issues such as theatre delays to an audience of vascular surgery consultants. It is possible that caseload pressures were lower in the postintervention period compared with the preintervention period. Ultimately, an element of chance cannot be excluded as sample sizes were relatively small.
Prescribers and nursing staff consistently withheld patients’ oral diabetes medications and rapid/short-acting insulins appropriately while VRIII was running. Although nursing staff continued to bear most of the responsibility for withholding oral diabetes medications during the postintervention period, this shifted to predominantly prescriber-initiated withholding in the reaudit period. This is an important distinction as it directly impacts patient safety. When the prescriber withholds such medications on the chart at the time of VRIII prescription, it ensures that these cannot be administered mistakenly (which took place on two occasions in this study). On the contrary, there was more rapid improvement in prescriber-initiated withholding of rapid/short-acting insulins. Similarly, intermediate/long-acting insulin doses were amended considerably more often in the postintervention than preintervention period. In the reaudit period, prescribers demonstrated sustained improvement in initiating appropriate changes to patients’ insulin and oral diabetes medications when commencing VRIII. These positive results may be attributable to the combination of the VRIII Prescribing Checklist, targeted teaching and eMeds reinforcing messages.
The breadth and depth of study of local VRIII prescribing practices is a strength of this quality improvement project. Baseline, postintervention and reaudit data were collected by the same researcher to reduce inter-rater variability. Interventions were designed using a collaborative approach between doctors, pharmacists and endocrinology specialists. This has resulted in a VRIII Prescribing Checklist that has relevance well-beyond the Vascular Surgery ward. Indeed, other surgical wards in our hospital have started to implement this tool to better inform prescribers of perioperative VRIII within their clinical area. Due to the nature of the specialty, vascular surgery has a high proportion of patients with uncontrolled diabetes, which therefore necessitates the frequent use of perioperative VRIII. Although it may not be required as commonly on other surgical wards, it is just as important that prescribers in these areas can initiate perioperative VRIII safely. One of the main limitations of this project stemmed from the variability in eMeds used between hospitals. Interventions involving eMeds updates are not relevant for sites using other systems, therefore, limiting generalisability. Another disadvantage is the impermanence of educational interventions. Junior doctors rotate every 4 months and, as the primary prescribers of VRIII on the ward, this necessitates teaching at regular intervals. To address this challenge, a VRIII prescribing session has been incorporated into the departmental junior doctor induction, which is now held for every new cohort.
Conclusion
Local perioperative VRIII prescribing practices more closely met the standards set the by the JBDS-IP following implementation of a Prescribing Checklist, eMed updates and education for junior doctors and ward staff. With advancements made in the quality and safety of prescribing practices on our vascular surgery ward, there remains room for improvement in reducing the number of potentially unnecessary insulin infusions for a subset of patients with type 2 diabetes.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This project was registered and authorised on the Trust-wide Clinical Audit Database. Ethics approval was not required for this clinical audit.
Acknowledgments
We gratefully thank Mr Ryan Laloofor his assistance with the statistical analysis.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KA, NO and KS-J conceived of the idea. KA designed and led the project. KA and HB performed data collection. KA, NO, KS-J, NB and SK collaborated to develop project interventions. KA performed data analysis and interpreted results. All authors discussed the results and provided feedback at critical steps in the project. JF supervised the project. KA wrote the manuscript with support from JF and NO. KA is the guarantor for this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.