Article Text

Abstract
Objectives To evaluate implementation of digital National Early Warning Score 2 (NEWS2) in a cardiac care setting and a general hospital setting in the COVID-19 pandemic.
Design Thematic analysis of qualitative semistructured interviews using the non-adoption, abandonment, scale-up, spread, sustainability framework with purposefully sampled nurses and managers, as well as online surveys from March to December 2021.
Settings Specialist cardiac hospital (St Bartholomew’s Hospital) and general teaching hospital (University College London Hospital, UCLH).
Participants Eleven nurses and managers from cardiology, cardiac surgery, oncology and intensive care wards (St Bartholomew’s) and medical, haematology and intensive care wards (UCLH) were interviewed and 67 were surveyed online.
Results Three main themes emerged: (1) implementing NEWS2 challenges and supports; (2) value of NEWS2 to alarm, escalate and during the pandemic; and (3) digitalisation: electronic health record (EHR) integration and automation. The value of NEWS2 was partly positive in escalation, yet there were concerns by nurses who undervalued NEWS2 particularly in cardiac care. Challenges, like clinicians’ behaviours, lack of resources and training and the perception of NEWS2 value, limit the success of this implementation. Changes in guidelines in the pandemic have led to overlooking NEWS2. EHR integration and automated monitoring are improvement solutions that are not fully employed yet.
Conclusion Whether in specialist or general medical settings, the health professionals implementing early warning score in healthcare face cultural and system-related challenges to adopting NEWS2 and digital solutions. The validity of NEWS2 in specialised settings and complex conditions is not yet apparent and requires comprehensive validation. EHR integration and automation are powerful tools to facilitate NEWS2 if its principles are reviewed and rectified, and resources and training are accessible. Further examination of implementation from the cultural and automation domains is needed.
- qualitative research
- nurses
- attitude of health personnel
- clinical decision-making
- implementation science
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- qualitative research
- nurses
- attitude of health personnel
- clinical decision-making
- implementation science
WHAT IS ALREADY KNOWN ON THIS TOPIC
Very little is known about the implementation of electronic health record (EHR)-integrated early warning score (EWS) and the perception of clinicians in different hospital settings.
WHAT THIS STUDY ADDS
The challenges and facilitators of implementing National Early Warning Score 2 (NEWS2) can be system related or culture related.
Facilitating NEWS2 through EHR integration and automation can support the implementation when resources and learning are provided.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The study identifies the factors that need to be investigated and rectified in hospital settings to achieve the aims of EWS and reduce further adverse events.
Findings can inform policy makers and system developers to consider clinicians’ opinion when planning further implementation in different settings.
Introduction
Prediction tools in acute care settings can improve patient safety through enhanced efficiency of care and reduced pressure on health systems.1 Early warning scores (EWS) are a potential solution to decrease critical events, unnecessary deaths and debilitating resources.2–4 EWS have become part of the escalation guidelines directing clinicians to the level of care needed.5 The National Early Warning Score 2 (NEWS2), the latest advocated EWS in the UK, is a simple aggregate scoring system in which a score is allocated to physiological parameters recorded in routine practice, that is, respiratory rate.6 The score indicates the risk of developing a critical event and the level of care needed.6 In conjunction, clinicians use their education and clinical experience, as when EWS did not exist, to make clinical judgements.7 8 Implementing EWS advises clinical assessment when puzzles are missing from knowledge and experience.
However, there is a gap in evidence on the performance of EWS in predicting critical events, that is, intensive care unit (ICU) transfer or in-hospital mortality, in different settings and specialties.9–12 For instance, in cardiac care and complex comorbidities, that is, patients with COVID-19, the performance of EWS is poor and research is in the early stages.9 13 Equally, there is a lack of evidence on implementing integrated EWS in electronic health records (EHR) in specialised clinical settings.9 14 With the electronic assessment recording, EWS scores and alarms are produced automatically, facilitating its utilisation by clinicians. The functionality gives more confidence in EWS generated when part of the burden becomes the role of the machine. It has improved clinical outcomes and staff workflow.15
For EWS to be successful, they have to be executed accurately. Errors in assessment, recording and escalation of care contributed to 20%–80% of the severe adverse events (SAE).16 As shown in previous EWS and digital solutions, wide dissemination does not necessarily lead to successful adoption.17 It is well established that failure of EWS is related to patients’ physiology or professionals’ practice, that is, poor adherence to the prescribed protocol for deterioration.17 18 In addition, the downsides of automated monitoring, that is, measurement errors, artefacts and false alarms,19 can challenge the progress needed. In times of increased work demand and patient acuity, such as in the COVID-19 pandemic, there are higher chances of human and system errors leading to SAE. NEWS2 was formally endorsed by National Health Service (NHS) England for standardised care for acutely ill patients20; however, there are limited findings to indicate a reliable performance and successful implementation in specialist settings.21 22 The significance of NEWS2 and automated application is only valuable if resulting in a tangible improvement.
The limited studies in implementing EWS in specialist settings and the lack of investigation of EHR integration indicate the need to explore clinicians’ perception when implementing EWS in different settings. Therefore, we conducted a qualitative study of EHR-integrated NEWS2 in a specialised cardiac, and a general hospital, from the perception of nurses using it. As EHRs were implemented in the two settings recently from 2019 to 2020 and followed by NEWS2 integration, examining the implementation would bring evidence-based findings to improve the practice of EHR-integrated NEWS2 as a health service.23 On the other hand, examining clinicians’ perceptions in a general setting with different care pathways, specialties and structures may show the impact of clinical care setting and work culture-related factors in implementing digital NEWS2. Not to mention, the COVID-19 complexity as a disease and the burden created in healthcare settings may influence clinicians’ adoption and perception of NEWS2. The non-adoption, abandonment, scale-up, spread, sustainability (NASSS) tool24 is a pragmatic, evidence-based design that can provide a thorough understanding of digitally supported tools in healthcare. Due to the application of electronic recording and automation, we followed the NASSS framework in the study.
Previous implementation studies
EWS models that proceeded NEWS2 were examined from nurses and doctors’ experiences in acute and non-acute settings. In a study in Norway, modified EWS 2 supported early recognition and knowledge sharing between nurses.25 Another study found that nurses value NEWS as it incorporates their knowledge and judgement, yet may not necessarily lead to desired clinical outcomes.26 In non-acute settings, it is believed to facilitate communication and decision-making. However, EWS used in emergency departments (ED) Hamilton early warning score (HEWS) was unvalued by physicians and nurses.27 HEWS may not be as advanced as NEWS and NEWS2 in development. Nonetheless, results from specialised departments like ED demonstrate the need to examine settings with unique functionality. The negative experience of NEWS caused tension when it was implemented.28 Compliance, workload pressure and discrepancies between clinical judgement and the scores generate workplace anxiety.17 28 As pressure increases in busy hours, defective collaboration and miscommunication arise between clinicians leading to failed implementation.17 The experience of EHR-integrated EWS in specialised settings is missing from the literature.
Objectives
To qualitatively evaluate the success and role of implementing EHR-integrated NEWS2 from nurses’ perception in a cardiac specialist and general hospital settings in the COVID-19 pandemic.
Methodology
Study settings
Setting 1
St Bartholomew’s (Barts) is a cardiac specialist and teaching hospital in London and has heart and cancer centres with other related specialties. The hospital has 387 inpatient beds.
NEWS was first implemented in 2012, followed by the updated version NEWS2 in 2018. The EHR system went live in 2020. NEWS was shortly shifted from paper to EHR-embedded format calculated from each vital sign’s measurements via Cerner. NEWS2 update was reflected in EHR systems. In addition, automated monitoring was introduced in Barts in 2021. It is a centre for cardiac and cancer care and provides a number of services for endocrinology, fertility, thoracic and a minor injuries unit. Patient observation and escalation using NEWS2 is part of the mandatory training for nurses and is governed by the trust’s policies and guidelines for observing and escalating adult patients.
NEWS2 pathway in Barts
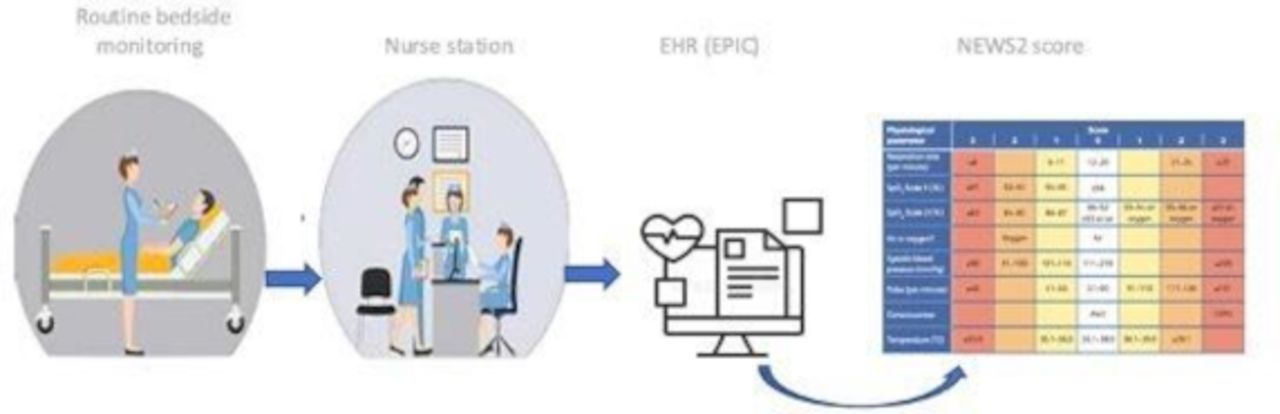
NEWS2 begins with assessment and vital sign measurement by nurses and nurse assistants via automated monitoring devices (Welch Allyn Connex Spot Monitor). Monitors are connected to Cerner, transmitting measurements directly to patients’ charts. NEWS2 is calculated automatically in the electronic chart; a score is given, then an alarm is shown when a score indicates the need for intervention. Clinicians need to log in to view the score of the patient (figure 1).

National Early Warning Score 2 (NEWS2) pathway through electronic health record (EHR) integration and automated monitoring1 in St Bartholomew’s Hospital (Barts).
Setting 2
University College London Hospital (UCLH) is a general teaching hospital. It includes various specialties, such as accident and emergency, stroke unit, cancer care, critical care, general surgery, general medicine and neurology. It has 665 inpatient beds. NEWS was first implemented in 2012, followed by the updated version NEWS2 in 2018. The EHR system went live in 2019 in UCLH; then, NEWS was shortly shifted from paper to EHR-embedded format calculated from each vital sign’s measurements via EPIC in UCLH. Routine monitoring using NEWS2 is a mandatory learning module in the UCLH eLearning portal.
NEWS2 pathway in UCLH
Nurses and nurse assistants do routine vital measurements. They input their recordings physically into the patient’s chart in EPIC. The score is calculated automatically, and an alarm will show when the status indicates attention. Nurses and physicians view the score when logged in to their patients’ charts (figure 2).

National Early Warning Score 2 (NEWS2) pathway through electronic health record (EHR) integration in University College London Hospital (UCLH).
Study framework
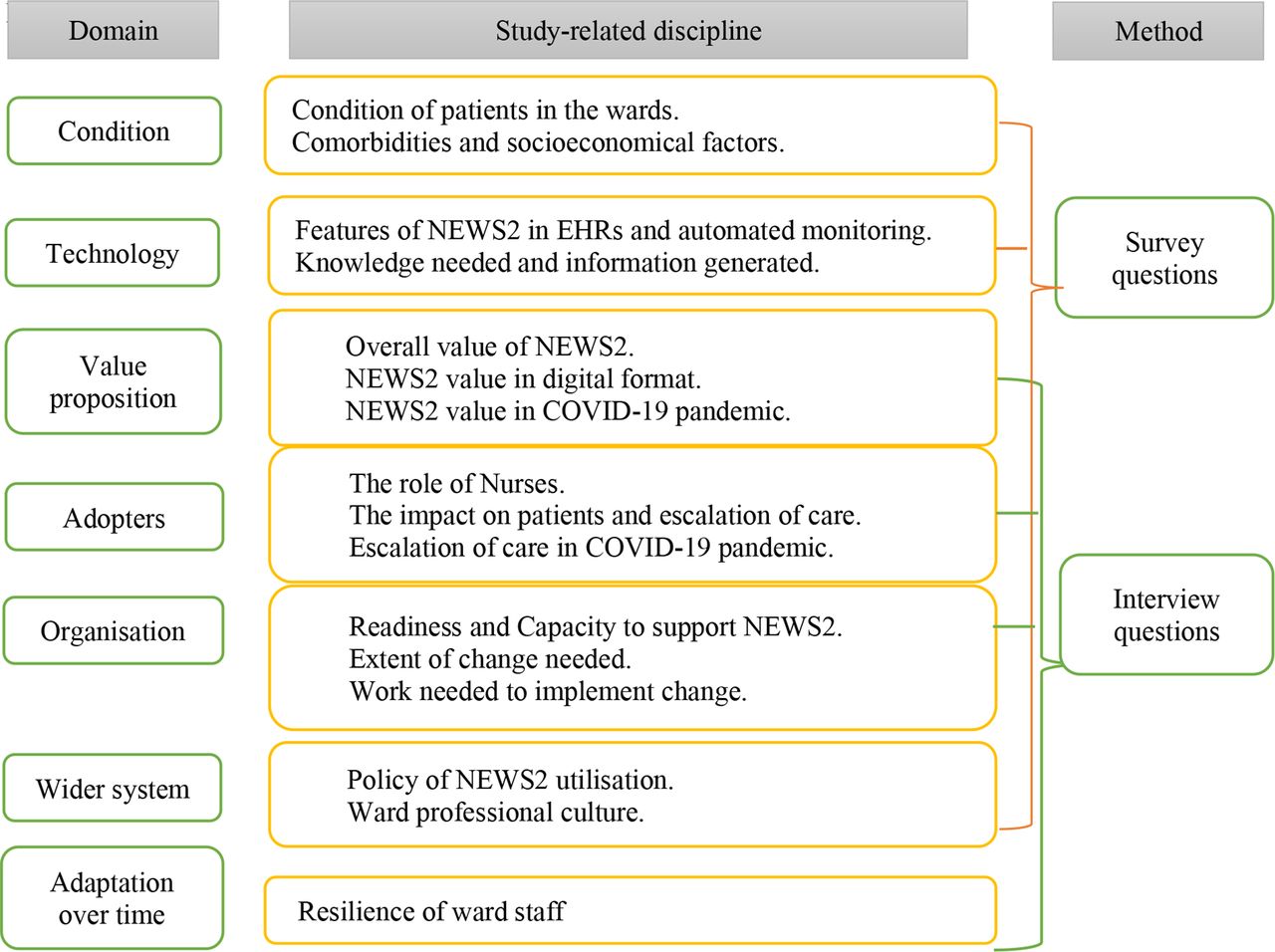
We conducted a qualitative study design to evaluate the implementation, following the NASSS framework.24 The NASSS design was chosen for its compatibility with evaluating the adoption of digitalised health systems in healthcare settings. The factors in the framework were rephrased to present the process of implementing NEWS2 and to guide structuring questions around the investigated areas (figure 3).
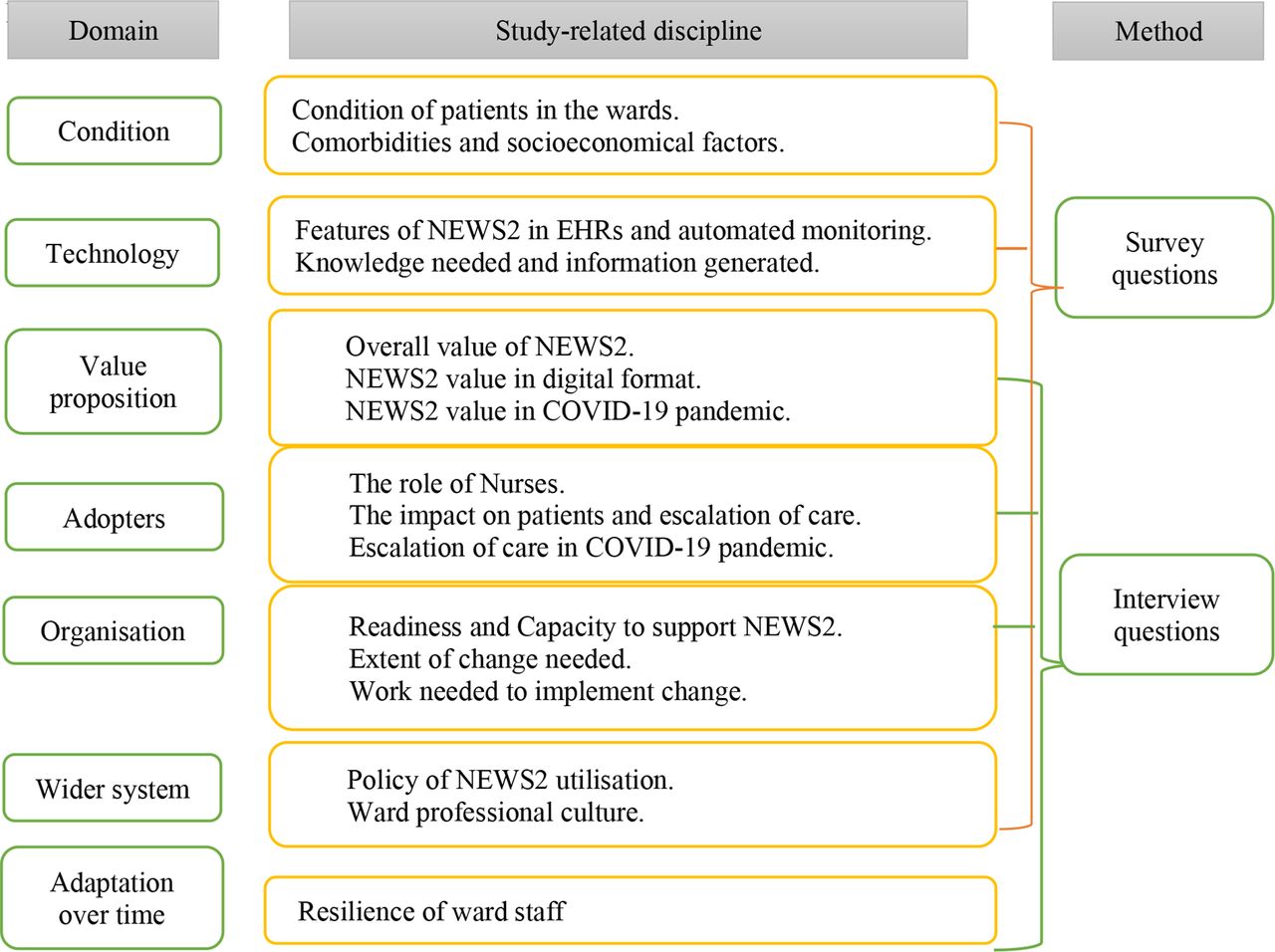
Non-adoption, abandonment, scale-up, spread, sustainability (NASSS) framework domains and methods in the study. EHR, electronic health record; NEWS2, National Early Warning Score 2.
Data collection
A purposive sampling method was followed with input from the research team, the critical care outreach team (CCOT) and resuscitation team in Barts and patient emergency response team in UCLH to identify representative participants to contact based on roles and experiences in using NEWS2. Focus groups were initially planned to gather a collaborative perception of nurses from different hierarchical and role levels: ward nurses and managers. A staff nurse is a qualified registered nurse who delivers direct care to the patient; a nurse manager is a more senior nurse responsible for managing nurses, drawing together patient experiences and coordinating with the multidisciplinary team, that is, charge nurse or ward manager. Invitation emails for focus groups were sent in March 2021 to ward managers and nurses in the cardiac specialist hospital, and a follow-up email was sent 10 days later. Due to the workload pressure during the pandemic, assigning participants to the focus group at one time was impractical. Therefore, as discussed with the research team, it was decided to conduct individual interviews (online supplemental appendix 2). Invitation emails to online interviews were sent in April 2021 to 10 nurses and managers in Barts, and equally to UCLH staff in June, followed by a reminder after 10 days. Information sheets and consents were sent before setting a date for interviews. Informed consent was obtained prior to conducting the interviews.
Supplemental material
A questionnaire was created in SmartSurvey,29 including consent to answer the survey. A link was sent to nurses and managers in cardiac and non-cardiac wards: cardiology, cardiac surgery, haematology and oncology wards and ICU in Barts; and medical, oncology and haematology wards and ICU in UCLH. Wards in UCLH were chosen to provide a mutual environment of patients’ specialty to Barts. Survey questions were matched, excluding the automated monitoring part in UCLH survey (online supplemental appendix 1). A reminder was sent after 14 days to boost participation. The data collection period was 8 months in total.
Data analysis
Interviews were recorded in teams then saved with surveys in the NHS network. Recordings and surveys were pseudorandomised then transferred to UCL Data Safe Haven (DSH), a secured database system with restricted access to the principal investigator (PI) and chief investigator (CI), via safe gateway technology. Transcription of audio recordings and analysis of transcriptions and surveys were done in NVivo. Survey data were extracted from SmartSurvey and analysed in NVivo.
The interviews were analysed thematically to enable us to identify shared ideas and experiences and recognise patterns in data sets.30 Themes were derived from coded data during the analysis process. The analysis followed five steps—first, familiarity with the interview by listening to the audio and reading the transcription by BA. Script and audio were compared by BA and AB to achieve reliability. Second, initial codes were assigned to parts of the text by BA with relevancy to the domains in the framework and reviewed by AB. Third, identifying relevant themes and subthemes that capture the idea of significance. Fourth, themes and subthemes were checked by BA and AB to assess their quality. Fifth, themes were organised and named according to the relativity with the research aim, and the framework domains examined. For the survey answers, quantifiable data from answers were analysed descriptively. Results were used to support the findings in the theme formed from the interviews. This step is conducted by comparing the interview results to the survey response, exploring the same factor, or leading to a unified theme to find the level of agreement between responses. The comparison method has been done in medicine and psychology research to measure the level of validity in findings.31 Discussion with the research team was carried out until an agreement was reached on the main themes produced. Results were reviewed and double-checked independently by BA and AB. Finally, the results report comprises four main themes, then exported from DSH.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Eleven nurses and managers participated in interviews that lasted 35 min each. Survey respondents were 67 nurses and managers.
Interviews
In the cardiac setting, six staff responded, and four agreed and were interviewed. In the general hospital, seven nurses participated: three interviewed from the first invite. After follow-up emails, five responded, and four were interviewed (table 1).
Characteristics of interviews and survey respondents
Questionnaires
Twenty-eight staff answered the surveys in the cardiac setting, from cardiology, critical care, medical and oncology. From the general hospital, 39 answered the questions from critical care, medical and oncology wards (table 1).
Themes
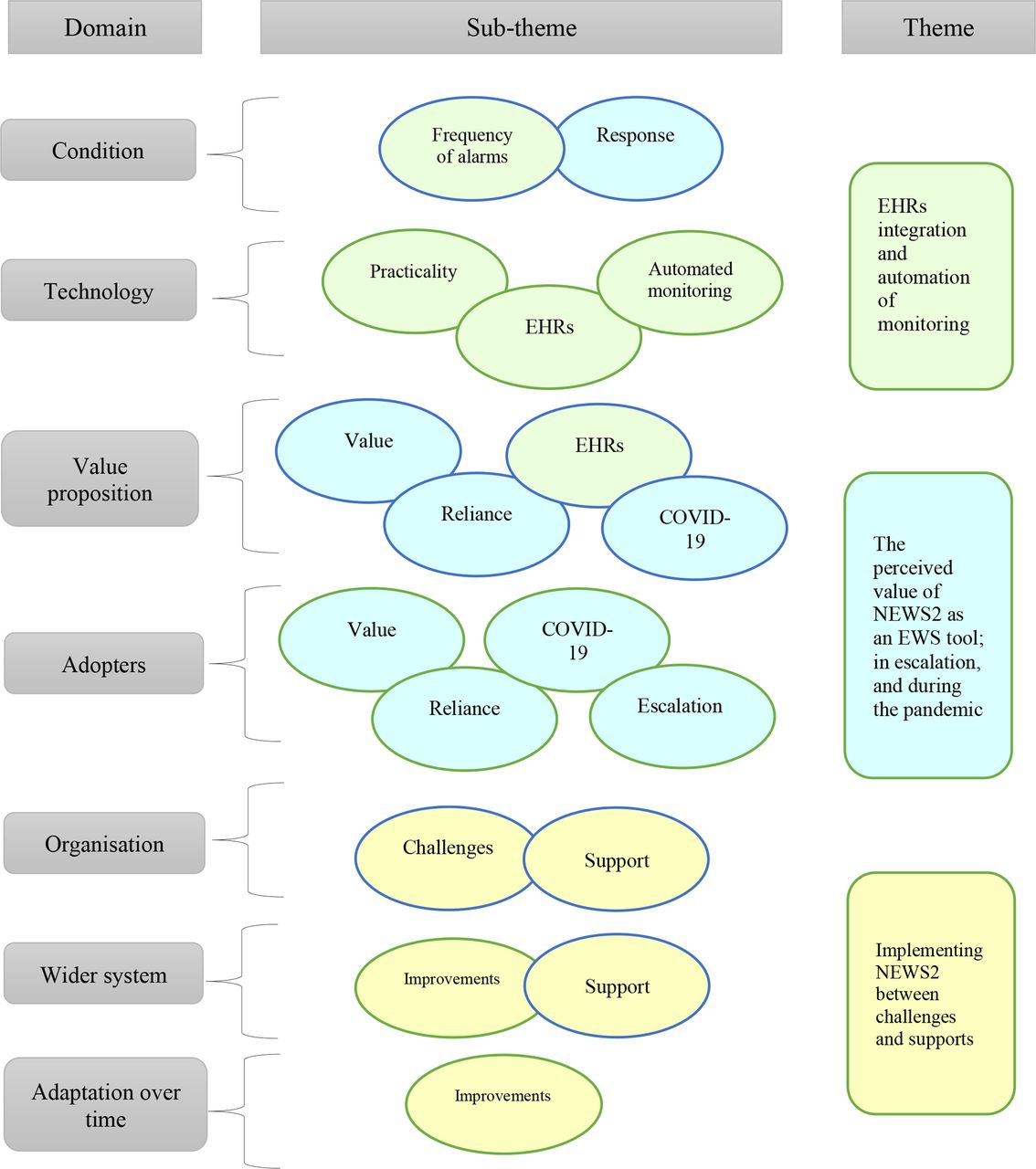
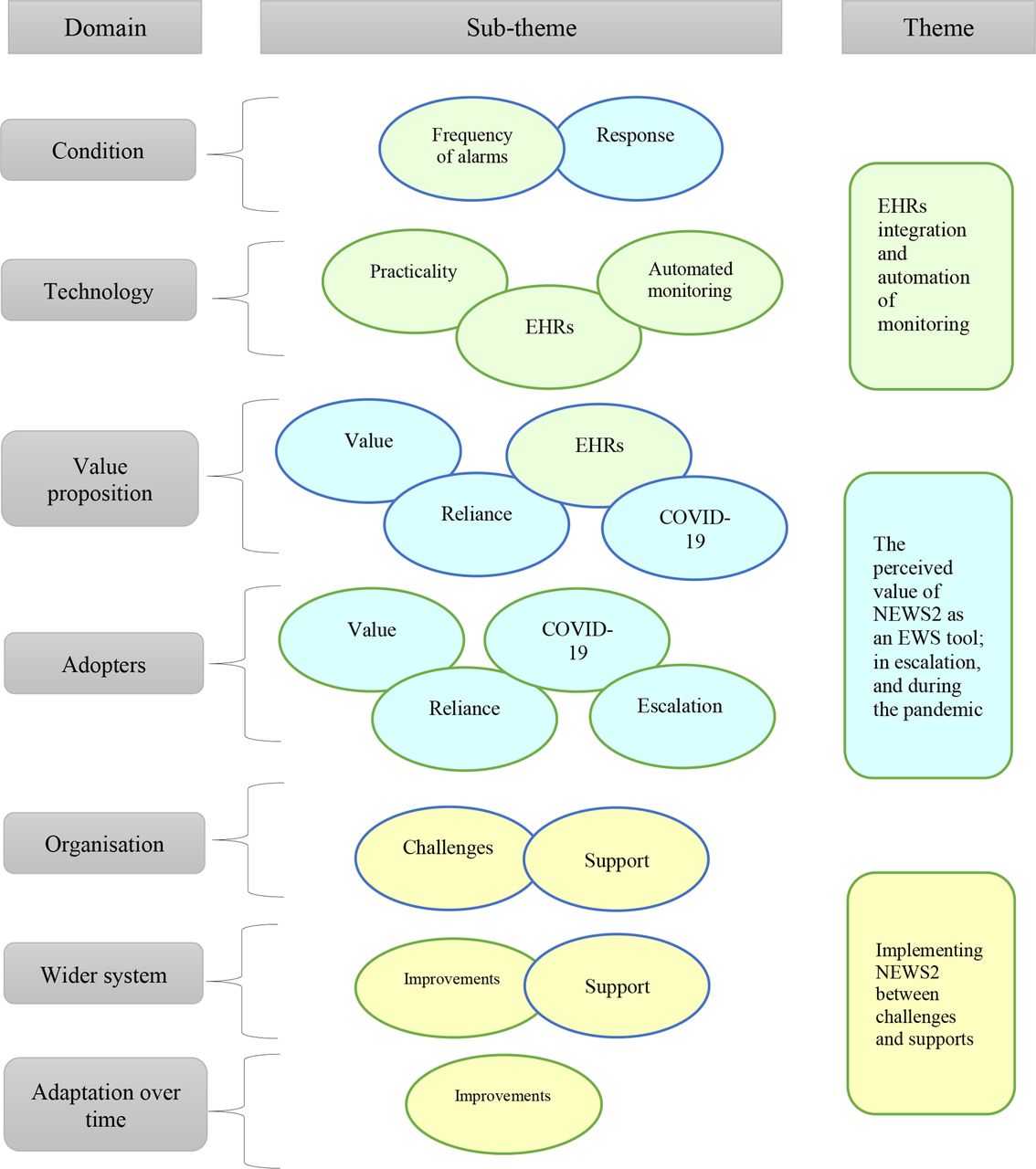
Three themes emerged from applying the NASSS framework on studying the success of implementing NEWS2 in the two hospitals. The themes from domains were as follows: (1) NEWS2 between challenges and supports; (2) the perceived value of NEWS2 as an alarming tool, in escalation and during the pandemic; (3) digitalisation: EHR integration and automation of monitoring. Some domains from the framework intersect in themes due to the relativity in subthemes to more than one domain (figure 4). Results from the survey served as a supplement that supported the themes. Table 2 explains the characteristics of the interviewees’ hospital setting and digital system.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Themes and subthemes emerging from the non-adoption, abandonment, scale-up, spread, sustainability (NASSS) framework domains. Bubble colours relate subthemes to the main themes formed. EHR, electronic health record; EWS, early warning score; NEWS2, National Early Warning Score 2.
Culture and system characteristics of interview participants
NEWS2 between challenges and supports
The difficulties found by nurses and managers were human-related, tool-related and resource-related factors.
From the human-centric side, junior nurses worry if their judgement for escalation is based on NEWS2, and their knowledge is inaccurate or undervalued. On the other hand, clinicians and rapid response teams may not always be cooperative when escalation is reported, resulting in timidness by junior staff and avoiding being involved in escalation.
I think NEWS2 can be unhelpful when I see how the medical team behave in the situation. (Sm)
It’s about increasing the psychological safe space to speak up no matter who you are. We’re not quite there yet. (Gm)
The information technology (IT) literacy and interest difference between staff cause a gap in adopting NEWS2 in EHRs in both hospitals. Resistance or delays in learning lead to errors in documentation and obstruct escalation.
Documentation isn’t Great. (Sm)
Because it’s an electronic system, some staff aren’t particularly comfortable using IT equipment. So, they do the Observation, write on a piece of paper, then enter it later. (Gm)
NEWS2 parameters were considered problematic. Their format may not be appropriate for the patient group, specifically cardiac patients, as reported from both sites. There’s a frequent need for parameter adjustment to suit a patient’s medical history to avoid repetitive alarms. Adjustment is challenging as this role is assigned to doctors only.
The problem with it is that the medical team needs to input the target parameters, and only when they do that it does trigger NEWS2. (Gs)
Particularly I think cardiology patients need parameter changing. (Sm)
Poor resourcing of equipment and staff affects the adoption negatively. When workstations are occupied, recording may be incorrect, and escalation is delayed, yet the issue may not be present in the specialist hospital, where automated monitoring occurs. In addition, nursing assistants who do routine monitoring are not as trained as registered nurses. Reporting deterioration can be missed or delayed.
The healthcare assistants do the observation, then by the time they report, or maybe they forget to tell you the patient is scoring five or six. (Ss)
We sometimes don’t have access to an EHR machine because they’re busy or broken, or we haven’t got enough, or we don’t have access to the handheld devices. (Gm)
From the support side, nurses and managers had a consensus on the benefits training provided in both sites. However, training has declined due to the pandemic pressure in the workplace. They reported significant support by the hospital management to use NEWS2 and adopt the EHR-integrated version, including induction programme training. Ongoing guidance by informatics experts, superusers and ward managers showed a culture of appreciating the management support as reported in surveys and interviews. Nonetheless, lack of training and auditing is an issue in both sites. An emphasis was reported on structuring a clear step-by-step process for implementation. Quality projects that focus on improving documentation and escalation, such as deteriorating patient’s dashboard project in the specialist hospital, were valued by staff in both sites.
I think they are supporting it. But I do think it’s a shame that, throughout the pandemic, it’s not audited anymore. (Sm)
Other hospitals created dashboards of patients scoring high for users and outreach team to focus on. (Gm)
Some nurses in general hospitals perceive it as a mandatory tool rather than a choice yet agree to follow. Resilience was subject to personal and experience differences, such as age and recurrent guideline updates. Younger staff were reported to be more receptive to change than older staff.
They are quite resilient because there has been much structural process, which has changed constantly, the team have taken them forward quite well. (Gs)
They easily pick up on the new electronic things; it’s quite a young team. (Gs)
Some don’t change because they find the computer stuff and everything a little bit difficult. (Ss)
Perceived value of NEWS2 to alarm, escalate and in the pandemic
Overall, nurses and managers believed NEWS2 helps prioritise patients’ needs according to acuity, therefore improving patient safety. They valued the unified language between clinicians to overcome disagreements arising. Tangible advantages of NEWS2 were seen in recognising a response to treatment, a need for transfer to ward or ICU or just an impression of the patient’s status. Nonetheless, it is deemed ‘overvalued’ by some nurses, and others anticipated the need for iteration due to its failure in some settings like cardiology and general surgery; creating a culture of hesitance to adopt. Senior staff perceive its usefulness for junior doctors and nurses yet believe it poses the risk of over-reliance in using a tool that may not be reliable for each condition. It can restrict their critical thinking due to their lack of experience. They perceive it as an optional mean in the escalation process yet not dependable.
It allows us to catch things before we have to send a patient elsewhere. (Sm)
Historically, sometimes nurses will argue if the patient is sicker or not; NEWS2 frames this with a nationally recognised number. (Gm)
I used to see patients that were unwell, that didn’t trigger NEWS. Junior nurses worry about what the audit says, they can be completely fixated on a NEWS2 and not the patient holistically. Over-reliance becomes a danger. (Gm)
In escalation of care, it provided clarity. When, where and whom to escalate to is coherent to everyone, potentially saving time and promoting safety. Yet, nurses from both sites reported that the impact of NEWS2 in the escalation is insignificant to make a noticeable difference.
This is very clear cut in terms of NEWS2. (Gm)
I don’t think it’s made that much of a difference. (Gs)
In the time of the pandemic, there was an agreement by most staff that no advantage observed is credited to implementing NEWS2 in clinical work or patients’ outcomes. Nurses and doctors are more vigilant to deterioration due to international and organisational recommendations to manage and prevent COVID-19. Teams, that is, medical, infection control and CCOT, were present, facilitating the escalation of care. An advantage reported was specific attention to temperature scores in NEWS2 to alert any suspected COVID-19 case.
I don’t think it had much of a value in the pandemic. We had a medical team on our Ward all the time, which we weren’t used to, and of course, we had a good response. (2S)
Digitalisation: EHR integration and automation
NEWS2 in EHRs is perceived to have several advantages, with some unpleasing downsides. Accuracy of calculation and timely scoring were reported once entered in patients’ charts. This facilitates decisions for treatment or escalation, and the ability to audit documentation. On the other hand, it has been perceived to inhibit junior nurses and doctors’ thought processes when they rely on the system to produce a score without examining its parameters. Some nurses expressed a preference for the paper chart version of NEWS2 over the electronic one due to the absence of colour coding, inability to adjust thresholds, omission of score trend and constant alarm pop-ups. More dissatisfaction with the model in EHRs was expressed by general hospital staff than specialist hospital, who agreed more to it. Personal differences like age and IT literacy cause a restrain to some nurses to adopt digital documentation.
We can deep dive in the documentation to make sure that everyone is doing what they need to do. (Sm)
There are benefits of an electronic system, but it doesn't allow nurses and doctors at a junior level to think about their thought processes. (Gm)
I did use to like the graphs that we used to get in the paper version, to be able to see what the acuity trend is like for patients and across the floor. (Gs)
With automated monitoring in the specialist hospital, the accuracy of recording and timely data transfer is reliable. Nurses are more aware of the need to accomplish this task when it is automated; not appearing on the screen means undone, while previously it could indicate late entry. Nonetheless, timely observations may not lead to timely escalation. Nurses do not carry computers or handheld devices all the time. Therefore, escalating a case is subjected to completing the documentation on the workstation, which may be by the end of assessing a number of patients.
it’s accurate and timely; the moment you open the screen, it will flash to remind you to act. (Gm)
They’ll do a whole lot of patients, six to ten and then come back and escalate it at the end. (Sm)
Understanding the information behind NEWS2 and generated by it was straightforward to most participants. Nurses who considered it unideal expressed the need to learn the rationale behind each parameter scoring and confusion related to triggering at the patients’ baseline. Nonetheless, the NEWS2 score and parameter value is perceived to be unrealistic. Constant unnecessary alarms are disadvantages reported by nurses working in cardiology and oncology wards in both sites, while not alarming when assessment indicates the need to escalate. Nurses, who are the primary assessors for NEWS2, are not authorised to adjust the scale, causing annoyance and avoidable alarms when done by doctors.
I think there’s a lot of unnecessary pop-up boxes. (Sm)
Sometimes, the patient might not be newsing. But you just know and feel something changed. And often, we’re quite right with that. (Gm)
Discussion
Our study in the general and specialist settings examined the facilitators, challenges and value of implementing EHR-integrated EWS guided by the NASSS framework. We have explored nurses’ views in a unique time of the pandemic. The framework’s domains have intersected in the themes leading to three findings identified. The implementation support by hospital decision makers was appreciated, yet, determined challenges, like clinicians’ behaviours, IT literacy, lack of resources and training and the perception of NEWS2 value, can forbid the success of this implementation. Second, the impact of the pandemic on clinical practice and training has resulted in uncontrollable changes and enforcing guidelines that lead to undervaluing NEWS2. Lastly, EHR integration and automated monitoring are strong mediums for improvement that are not fully or precisely employed yet. There was an agreement from both sites on the facilitators and barriers, with preference from the specialist setting of the EHR integration and employing dashboards to improve escalation. The challenges found were cultural and setting related or digital system related, as manifested by participants’ views from both hospitals.
The challenge of seniority-related behaviour can be daunting to junior nurses and doctors who suppress their development in the work setting. Junior clinicians are the most receptive to change in the health system, and their ability to learn is high, a wasted advantage if discouraged. In previous EWS implementation, the seniority level of qualified nurses can affect the response of medical staff to review a patient or not.32
Increasing the safe space to express clinical concerns by junior staff is a major need to be addressed to improve the work culture in hospital settings.
The perception of NEWS2 as a unified EWS for patients with complex conditions is appreciated for patients’ safety and eliminating clinical judgement disagreement, yet insufficiently valued. They doubt their decision to escalate or have a dismissive culture to high NEWS2 score, majorly in the cardiology settings, owing to their clinical knowledge of patients’ baseline and history. Applying an EWS system for critically ill patients can either be a confidence booster if perceived as reliable,25 or a source of tension between their own trusted knowledge and experience and nationally enforced guidelines.33 To date, there is insufficient evidence on the validity of NEWS2 in specialised subgroups, including cardiology and oncology settings9; therefore, the call for unified NEWS2 remains weak. However, clinicians’ belief towards applying NEWS2 to avoid further risk to patients’ safety is valid.
Inadequate resources and training are challenges to implementing EWS that were heightened during the pandemic. Various medical devices are in shortage globally34 35 and missed training opportunities created a gap in professional development, negatively impacting clinicians’ confidence.36 37 The surge in hospitalisation and escalation to ICU due to the COVID-19 pandemic necessitate the enforcement of national and international frameworks as a well emergency response to overcome the crisis.35 38 39 That came ahead of implementing a national EWS developed for ward patients when hospitals were more stable functionally. Greater attention was paid to all patients during the pandemic with the presence of various medical teams, facilitating critical care regardless of NEWS2 score.
The documentation non-adherence presented a cultural issue in both hospitals, with more non-compliance and the need for auditing expressed in the specialist setting. Embedding NEWS2 in EHRs and automated monitoring can be robust solutions representing the role of digitalisation in improving documentation, clinical tasks and patient outcomes. There is inadequate evidence on the benefit of EHR integration in previous studies. Our study indicates the advantage of accuracy and timeliness of scoring and alarming NEWS2, prompting decision-making and early intervention and potentially decreasing workload. Automated monitoring has motivated staff to complete documentation since what is seen is done.19 However, digital system challenges, including insufficient workstations, IT assessment and training40 41 and overlooking the positive aspects of paper workflow, cause transformation to be hindered. Therefore, it is essential to address the obstacles to implementing EWS in EHRs and work towards overcoming them by supporting the implementation from the human and the system perspective.
Strengths and limitations
The study examined the implementation in two different sites in structure, policies, specialty and care pathways.
The NASSS framework was used as a guide, a solid theoretical foundation that analyses the complexity of implementing health technology solutions.
We conducted the interviews and surveys at the time of the pandemic in England, which provided enhanced rapport and a rich narrative.
The sample is limited by purposive sampling and the pandemic pressure, which might have restricted further participation in the study.
The findings are correlated with the pandemic impact on the workflow and perceptions. Postpandemic implementation studies are required.
The interviews were guided by the domains and may have missed some richness of human-centric topics that could be explored deeply, that is, seniority behaviours and EHR users’ preferences.
The findings might apply to hospital settings with similar structures and EHR systems; in other hospitals with different patient record systems or lacking digital integration, the findings may not be generalisable.
Conclusion
The significance of NEWS2 can be underestimated when challenges are overlooked, and evidence of its validation is not apparent. NEWS2 was appreciated partially by some nurses and managers; however, it was not sufficiently strong in specialised care like cardiology to empower the adoption. Clinicians’ behaviour in escalation from a cultural perspective, IT literacy and resources from digitalisation perspective impact the implementation. COVID-19-related regulations and guidelines influence clinicians’ practice more than implementing EWS and digital solutions. Implementing new EWS and digital solutions may be less complicated prior to the pandemic. However, more evidence is needed. Studying the validity of NEWS2 in specialised settings and complex conditions is required to guide the implementation. EHR integration and automation are dynamic tools to facilitate NEWS2 utilisation if the principles of NEWS2 are reviewed and rectified, and resources and training are accessible. There is a need to explore the implementation further from human-centric, cultural and digital transformation domains.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and is registered and approved by the Health Research Authority (HRA) and Health and Care Research Wales (HCRW) and sponsored by the University College London (UCL) (REC reference: 20/PR/0286). Participants gave informed consent to participate in the study before taking part.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @baneenalhmoud?lang=en
Contributors BA, AB and TB conceived the study. BA carried out the interviews and surveys with guidance from TB, DM and LH. Data analysis was conducted by BA with guidance from AB. BA wrote the initial draft of the manuscript. All authors contributed to the interpretation of findings and revision to the manuscript. AB is guarantor for the work.
Funding BA has received PhD funding from the Saudi Arabian Cultural Bureau (grant number: ELP003964).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.