Article Text

Abstract
Introduction Soreness is a common complaint in patients who receive lumbar spine surgery (LSS) for degenerative lumbar spine diseases (DLSD). However, soreness is not assessed independently and its impacts on outcomes of LSS remains largely unknown. Sng(pronounced sә-ng, 痠) in Chinese language is the word with the closest meaning to soreness, and Chinese-speaking people naturally use sng to describe their non-pain ‘soreness’ symptom. This study was aimed to investigate the prevalence and impacts of soreness or sng on outcome of LSS by introducing Visual Analogue Scale (VAS) of sng on back and leg.
Materials and methods This prospective cohort study recruited patients who receive LSS for DLSD. Participants completed the patient-reported outcome measures at 1 week before and 1 years after LSS. The patient-reported outcome measures included (1) VAS for back pain, leg pain, back sng and leg sng, (2) Oswestry Disability Index (ODI) and (3) RAND 36-item Short Form Health Survey. The minimal clinical important difference (MCID) of ODI and physical component health-related quality of life (HRQoL) was used.
Results A total of 258 consecutive patients were included and 50 dropped out at follow-up. Preoperatively, the prevalence of sng was comparable to pain both on back and leg; postoperatively, the prevalence of sng was higher than pain. Leg and back sng were associated with preoperative and postoperative mental HRQoL, respectively. The reduction of sng on back and leg were significantly less than pain postoperatively. Leg sng was the only symptom independently associated with attaining MCID.
Conclusion Soreness or sng should be assessed independently from pain in patients receiving LSS for DLSD because soreness or sng had substantial clinical impacts on the outcome of LSS.
- Pain
- Patient-centred care
- Patient satisfaction
- Surgery
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Soreness or sng is a common complaint but it is not assessed independently from pain and its impacts remains largely unknown.
WHAT THIS STUDY ADDS
Soreness or sng has differential impacts from pain.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Soreness or sng is worthy to be assessed independently in clinical practice or clinical trials.
Introduction
Soreness is one of major complaints in patients with chronic pain.1–5 Cumulative evidence has suggested that it is a unique symptom differing from pain in patients with chronic widespread pain.1–3 Behaviourally, soreness (eg, delayed-onset muscle soreness) would evoke a motivation to massage or stretch the affected site, whereas pain (eg, tissue injury) induces avoiding or guarding behaviours.6–10 Also, soreness is a different sensory quality from pain during dry needling and a therapeutic sign called deqi in acupuncture analgesia.11 12 Recently, soreness was shown to have discriminative metabolic and proteomic characteristics as compared with pain in patients with fibromyalgia.13 Chronic pain associated with degenerative lumbar spine diseases (DLSD) substantially impair quality of life and lumbar spine surgery (LSS) is usually the last resort when other conservative treatments fail. By using Visual Analogue Scale (VAS) of soreness, we first showed soreness of back and leg is a common complaint in patients who receive LSS for DLSD.4 However, the clinical impacts and the incidence of soreness and its treatment response to LSS is still obscure.
The word ‘soreness’ in English describes the quality of being painful because of injury or too much use. To avoid confusion and to facilitate scientific research and clinical practice, we proposed a new term, sng (pronounced sә-ng), to replace ‘soreness’ to differentiate it from pain perception.14 Sng is the Romanisation form of ‘soreness’ in Taiwanese (Southern Min) to describe the perception of acid sensation that occurs in fatiguing exercise, musculoskeletal disorders, influenza, vaccination, physical therapy, acupuncture, etc.14 Besides, sng (痠) in Chinese language is the word with the closest meaning to soreness, and Chinese-speaking people naturally use sng to describe their non-pain ‘soreness’ symptom. Accordingly, it is more practical and effective in using sng for communications with Chinese-speaking patients. Here, we introduced VAS of sng in this study to investigate its incidence and impacts on the outcomes of LSS. The aims of the current study were to (1) investigate the prevalence of pain and sng, (2) determine whether sng, independent of pain, has a unique and significant clinical impact before and after LSS on health-related quality of life (HRQoL) and (3) examine whether sng was a significant risk factor for the treatment response of LSS.
Methods
Design and participants
This was a longitudinal study including patients scheduled for lumber spine surgery by convenience sampling at two hospitals in northern Taiwan from June 2016 to March 2019. Participants were enrolled according to the following criteria: (1) aged 20 years and above, (2) had low back pain (LBP) over 3 months co-occurring with intermittent claudication or perceived pain in one or both lower limbs at sites that are consistent with the area innervated by the L4, L5 or S1 nerve roots, or other sensory symptoms in the affected areas (typically, the pain may be perceived in the buttock, thigh, calf, leg, foot or toes), (3) yielded degenerative lumbar spine pathology corresponding to their symptoms on images and (4) were able to communicate using Chinese Mandarin and complete all assessments.
Participants were excluded if they had neuropathic pain due to causes other than degenerative disease of the vertebrae in the lumbosacral spine or associated soft tissue, the history of major psychiatric diseases, cancers, or substance abuse before the study, or other surgical interventions in addition to lumbar surgery during the study period.
Measurement of pros
A VAS was used to quantify the intensity of back pain, leg pain, back sng and leg sng. The VAS is a 0–10 horizontal line with 0 indicating no pain and 10 reflecting severe pain (worst imaginable pain). Participants were required to mark the horizontal line to reflect their appropriate pain or sng perceptions during movement in the past month. Before commencing the study, we selected 50 participants who received pain medication on the first postoperative day after LSS to assess the responsiveness of the four VAS measurements to pain medication. Reliability is a critical component of responsiveness.15 16 The VAS scores for back pain, leg pain, back sng and leg sng sensitively detected changes in pain and sng over time and in response to pain medications among our participants (the ranges of Cohens d from −0.3 to −1.1 for pain and from −0.3 to −0.9 for sng, online supplemental table 1). In the current study, we used a VAS score ≥3.5 as cut-off for determining significant (moderate) chronic pain or sng.17
Supplemental material
HRQoL was adopted as the indicator of clinical outcomes of this study, which was assessed using the RAND 36-item Short Form Health Survey (RAND-36).18 It is a multidimensional measurement tool that includes 36 items summarised in two measures related to physical and mental health components. Four domains—physical function, physical role, bodily pain and general health—were included in the physical component summary (PCS). The mental component summary (MCS) is represented by emotional role, social function, mental health and vitality domains. The RAND-36 approach is based on the concept that physical and mental health components are related when diseases may simultaneously affect both states. Each scale ranges from 0 (worst health state) to 100 (best health state), a higher score reflecting better HRQoL. The RAND-36 has excellent measurement properties.18 19
The minimal clinically important difference (MCID) was used to measure treatment response following lumbar spinal surgery. It was determined by calculating the change in scores of the RAND-36 PCS (cut-off=4.9) or Oswestry Disability Index (ODI) (cut-off=12.8) between the 1-year follow-up and baseline.20 Patients with achievement of the MCID were considered to have attained the MCID of the PCS or ODI; otherwise they did not achieve the MCID. The ODI contains 10 items for measuring disability severity related to LBP. Each item is scored from 0 to 4 on a five-point ordinal scale, with 0 indicating no limitation and 4 extreme limitation or an inability to function.21 The Chinese version of the ODI has excellent internal consistency (Cronbach’s alpha=0.903), test–retest reliability (intraclass correlation coefficient=0.89) and convergent validity with the Medical Outcomes Study 36-item Short Form physical functioning subscale (r=0.75).22
Covariate measures
A predesigned information sheet was used to collect demographic and disease characteristics, including age, sex, body mass index (BMI), modified Charlson Comorbidity Index (mCCI), duration of symptoms, use of analgesics and the ODI. The mCCI contains 11 conditions, including cerebrovascular disease, chronic pulmonary disease, congestive heart failure, myocardial infarction, peripheral vascular disease, diabetes, hemiplegia, renal disease, liver disease, age and disseminated cancer. A score of 1, 2, 3 or 6 was assigned to each condition according to the risk of death related to each condition. A total score is calculated by summing the number of morbidities.23 The ODI contains 10 items for measuring disability severity related to LBP. Each item is scored from 0 to 4, using a five-level ordinal scale, with 0 indicating no limitation and 4 reflecting extreme limitation or an inability to function.21 Excellent reliability and validity have been demonstrated.22
Procedures
All participants who met the inclusion criteria were informed of the study purpose and procedures. Once written informed consent was obtained, two trained research assistants asked participants to complete a battery of self-reporting questionnaires including the information sheet, the VASs for back pain, leg pain, back sng and leg sng, ODI, and RAND-36 at 1 week before surgery. Trained research coordinator who is independent of surgeons contacted participants to complete the same questionnaires 1 year after surgery in person or over the phone (online supplemental figure 1).
Statistical analysis
Results are presented as proportions for categorical variables and means (SD) for continuous variables. Descriptive analyses and frequency distributions were used to analyse the distribution of demographic and disease characteristics. The McNemar test was used to compare the changes in prevalence rates of pain and soreness/sng before and after surgery. Repeated measures analysis of variance was used to examine changes in preoperative and postoperative scores in sng and pain as well as HRQoL after adjusting for potential confounding factors (ie, age, BMI, mCCI, male sex, duration of symptoms, ODI score, analgesic use, preoperative PCS/MCS, spondylolisthesis disc herniation and spondylotic stenosis). A multivariate linear regression model was used to explore the association of pain and sng with HRQoL in physical and mental health. The variance-inflation factor (VIF) was used to assess multicollinearity in regression analysis and the value <10 indicates the interdependence of predicting variables. logistic regression model was used to examine the association of patient characteristics and symptom VAS score with MCID achievement. All statistical analyses involved by using SPSS V.22.0 for Windows, and significance was set at p<0.05.
Patient and public involvement
The research question of sng and sng VAS as an outcome measurement was developed because many patients receiving LSS for DLSD complained it. No patient was involved in study design, recruitment or conduction of this study.
Results
Patient characteristics
We enrolled 258 consecutive patients received LSS for DLSD; 50 dropped out at the follow-up (response rate: 80.6%). Reasons for withdrawal included tight schedule and receipt of other surgical interventions during the study period. No significant difference was identified in terms of demographic and disease characteristics between remaining and withdrawing participants. The mean age of participants was 61.5 (SD 13.3) years, and approximately half were male. Other details of demographic and disease characteristics are summarised in table 1.
Baseline demographic and disease characteristics among participants (n=258)
Changes in pain and sng before and after surgery
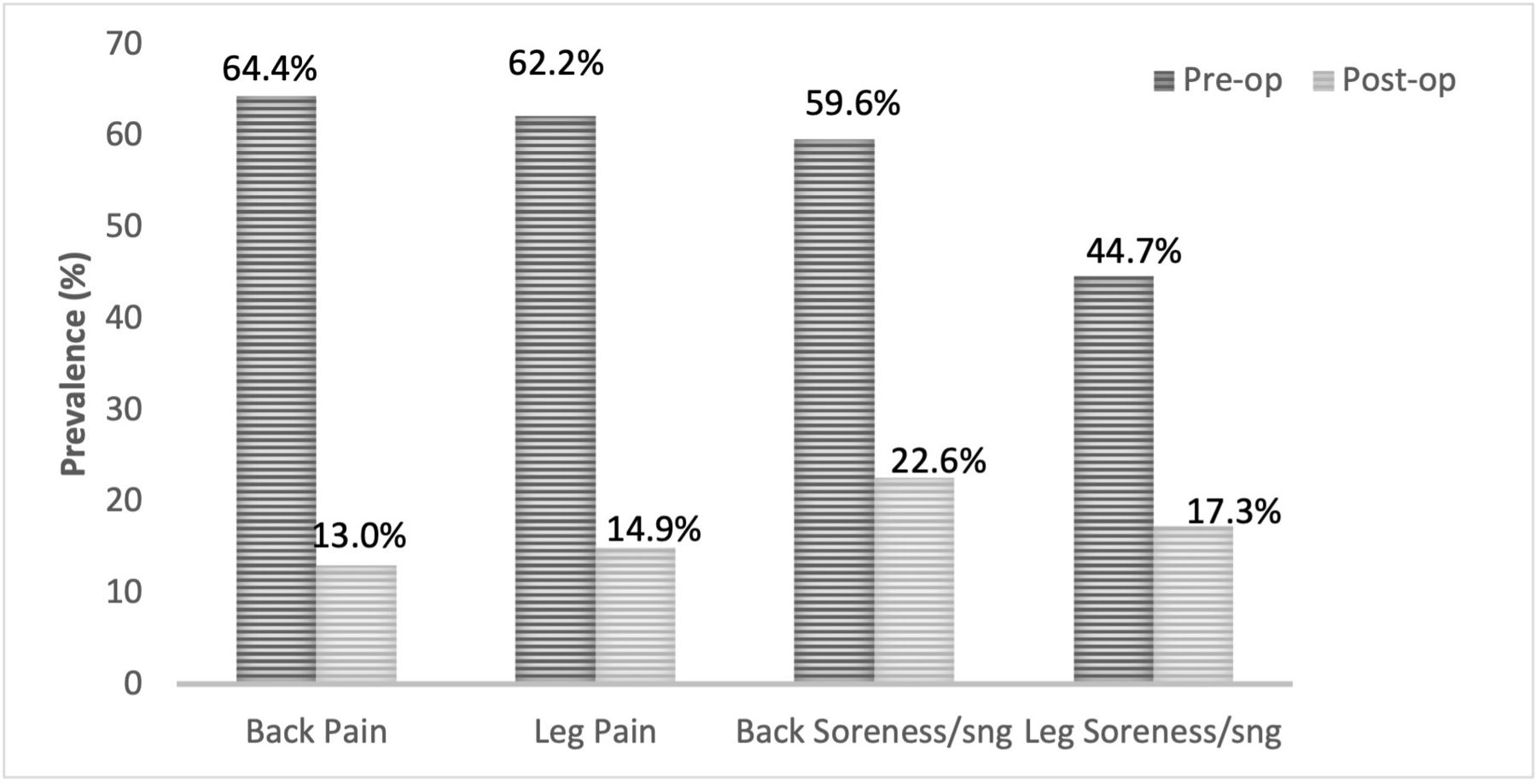
The prevalence of pain and sng at 1 week before and 1 year after surgery is presented in figure 1. Before LSS, the prevalence of back pain, leg pain, back sng and leg sng was 64.4%, 62.2%, 59.6% and 44.7%, respectively; at the follow-up, the prevalence for back pain, leg pain, back sng and leg sng 13.0%, 14.9%, 22.6% and 17.3%, respectively. The VAS scores for preoperative and postoperative pain and sng are in online supplemental figure 2. Before surgery, back pain, leg pain and back sng, but not leg sng, were on average moderate; after surgery all scores indicated mild symptoms, indicating that leg sng seems in the mild category before and after surgery. As compared with preoperative scores, mean postoperative pain and sng scores were significantly reduced (all p<0.001). The reduction in scores after surgery was significantly greater for pain than sng for both the back and leg (both p<0.001, figure 2).

Prevalence rates of back pain, leg pain, back sng and leg sng before and 1 year after surgery.

{kind=link}
{kind=link}
Change in mean visual analogue scale scores (preoperative–postoperative scores) regarding pain and sng according to back and leg. Data are mean (SD). The significance of changes in symptoms was analysed by repeated measures ANOVA adjusted for age, sex, ODI scores, mCCI, analgesic use and years of low back pain. ANOVA, analysis of variance; mCCI, modified Charlson Comorbidity Index; ODI, Oswestry Disability Index.
Clinical impact of pain and sng associated with HRQoL
The physical and mental component means of HRQoL scores are presented in online supplemental figure 3. A further analysis revealed that physical but not mental HRQoL was significantly improved (p<0.001). Table 2 presents the association of pain and sng with HRQoL before LSS. The results of VIF were acceptable, suggesting that there was no problem of multicollinearity in regression analysis due to interdependence of variables. After controlling for possible confounders, back pain was significantly associated with physical HRQoL (B=−0.35, p=0.02), so participants who had pain experienced poorer physical HRQoL. Notably, leg sng was negatively associated with mental HRQoL after adjustment for confounders (B=−0.64, p<0.003), so participants who complained of leg sng experienced poorer mental HRQoL.
Prediction model of preoperative pain and sng on physical and mental health-related quality of life (n=208)
Table 3 shows the association of pain and sng with HRQoL after LSS. After controlling for possible confounders, neither pain nor sng was associated with physical HRQoL. Notably, back sng was negatively associated with mental HRQoL after adjustment for confounders (B=−0.67, p=0.04), so participants who complained of back sng experienced poorer mental HRQoL.
Prediction model of postoperative pain and sng on physical and mental health-related quality of life (n=208)
Treatment responses following LSS
The univariate analysis for MCID achievement is presented in table 4. Age, mCCI, postoperative leg sng, back pain and leg pain were identified as potential confounders (all p<0.05) and sequentially entered a multivariate logistic regression model for MCID achievement. Leg sng was the only symptom independently associated with MCID achievement after adjustment for confounders (OR=0.75, 95% CI 0.64 to 0.86, p=0.007).
Univariate and multivariate analyses of associations between patient characteristics and minimal clinically important difference
Discussion
By introducing the VAS to evaluate the symptoms of sng, we revealed sng as a complaint as frequent as pain in Chinese-speaking patients who receive LSS for DLSD. Preoperatively, leg sng affected mental HRQoL, whereas back pain affected physical HRQoL. Postoperatively, only back sng affected mental HRQoL. In addition, after LSS, the reduction in VAS score was significantly lower for sng than pain. Leg sng was the only symptom associated with achievement of the MCID after LSS. Sng had unique clinical impacts and a different response to LSS than pain and thus should be assessed independently when surgically treating DLSD.
In this study, we identified soreness or sng as an important symptom with differential clinical impacts from pain in patients with DLSD. Pain is well known to affect physical aspects of the quality of life,24–27 whereas we found that sng selectively impaired the mental HRQoL of patients with DLSD. This result is consistent with a previous study of Chinese female migrant workers showing muscle soreness or sng associated with all seven domains of the RAND-36 except for physical functioning.28 In addition, two previous studies demonstrated that soreness or sng (eg, muscle soreness or post-needling soreness) was also associated with psychological factors (anxiety or catastrophising thinking) in situations of traumatic brain injury, myofascial pain and dry needling treatment.29 30 Chronic mental stress moderated the perceived soreness after muscle resistance training.31 Knowing the specific impact of soreness or sng on mental health, one should pay attention to and take care of patients’ complaints of soreness or sng.
Our study points out that assessment of soreness or sng is an unmet medical need in patients who receive LSS for DLSD. Patient-reported outcomes (PROs) are the standard measure to evaluate the outcomes of spine surgery.20 VAS of pain on back and leg, ODI, and HRQoL serve as important PROs in many studies of LSS.20 However, sng as a common complaint in Chinese -speaking patients3 32 33 is not included in current PROs for LSS. In the clinical studies of LSS or many clinical trials for DLSD, the VAS for pain is the only measurement used for symptom severity. Pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage by the International Association of Pain.9 34 According to this definition, soreness or sng as an unpleasant sensory experience should be under the category of ‘pain’. However, the supplementary explanation also states that ‘unpleasant abnormal experiences may also be pain but are not necessarily so because, subjectively, they may not have the usual sensory qualities of pain’.9 34 This study reminded that ‘pain or discomfort’ is a complex of subjective perceptions to a person with pain and soreness or sng as a unique symptom distinct from pain should be included in the toolbox of pain evaluation. Pain should not be the only measurement in clinical trial or studies of spine surgery.
The differential clinical impact and response to treatment of sng we have shown suggests that sng is a distinct symptom from pain in the perspective of sensory quality. The sensory quality of symptoms reflects the underlying pathophysiological mechanisms.35–37 For example, some distinct sensory quality of symptoms (numbness, tingly feeling, ‘pins and needles’, stinging, and electrical feeling) was used to identify a neuropathic origin.35 Following this concept, more effective treatment based on the mechanism could be developed and treatment could be individualised according to the various sensory quality of symptoms.38 The underlying pathophysiological mechanism of sng is largely unkown. We proposed the term ‘sngception’ (sng-ception) to represent the specific somatosensory function to sense tissue acidosis and transmit the acid sensation from the peripheral to central nervous system .14 A clinical trial is needed to prove the causal effect of tissue acidosis and sng perception, although previous studies have shown that intramuscular acidification causes pain in English-speaking healthy volunteers.39
Limitations and generalisability: The term ‘sng’ is commonly used by Chinese-speaking patients, whose equivalent has not been found in other languages. Should clinicians in other countries wish to introduce the term when evaluating similar pain-related outcomes, they may adopt the term ‘sng’ since it is useful to fill the void. Alternatively, they could also use the equivalent in their respective language, should such linguistic expression is available. The study included only participants in two hospitals of North Taiwan, which limits the generalisability of the results. Also, we used different approaches to collect data—face-to-face and telephone interviews—which may affect participants’ responses to the measurements. Last, although leg sng was the only symptom independently associated with achieving a minimal clinically important difference, an OR of 0.75 is less than a small effect size suggestion (1.68),40 indicating leg sng had very small effect size in interpretation of minimal clinically important difference. Future studies are warranted to verify our findings.
Conclusions
Sng or soreness is a common complaint in patients who receive LSS for DLSD. Leg sng and back sng are associated with mental HRQoL preoperatively and postoperatively, respectively. Sng can be significantly reduced after LSS but to a lesser extent than pain. Leg sng is the only symptom associated with achievement of the MCID. Considering that sng has unique clinical impacts and a different response to LSS from pain, soreness or sng should be assessed independently to pain.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Joint Research Ethics Review Boards at the participating hospitals (N201602059 and N201612086). This study was conducted in accordance with the Declaration of Helsinki.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it first published. Author name 'Hsiao-Yen Chiu' is changed to 'Hsiao-Yean Chiu'.
Contributors JHL and C-CC did the study design. JHL and YCC collected the data. HYC did the statistical analyses. JHL, HYC and CCC wrote the manuscript. I-WS provided her expertise in linguistics in response to reviewers. CCC and YWY provided administrative support. JHL is responsible for the overall content as the guarantor.
Funding This work was supported by intramural funding of Academia Sinica and grants from the Ministry of Science and Technology, Taiwan and Taipei Medical University and Taipei Medical University Hospital (MOST106-2321-B-001-044, MOST107-2321-B-001-020, MOST 108-2321-B-001-005, MOST 108-2321-B-001-028-MY2, MOST110-2321-B-001-010, MOST111-2321-B-001-009, 108TMU-TMUH-08).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.