Article Text

Abstract
Background At 10%, Karamoja region has the highest rate of child wasting in Uganda. The region has 126 outpatient therapeutic care (OTC) sites for managing children with severe acute malnutrition.
Local problem Cure rate (CR) in OTC in Karamoja remains below the international standard of over 75%. The study aimed at increasing the CR in 10 OTC sites in Karamoja, from 74.1% to >75% in 13 months.
Methods The study commenced in July 2018, up to September 2019, in purposively selected health facilities in six districts in Karamoja. Quality improvement (QI) methods per the Ministry of Health QI Framework were applied. QI teams (QITs) tracked the outcome of the tested changes for 13 months. χ2 tests were used to assess the intrafacility and interdistrict association in CR.
Intervention Institute for Health Improvement (IHI) (2003) improvement model was applied in this collaborative. QITs conducted root cause analysis of CR gaps, which guided them in the development of improvement aims, changes and indicators. QITs used plan–do–study–act cycles to test and adopt the feasible changes.
Results CR increased from 74.1% to 78.6%, with an overall average of 80% within 13 months. Abim district had the highest CR (83.3%) and Kaabong district the lowest (75.2%). Health centre II (84.0%) had the highest CR. Assigning village health teams to follow up caregivers of children in OTC with missed appointments, allocation of village health teams and local leaders to monitor the administration of ready-to-use therapeutic food to children, and screening and treating comorbidities among children in OTC increased CR.
Conclusions QI methods focusing on collaborative learning increased CR among children in OTC in Karamoja. Sustaining the gains requires district health offices, partners and health facility management’s commitment to institutionalise the QI collaborative learning approaches.
- community health services
- health behavior
- PDSA
- quality improvement
- collaborative, breakthrough groups
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
No research on the use of quality improvement (QI) collaborative learning approaches for increasing cure rate (CR) among children with severe wasting managed in outpatient therapeutic care (OTC) programmes in Karamoja, Uganda.
WHAT THIS STUDY ADDS
QI collaborative learning approaches increased CR by 4.5 percentage points between July 2018 (74.1%) and August 2019 (78.6%). Thus, QI collaborative learning can potentially improve OTC programmes’ performance beyond the standard CR of >75% in Karamoja, Uganda.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
A strengthened partnership between the district health and community-based services departments is necessary to institutionalise the gains made from the QI collaborative learning approach. Additional research is needed to ascertain the extent to which the achieved performance is sustained by the local government and health facilities beyond the project approach applied in this study.
Problem
Despite the persistent low cure rate (CR) below the Sphere humanitarian standard of >75%, there is no research on the use of collaborative QI approaches for increasing CR among children with severe acute malnutrition (SAM)/wasting managed in OTC programmes in Karamoja subregion, Uganda. The study aimed at applying QI principles to improve CR among children with severe wasting in 10 OTC sites in Karamoja region from 74.1% to >75% in 13 months.
UNICEF Uganda implemented the study in collaboration with Doctors with Africa (CUAMM), Moroto Regional Referral Hospital (RRH) and the selected district local governments. UNICEF Uganda supports the Ministry of Health (MOH) through Moroto RRH, district health offices (DHOs) and health facilities to plan, implement and monitor OTC.1 UNICEF Uganda ran this project as part of its Karamoja Nutrition Programme in 2018, which aimed at strengthening health systems for nutrition service delivery in the region.
UNICEF Uganda is a United Nations agency mandated by the United Nations General Assembly to advocate for the protection of children’s rights, to help meet their basic needs, and to expand their opportunities to reach their full potential. In Uganda, UNICEF began its operations in the early 1960s. UNICEF supports national efforts to accelerate the realisation of children’s rights and progress towards achieving the Sustainable Development Goals for children in line with the Government of Uganda’s Vision 2040. UNICEF’s current programme focuses on education, child protection, social protection, health, nutrition, and water, sanitation, and hygiene. While working at national scale, UNICEF uses a focus-district approach that targets those districts with the highest prevalence of child deprivation, including refugee movements, disease outbreaks and climate-related impact. This programme is delivered through over 100 technical specialists at national and district level.
Background
Globally, 47 million of children under 5 had wasting in 2019, with 14.3 million severely wasted. The majority of children with wasting are found in Asia and Africa.2 Global severe wasting has reduced by only 11% over the past 20 years.3 In Uganda, 280 000 and 86 743 of children under 5 are wasted and severely wasted, respectively.4 West Nile and Karamoja regions have the highest prevalence at 10.6% and 10%, respectively.4 Wasting in Karamoja increased from 7.1% in 2011 to 10% in 2016, with severe wasting doubling to 3.0% in the same period.4
SAM is defined as weight-for-height/weight-for-length Z-score of <−3SD of the WHO’s Child growth standard, or an absolute mid-upper-arm circumference of <11.5 cm, or the presence of bilateral nutritional oedema.5 6 Children with SAM are nearly 12 times more likely to die than their healthy counterparts.7 Timely identification and initiation of treatment of all severely wasted children to care is needed to prevent complications and death.8
Programmes for treating children with SAM have been implemented in Karamoja for decades. Uganda’s Integrated Management of Acute Malnutrition (IMAM) guidelines provide an outpatient therapeutic care (OTC) programme for treating severe wasting without medical complications.9 OTC brings the services for the management of SAM closer to the community using ready-to-use therapeutic food (RUTF), community outreach and mobilisation. Besides RUTF, severely malnourished children are given routine medications such as deworming tablets, antibiotics and measles vaccine.10 In 2018, about 27% of children with SAM were enrolled in feeding programmes in Karamoja, with 15% receiving services from OTC.11
Inadequate intake of nutritious diets, malaria, acute respiratory infection and diarrhoea are the leading causes of wasting among children under 5 in Karamoja.12 The high and recurrent food insecurity, inadequate access to safe sanitation facilities, and low per capita water use worsen the wasting levels among children under 5 in Karamoja.
CR is a proportion of patients successfully discharged as cured during the reporting period, of which discharges include cured, defaulters, deaths and non-respondents. Within Uganda, the CR in OTC is reported to be between 52.9% in Arua and 71.5% in Karamoja,13 14 which is below the Sphere humanitarian standard of 75%.15
Mwanza et al16 reported CR of 80% in OTC in Zambia. In Mozambique, CR among children with wasting managed in the health facilities was 48.2%.13 CR among children managed in OTC in Ethiopia ranges from 61.8% to 79.6%.17–21 Although CR in Karamoja improved in 2013–2016 (71.5%),22 it was below the standard 75%.15 The key drivers for the low CR included severe household food insecurity, walking for more than one hour to receive treatment, diarrhoea comorbidity and sharing of RUTF.20 Children treated in health centres and health posts had a higher recovery rate than in hospitals.20 Children who received routine medication were older, had no comorbidity and had better odds of recovery.3
Rationale
The improvement model developed by IHI (2003)23 was applied in this collaborative. This is a method for quickly testing and implementing evidence-based changes across a group of facilities. It included 2 days’ orientation of the regional and district-based coaches and mentors. The district teams then identified the quality improvement (QI) areas that would yield the improvement in CR of children identified with SAM. The intervention considered a 13-month learning period involving QI Teams (QITs) from 10 high-volume health centres focused on improving CR above the >75% international performance standard. QI principles, methodologies and tools were used per the MOH’s QI framework to identify the root causes of the problem and test and implement feasible changes resulting in increased CR. The QI process for tested changes was guided by the monthly plan–do–study–act (PDSA) cycles.
Following the selection of QI areas during the orientation of the district-based coaches and mentors, the QITs collected baseline data for the period—January to June 2018. The teams collected data on the number of children with SAM managed in OTC discharged as cured, and the total of children with SAM managed in OTC discharged from the participating health facilities. The teams used existing data in the Health Management Information System (HMIS) registers to compute monthly CR for children with SAM managed in OTC.
Design
Study sites
The study took place in high-volume health facilities purposely selected by DHOs in Abim, Amudat, Kaabong, Kotido, Nakapiripirit and Napak in consultation with UNICEF and its implementing partner—Doctors with Africa (CUAMM). This study focuses on only 10 facilities composed of 2 (20.0%) health centre IVs, 7 (70.0%) health centre IIIs and 1(10.0%) health centre II. Table 1 provides the details. Uganda’s health facility setting has the national referral hospital (NRH) as the highest, providing specialist services in addition to other clinical services, followed by the RRH, district general hospital and health centres IV, III and II.24 The health services are structured into NRHs and RRHs, general hospitals, health centre IVs, HC IIIs and HC IIs. The HC I has no physical structure but a team of people (the village health team (VHT), which works as a link between health facilities and the community.
District and facilities that participated in learning collaborative
The intervention
Support to facility-level staff to learn and apply collaborative QI principles
The national and district coaches and mentors, used four approaches to support health facility QITs to use collaborative QI (CQI) methods to improve MNH and Nutrition care per the MOH’s QI Framework and standards.25 The teams adopted the same approaches applied in the Partnership for HIV Free Survival initiative.26 The details are described in the implementation steps subsection.
The regional orientation of district teams in QI approaches
Technical specialists with critical skills and experience in collaborative learning from the NGO CUAMM, UNICEF and MoH conducted a 2-day (19 July 2018–20 July 2018) regional orientation of the district health teams (DHTs), regional and district-based coaches and mentors, health workers and representatives from NGOs (CUAMM, CRS and Mercy Corps).
The orientation aimed at improving the skills and knowledge of regional and district-based coaches and mentors, to build the capacity of sites in applying CQI approaches to improve MNH and Nutrition quality of care. The key topics covered included an introduction to CQI and an overview of 5S (Sort, Set, Shine, Standardise and Sustain), CQI action planning, learning sessions and harvest meetings, collaborative improvement model as well as testing and implementing changes using the PDSA cycle. 5S is a sequence of activities that include Sort, Set, Shine, Standardise and Sustain to improve the working conditions and make them as convenient as possible.25 During the orientation, the capacity-building team introduced coaches and health workers to documentation journals and PDSA tools which they used to document the progress, record data and plot time series charts.
Formation and functionalisation of QITs
Within each selected health facility, district coaches and mentors facilitated the formation or the functionalisation of the QITs for the initiative. The QITs consisted of health facility service providers in the targeted care points such as outpatient department (OPD), antenatal care and maternity. A QIT team was considered functional if they frequently met (at least once a month), with documented evidence of the meetings, and worked on an improvement project. The collaborative improvement approach constituted identification improvement aims, analysing the root causes of the identified problem through brainstorming, ‘five whys’ and ‘fishbone approach’,25 as well as testing small incremental changes to improve clinic processes. The PDSA cycle guided this process.27 The QITs tracked the impact of these changes using existing data in the HMIS—and annexed indicators for OTC that corresponded to the various clinical processes being improved. Sustainability of the intervention hinged on the use of existing healthcare structures and monitoring tools so that institutionalisation was seamless even at the closure of the study.
Strategy
During the initial coaching and mentorship visit, with guidance from coaches and mentors, the QITs, through brainstorming exercises, identified the root causes of low CR among children with SAM admitted to OTC programmes using the 5WHYs approach. The team then developed possible solutions/changes implemented through PDSA cycles. Selected changes were tested for a maximum of 3 months, with data collection done monthly to measure the progress made. During monthly QIT meetings, the teams discussed their performance, documented what changes were implemented, results achieved and identified other possible solutions to improve their projects. The following questions guided the health facility QITs:
What are we trying to accomplish?
How will we know that a change is an improvement?
What changes can we make that will result in improvement?
The overall QI project objective was to increase the CR among children with severe wasting managed in OTC from 74.1% to >75%. The QITs identified three root causes hindering the achievement of CR and developed changes to address them: the caregivers of children under 5 in OTC missed their appointment dates for refilling RUTF due to the long distance to the health facility where OTC is offered, or children falling sick and seeking care in different health centres, the caregivers’ failure to correctly feed children in OTC per the RUTF protocol and the failure of the health workers to timely identify and treat other medical complications among the children in OTC.
After several PDSA cycles implemented by QITs, the following were the common possible solutions/changes that worked across the 10 collaborative sites; assigned VHTs in each village to follow up with caregivers of children in OTC who miss their appointment dates for a refill of RUTF within 5 days; refilled RUTF for 2 weeks for children whose caregivers were termed as ‘mobile communities’; QITs assigned VHTs and local leaders to monitor the administration of RUTF to children with SAM at home; and involved other family supporters and male partners in the care plan for children with SAM.
At the end of the collaborative, the QITs, regional and district coaches and representatives from implementing partners and MoH convened at the regional level for a harvest meeting, where changes that worked across the collaborative sites were consolidated into a ‘change package’ that was used during scale up in other health facilities in the region.
Implementation steps
Training of regional and district coaches
Technical specialists with critical skills and experience in collaborative learning from CUAMM, UNICEF and MoH conducted a 2-day (19 July 2018–20 July 2018) regional orientation of the DHTs, regional and district-based coaches and mentors, health workers and representatives from NGOs (CUAMM, CRS and Mercy Corps).
The orientation aimed at improving the skills and knowledge of regional and district-based coaches and mentors to build the capacity of sites in applying CQI approaches to improve MNH and Nutrition quality of care. The key topics covered included an introduction to CQI and an overview of 5S, CQI action planning, learning sessions and harvest meetings, collaborative improvement model, testing and implementing changes using the PDSA cycle. During the orientation, the capacity-building team introduced coaches and health workers to documentation journals and PDSA tools which they used to document the progress, record data and plot time series charts.
Routine on-site coaching and mentorship
From July 2018 to August 2019, UNICEF facilitated on-site monthly coaching and mentorship sessions in the collaborative sites with support from regional and district-based coaches and mentors. At each monthly coaching visit, QITs, with support from the national/regional and district coaches, reviewed their data and discussed their results and any challenges they experienced. During these meetings, the coaches also shared successful practices from other sites that they supported with their QITs. The coaches supported the QITs in collecting facility data to update their documentation journals. The joint coaching and mentorship teams compiled the monthly coaching and mentorship reports that they shared with the DHO and UNICEF.
Collaborative learning sessions
Throughout the CQI process, UNICEF organised quarterly 2-day collaborative learning sessions through its implementing partners, including CUAMM and Moroto RRH. Two to three health facility QIT members from each collaborative learning site, district, regional/national coaches and partner representatives participated in the sessions. The sessions facilitated peer-to-peer learning and supported the implementation of successful changes among facility QITs. The sessions encouraged QITs to share their results using detailed run charts showing monthly progress toward indicator targets and exchange ideas about how to address challenges. During sessions, QITs reviewed their journals and run charts to identify what was working well and what was not for sharing with the rest of the teams in a plenary presentation. At the end of each session, the teams developed action plans for improving their improvement project performance in the next 3 months.
Harvest meeting
After 1 year of implementation, representatives from the collaborative site teams in Karamoja gathered at a learning and harvest meeting in Moroto on 25 September 2019–26 September 2019. During the session, the representatives discussed successful and unsuccessful changes and related evidence collated and evaluated by teams to identify teams’ ‘best advice’ for new teams, including how-to-guide, for the learning areas of OTC CR and other technical areas. The teams also identified changes the sites had tested to improve OTC CR and developed action plans for the next period. This guided the generation of a knowledge management product called ‘change package’ for the spread phase.
Outcomes of the nutrition collaborative demonstration phase
The regional and district QI coaches were the health workers who had encompassed the QI approach, understood the QI methods, and grasped and understood the programme’s QI activities to the level of having the capacity to train others. Documentation was one of the areas that needed intense work and improvement as this was a weak area, specifically in Integrated Nutrition registers and patient information tools. Teams improved documentation at OTC sites specifically for information on HIV testing and appetite test, RUTF dosage and follow-up counselling on nutrition. Teams improved the provision of RUTF to children with SAM and gave appropriate appointment dates for subsequent visits. Improved CR as one of the primary outcomes was achieved whereby the supported sites had a 4.5% increment. There was an improved follow-up on the caregivers of children in OTC who missed their appointment dates, improved adherence to RUTF and better outcomes for children with severe wasting. The creation of district ownership for the programme enabled members of the DHT or other district-level health workers to capacitate more health workers and monitor the programme. The strong partnership developed under the UNICEF leadership created a forum for discussion during all phases of collaborative improvement implementation.
Data analysis
Data from the collaborative sites were aggregated across the ten health facilities. The numerator, denominator, indicator, the average and the median of the indicator were charted monthly. The CR among children with SAM in OTC was computed by dividing the number of those discharged as cured by all discharges in a month and multiplying it by 100. The data were entered into SPSS version 19, and the descriptive statistics of CR were obtained. CR was categorised into dummy numbers of ‘1’ and ‘0’ for >75% and ≤75%, respectively, for use in binary logistic analysis. Pearson’s χ2 and the Fisher’s exact test were used to assess the association between CR and the districts, health facilities and the year of intervention implementation (2018 and 2019). All the associations were considered statistically significant at a two-tailed p value of less than 5%.
Results
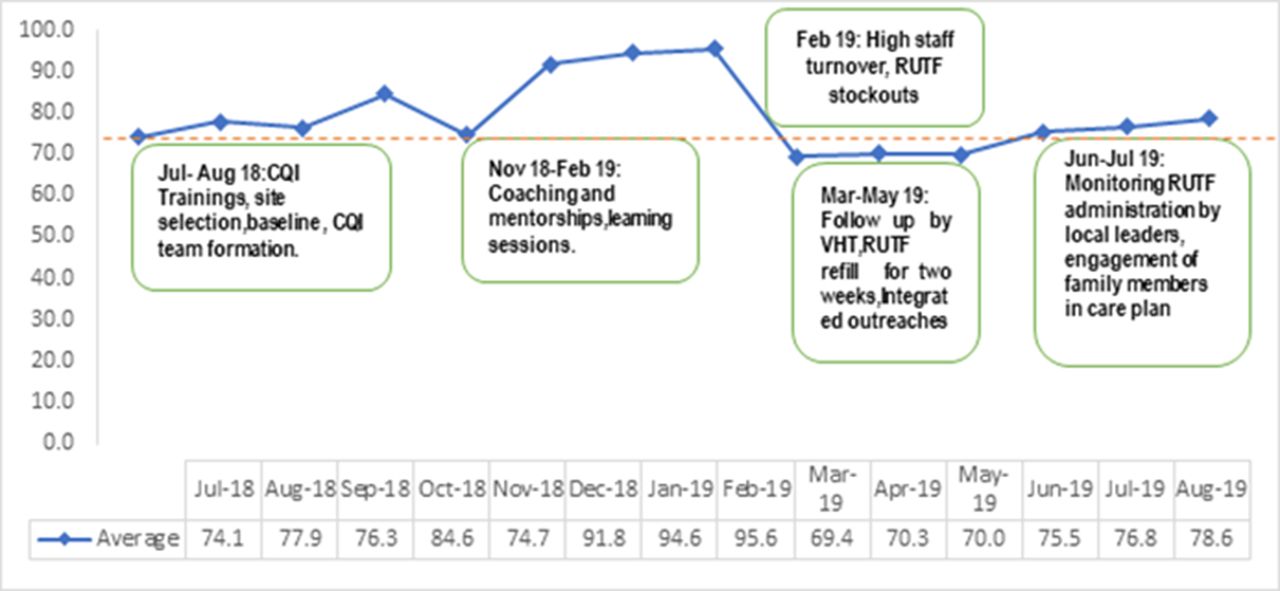
CR among children with severe wasting managed in OTC improved from 74.1% in July 2018 to 78.6% in August 2019. This represents an average CR of 80.0% for all 10 facilities for the 13 months of the project implementation, a 5.9 percentage increase from the baseline value of 74.1%. The performance reached its peak from December 2018 to February 2019. Within the first 3 months of the project implementation, CR increased from 74.1% to 84.6%. This followed a drop to 74.7% and a rapid acceleration to 95.6 % in the next 3 months. Another drop in performance was recorded in March 2019 (69.4%), followed by gradual increments in the next 6 months, peaking at 78.6% in August 2019 (figure 1). The peak performance seems to correspond to the period following the quarterly regional CQI learning sessions, which took place on 30 August 2018–31 August 2018, 19 November 2018–20 November 2018, 20 February 2019–21 February 2019, 22 May 2019–23 May 2019 and 25 September 2019–26 September 2019.
{kind=link}
Average cure rate among children 6–59 months with SAM managed in OTC from July 2018 to August 2019. CQI, collaborative quality improvement; OTC, outpatient therapeutic care; RUTF, ready-to-use therapeutic food; SAM, severe acute malnutrition; VHT, village health team.
Detailed change package for improving the CR in OTC at 10 demonstration facilities in Karamoja region
Table 2 summarises the recommendations from QI teams involved in the demonstration phase of the collaborative sites. The changes yielded the best results for each of the four improvement aims they worked on. Teams provided details on how they implemented the changes for other facilities to replicate the improvement work more readily.
Tested and implemented changes for improving the cure rate in OTC
Performance of the collaborative learning sites and districts in the successful management of children with severe wasting in OTC
At baseline, Amudat had the highest CR (100.0%), and Kaabong had the lowest (50.0%). Health centre II had the highest CR (100.0%) and health centre III had the lowest (60.6%). During the project implementation, Abim had the highest CR (83.3%), and Kaabong had the lowest (75.2%). Health centre II (84.2%) had the highest CR, and health centre III had the lowest (79.1%) (table 3).
Average cure rate by district and health facility level
The findings in table 4 show that 64.3% of the health facilities achieved the standard CR of >75% during the study period (July 2018 to August 2019). Within the health centre II and IIIs, 75.0% and 61.3% had a CR of >75%, while 66.7% of the health centre IVs achieved the standard CR. The χ2 analysis indicated no significant statistical association existed between the standard CR of >75% and the facility level (p=0.652).
Performance of districts and health facilities in 2018 and 2019
Within the districts, 78.1% sites in Napak, 68.0% in Nakapiripirit, 66.7% in Kotido, 66.7% in Abim, 41.7% in Amudat and 38.5% in Kaabong achieved the standard CR. The CR was also not significantly associated within the districts (p<0.096).
Discussion
This is the first joint MNH and Nutrition collaborative learning initiative implemented in 13 months to increase CR among children with SAM managed in ten OTC sites in Karamoja, Uganda. The initiative applied the HCI’s collaborative improvement model, which had not previously been tried out for OTC in Karamoja, an area with high level of severe child wasting. The earlier implemented QI initiatives in Karamoja are limited to nutrition assessment among pregnant women.28 29 Whereas the previous initiatives involved only the health facility health workers and NGO staff in their implementation, the current project actively engaged the central and local government MNH and Nutrition staff as national and district coaches and mentors.
This study has provided evidence that applying QI principles improved the average CR in the ten OTC sites in Karamoja by 4.5 percentage points between July 2018 (74.1%) and August 2019 (78.6%). The overall average of 80.0% achieved in the 13 months of the initiative is higher than the standard CR of >75% by 5%.
The study recorded the highest increase in CR in the first 7 months of the project implementation (August 2018 to February 2019). This could be related to the rapid support the national, regional mentors and coaches provided to the teams and the site teams were still motivated by the observed improvements recorded. The peak performance corresponds to the period shortly after the quarterly regional CQI learning sessions, which took place on August and November 2018, and February, May and September 2019. These learning sessions imparted knowledge, skills and positive attitudes to the CQI teams, who, on return to the collaborative learning sites.
Considering the diversity of factors impeding CR in Karamoja—a semiarid region, the 78.6 percentage increase is a good improvement within a year compared with the previous achievements in the same region. For instance, CR in 2013–2016 improved to 71.5%.22 Compared with the findings by Global Health Liaisons Global Health Liaisons (2016),22 in which 50% of the facilities achieved CR of >75% within 3 years, 64.3% of the 10 facilities in the current project achieved this within 13 months. The collaborative learning approaches thus improved CR to among children with SAM managed in OTCs in Karamoja, Uganda.
The initiative increased CR by enhancing return appointments for the refill of RUTF, adherence to the prescribed RUTF and screening and care for children with SAM in OTC with comorbidities. The missed appointments for refilling the RUTF by the caregivers is the main barrier to effective management and treatment of children with SAM in OTC in Karamoja. This study proved that it is possible for the health facilities to successfully address this challenge through close collaboration of the health workers with the VHTs and the local leadership. The successful sites generated a list of caregivers who missed their appointments and assigned VHTs to follow them up in their respective villages within 5 days, so the caregivers visited the health facilities to get the RUTF.
To address the challenge of the missed appointments for the refill of RUTF, the health facility teams provided a 2-weekly ration of RUTF to caregivers from ‘mobile communities’. The 2-weekly ration of RUTF instead of the routine weekly one ensured the caregivers had an adequate supply to feed the children until they returned home. This change’s success depended on the caregivers’ honesty and the mutual trust between them and the health workers managing the OTC services. It also relied on the commitment of the health workers to consistently identify caregivers who planned to move away from their usual homes before the next appointed return visit to the OTC.
Health workers integrated OTC service delivery into the EPI/eMTCT/ANC outreaches in the communities. By doing this, the health workers took the OTC services closer to the communities, reducing the missing out on the refills for RUTF for their children. The VHTs supported the health workers at the outreaches by screening and referring children with SAM without medical complications to OTC services. The health workers enrolled those who met the admission criteria into OTC in which they provided RUTF to the SAM cases. The caregivers sought subsequent refills from the health facilities as the outreach had monthly schedules, yet the routine clinics for OTC were weekly. This change depended on the health facility health workers’ ability to transport RUTF to the outreaches. NGOs funding IMAM programmes in the subregion often provided transportation assistance to the health facilities for the integrated outreaches. This change partly addressed the barrier of long walking distance to the health facilities identified elsewhere.18 20
To improve the client’s adherence to RUTF protocol, site teams engaged VHTs and local leaders in community dialogue meetings to monitor the administration and conditions in which RUTF are kept at home. By identifying caregivers whose children were not gaining weight and assigning VHTs and local leaders to monitor the administration of RUTF as prescribed, the health facility QITs addressed one of the widespread challenges affecting the attainment of CR >75% in Karamoja This behavioural change will require a lot of community mobilisation and engagement to fully understand and address the causes for caregivers’ low or no adherence to RUTF protocol. This calls for active engagement of community-based structures such as parish development committees, and community development officers and local council leaders who influence behaviour change of the caregivers, mainly by reinforcing the messages from health workers and VHTs towards proper utilisation of RUTF. Close collaboration among the departments of health and community-based services of the district, implementing partners and communities in the participatory design, implementation, monitoring and evaluation of effective behavioural change interventions for appropriate use of RUTF is paramount in this regard. Teshome et al20 recommend discouraging sharing of RUTF to help improve the treatment outcome for SAM and this change attempted to address this.
The final change that the health facilities carried out involved timely screening, identification and treatment of children with SAM in OTC with comorbidities. As such, the health workers in this study provided all the children enrolled in OTC with clinical assessment through OPD to identify and treat any other medical conditions before receiving the RUTF during the return visits. This helped to increase the response to SAM management using RUTF. This change has great potential to enhance the CR if all facilities adopt it. This is because comorbidities worsen the nutritional status of the children with severe wasting and compromise their ability to regain weight rapidly.3 20
Despite the gains achieved in the collaborative learning sites in this study, many factors are likely to compromise those achievements. The success in attaining the OTC CR of >75% hinges on the continued availability of RUTF in the health facilities, provision of the correct dosage of RUTF to all eligible children, counselling of the caregivers on its correct administration and use, the commitment of the caregivers to return for refills in the facilities as scheduled, and identification and treatment of all comorbidities. Whereas the initiative empowered the health workers with the knowledge and skills to deliver quality care for children with SAM, it falls short in its ability to address the socioeconomic and behavioural challenges which prevent caregivers from adhering to the SAM management protocol. The VHTs, the main facility-community linkage agents, contributed to this study’s improved CR. Nonetheless, on their own, they cannot sustainably influence the caregivers to adhere to the SAM management protocol for their children. It is possible that the application of community mobilisation and engagement initiatives that empower the communities to take charge of the timely identification, referral and follow-up of children with SAM in OTC could complement the CQI efforts in the health facilities. In particular, the engagement of influential community leaders could rally all members to take the management of SAM seriously. This would address the high default rate and non-response rate to SAM management among children in OTC.
Lessons and limitations
Lessons
CQI coaching and mentorship sessions strengthened the capacity of existing staff to take on QI projects. Most importantly, building the capacity of regional and district coaches and mentors was necessary to help cascade QI support to facility teams for sustainability.
Addressing the defaulting of children with SAM in OTC and encouraging adherence to the right management protocol for caregivers are critical for increasing CR. The successful interventions included following up on caregivers who missed their appointments for the refill of RUTF.
The mentorship and coaching sessions helped address the initial lack of RUTF at the health facilities, a reflection of poor supply chain systems. Supporting DHTs and QITs on the appropriate methodology of forecasting, ordering, distributing and monitoring RUTF at the health facilities is helpful. Redistribution of RUTF from the facilities which are overstocked to those with frequent stockouts is a potentially good strategy to address stockout in the facilities.
Study limitations
Only 10 of the initial 21 sites successfully implemented their CQI project to the end. However, the QI process and the associated change package were able to drive improvement on the selected indicators. Thus, project findings highlight the relevance of QI in improving key process indicators in health facilities that can ultimately improve health outcomes.
The project depended entirely on external donor support, which sometimes led to delays in the implementation and monitoring due to a breakdown in the funding cycle. Besides, the INGO, which started the project by directly supporting the sites, stopped partway through the project. This could have affected the consistency and quality of the outcomes. However, UNICEF managed this by working directly through the national and regional coaches and mentors, with Moroto RRH replacing the role of CUAMM and supporting coordination for the initiative at the regional level.
Other considerations for sustainability
Sustaining support from VHTs and other community health workers by further strengthening community-based interventions as stipulated in the IMAM guidelines and health service delivery package, including facilitating community-facility linkages and follow-up of children with SAM cases enrolled on OTC programmes.
Continuous monitoring and support supervision to sustain positive changes in improving the supply chain systems for nutrition commodities and distribution as part of the integrated national supply chain system.
Inclusion of lessons learnt from the initiative in the comprehensive health service delivery package to support quality service delivery at the district and health facility levels.
Create systems to sustain changes proven to improve processes at the clinic level; for example, document new ways of working and consider having health workers’ performance appraisals contain a section that assesses health workers’ performance.
With the CQI approach already part of the IMAM package for the delivery of quality nutrition services, the well-built capacity of the regional and district coaches in the approach is expected to support future sustainability of the achieved efforts with minimal or no support from donors or implementing partners.
Conclusion
This QI collaborative learning initiative increased the CR in OTC in Karamoja by addressing gaps in the treatment of comorbidities, adherence to OTC clinic appointments and proper use of RUTF by caregivers. The orientation of teams on collaborative improvement approaches, ongoing onsite coaching and mentorship sessions and engagement in regional learning sessions were critical for success. Without the close collaboration of the facility teams with caregivers, other household members, VHTs and community leaders, it would have been impossible to increase the CR in the region. Sustaining the gains of this initiative requires a commitment by DHOs, partners and health facility management to institutionalise the collaborative approaches. The performance is likely to improve further through the investment in community mobilisation and engagement for adherence to the treatment protocol, reducing the sharing of RUTF and seeking care for comorbidities among the children with wasting in OTC. This would require building a strengthened partnership between the district health departments and community-based services with support from implementing partners.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was not sought as this was a QI initiative to improve the uptake of existing government-approved, evidence-based clinical interventions. Given that no new clinical interventions were being introduced and no intervention was conducted that could cause harm, the team did not seek institutional review board approval or individual informed consent. Only deidentified, aggregate data were used, and data were used only to track and improve the processes of nutritional care and for learning about interventions that improved nutritional care.
Acknowledgments
All the District Health Officers, District Nutrition Focal Persons, District Quality Improvement Teams and health facility Quality Improvement Team in Karamoja, Senior Nutritionist, Management of Moroto Regional Referral Hospital, Lead national MNH and Nutrition coaches and mentors, Doctors with Africa (CUAMM) and IntraHealth Uganda.
Footnotes
Twitter @alexkmokori, @joyceDraru
Contributors AM is the first author. AM and AHN designed the Quality Improvement (QI) collaborative learning project, while DA and CNA provided technical support throughout the project implementation and monitoring. AM collected and analysed the data, drafted and edited the manuscript. CNA on the other hand, supported data collection, cleaning, and reviewing. The manuscript was finally reviewed and edited by AHN, DA, CNA, alongside two new entrants, RB and JD. AM is responsible for the overall content.
Funding Foreign, Commonwealth & Development Office (FCDO) funded UNICEF Uganda to implement the Karamoja Nutrition Programme (SC170633), under which this Collaborative Quality Improvement activity was implemented.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.