Article Text

Abstract
Background One of the main drivers of maternal and newborn mortality and morbidity in India is a lack of quality of care in health facilities. Inadequate competencies of health workers, insufficient quality of training and infrastructure, and the financial challenges of providing training across the country impede quality care provision. To this end, the Government of India began exploring cost-effective tech and IT-based solutions to support existing quality improvement (QI) initiatives.
Method We describe the process and approach of scaling the Safe Delivery App (hereafter referred to as the App) throughout India. The App is an mHealth learning tool for equipping health workers in managing obstetric and neonatal emergencies by placing evidence-based, and up-to-date clinical guidelines in their hands through their mobile devices. The use of the App was supported by the Ministry of Health and the Department of Health at the state level. Both parties were actively involved in the roll-out of the App and had a clear vision of how the App can complement existing structures/systems/programmes.
Results The App was successfully integrated and implemented in various government-led QI initiatives. Approximately 20 000 healthcare workers (HCWs) have been trained on the App and selected clinical topics since its launch, and between 2018 and 2021 over 86 000 HCWs across all states and union territories used the App. Moreover, project-specific data show a significant increase in the knowledge level of users of the App.
Conclusion Scaling such a tool within existing programmes is not a linear process. In India, the approach, government buy-in and flexibility of implementation modalities led to the successful roll-out of the App. We have demonstrated that an mHealth tool can be used to support the growing desire of governments to use tech in support existing QI initiatives and supporting the improvement of quality of care provided.
- Quality improvement
- Maternal Health Services
- Mobile Applications
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction and background
Quality of maternal healthcare in India
India has made considerable progress in reducing infant and maternal mortality over the last 30 years. The infant mortality rate decreased from 40 per 1000 live births to 30 per 1000 live births from the year 2013 to the year 2019.1 The maternal mortality ratio decreased from 556 per 100 000 live births from 1990 to 91 to 113 per 100 000 live births during the years 2016–2018.1
Since the 1990s, the Government of India (GoI) has launched various initiatives under the Family Welfare Programme with the specific aim of reducing the maternal mortality ratio by improving women’s access to maternal health services from pre conception, during pregnancy and labour, and after delivery. Under the Family Welfare Programme, the first initiative, Child Survival and Safe Motherhood Programme (1992–1995) addressed maternal health and mortality. Following this, the Reproductive and Child Health (RCH-1) programme (1997–2004) was established. Although the RCH-I programme deployed additional nursing staff at primary health centres, little effort towards improving the quality of services was included.2 3
In 2005, the RCH-2 was launched as a follow-up to RCH-1 and became the National Rural Health Mission (NRHM) programme. In 2005, the NRHM was launched to ‘provide universal access to equitable, affordable and quality healthcare’.4 Under the programme, various innovative strategies were introduced to accelerate progress towards reaching the United Nation’s Millennium Development Goal 4 and 5, which focused on reducing child and maternal mortality between 1990 and 2015.5 These strategies included the promotion of institutional deliveries through incentive schemes generating demand for health services, and efforts to mobilise the community by front-line workers called accredited social health activists. They also established and strengthened the public health infrastructure and resources to provide essential and emergency obstetric and newborn care services and strengthened referral linkages between facilities and communities through ambulance services.4 As a result, India observed a substantial increase from 41% in 2005 to 06%–79% in 2015–2016 in institutional deliveries from 2004 to 2014.6 Although India has made considerable progress in reducing maternal mortality over the past years, it remains high in low performing states (161 deaths per 100 000 live births).6 In 2013, the GoI launched ‘A Strategic Approach to Reproductive, Maternal, Newborn, Child Plus Adolescent Health (RMNCH+A)’ which focused on the continuum of care and emphasised the need for equitable access to high-quality care. The GoI identified 184 high priority districts for critical RMNCH+A interventions and developed a framework to provide technical support to state and district health departments with support from development partners.7 These districts were selected because they were behind on key maternal and newborn health indicators along with other socioeconomic and health system-related factors.
Despite these efforts, gaps were identified in the knowledge and skills of staff at public health facilities as well as their access to the latest national guidelines. Therefore, a need for further targeted interventions for ongoing capacity building was identified.8–12 One globally accepted strategy to improve healthcare practices, which is also cost-effective, is the use of mHealth tools to train and educate healthcare providers.13–15 While exploring tech and IT-based solutions to support existing initiatives, the Ministry of Health and Family Welfare (MoHFW), GoI, identified the Safe Delivery App (hereafter referred to as the App) as a potential solution. The Maternal Health Division of the MoHFW GoI reached out to Maternity Foundation and Jhpiego India in December 2015 to initiate discussions regarding the adaptation of the App to the Indian context and subsequently in February 2016, Maternity Foundation, Jhpiego India and MSD for Mothers came together to support the MoHFW with adapting the App for India. The cocreation of a nationally adapted version of the App aligned with national clinical guidelines was an essential pre condition for large scale roll-out in India.
The Safe Delivery App
The App is a digital tool developed by the Maternity Foundation, the University of Copenhagen and the University of Southern Denmark for equipping healthcare workers (HCWs) in managing obstetric and neonatal emergencies. The App empowers HCWs by placing evidence-based, and up-to-date clinical guidelines in their hands through their mobile phones or tablets. A randomised control trial conducted in Ethiopia showed a significant improvement in skills and knowledge of HCWs who used the App for perinatal care compared with a control group that followed regular training models.16 Subsequently, other studies also found an increase in knowledge of management of postpartum haemorrhage and neonatal resuscitation in all those who used the mobile application.17 18
The App includes 13 modules focused on evidence-based key interventions for women and newborns around the time of birth (Basic Emergency Obstetric and Neonatal Care (BEmONC)) and preventative procedures aligned with global or national clinical and treatment guidelines. The App’s ‘MyLearning’ platform is designed to gamify learning and motivate users to keep challenging themselves to learn more and progress through various levels. It provides users with the opportunity to enter a learning universe and test their knowledge on different thematic areas across three levels of difficulty comprising 12 questions. Once users complete the three levels for all thematic areas, and the final certification examination, they become a Safe Delivery Champion and earn a certification. The certification examination comprises 15 clinical situation-based cases containing a total of 51 questions. The certificate is achieved by scoring at least 70% and by not selecting any answer options with fatal outcomes to mother or child.
Methods
Developing the App: India version
A global version of the App has been available since 2015. Maternity Foundation, in collaboration with partners, adapt and customise the Global version to align with national guidelines for country versions. This was done for the Indian version of the App: a rigorous review process of the entire App involving all partners commenced to align and adapt that content with the MoHFW’s existing maternal and newborn health guidelines. The initial adaptation involved changes to the audio and visuals to be contextually relevant, and the first version of the App was developed in English. This was followed by seven additional Indian language versions of the App.
In June 2017, the Indian version of the App was pilot tested in four districts each from Madhya Pradesh, Odisha, Rajasthan and Jharkhand. The results were extremely encouraging, which ushered in a confidence prompting a wider roll-out. Following extensive review, adaptation process and backed by the results of the pilot, the Hon’ble Union Minister of Health, MoHFW, GoI launched the App in December 2017.
From 2018 to 2021, there have been more than 100 000 downloads of the App in India. Overall, 86 242 are active users of the App using the app as a job aid or self-learning tool and are from 698 districts across all 36 states and union territories (UTs). These figures may underestimate the true number of users; only data from online devices are captured. Out of the active users in India, almost 40% have registered on the ‘MyLearning’ and 9% have achieved Safe Delivery Champion status.
Reaching 100 000: scaling the App
Following the launch of the App, Maternity Foundation and Jhpiego India developed a plan to roll it out. The aim was to introduce the App into existing programmes or capacity strengthening exercises for HCWs, in collaboration with the MoHFW, other non-governmental organisations partners and stakeholders. The App can be used by different cadres of HCWs because its focus is on BEmONC signal functions, which are common procedures for all HCWs working in maternal and newborn departments. Despite efforts, there were approximately 11 000 users of the App in India in the 2018. Through the years, the GoI supported Maternity Foundation in cementing partnerships with multiple stakeholders including but not limited to USAID, BMGF, UNICEF, IPE GLOBAL, Jhpiego, IHAT, Care India, FOGSI, which supported growth in users programmatically and geographically.
Dakshata
In 2018, Jhpiego India informally introduced the App into the Dakshata programme—a ‘3 Days Technical Update cum Skills Standardization Training’—launched by GoI in 2015 to strengthen the quality of care during and immediately after childbirth. The App was introduced during state sensitisation meetings and was included in training packages for off-site trainers and mentors.
More recently, in 2020, the App was officially included in Dakshata as a learning aid for self-directed education to be used during and after the 3-day training. The App is integrated to provide incremental inputs and reinforced messaging after the training. The training is competency based focusing on improving the skills required for high impact interventions during and immediately after childbirth. The training includes a focused, yet comprehensive package based on a tested quality improvement (QI) framework supported by post-training mentoring. During mentoring, mentors and mentees discuss the previous weeks clinical cases and when clarity is needed, they will refer to the Apps relevant content to reinforce knowledge and skill.
Between 2018 and 2021, 10 613 active users reported that they learnt about the App through Dakshata. These users are distributed in 555 districts across 35 states and UTs. Overall, 43% have joined MyLearning and 14% have achieved Safe Delivery Champion status (table 1).
Safe Delivery App indicators for India, LaQshya and Dakshata initiatives, 2018–2021
LaQshya initiative integration
The big breakthrough happened when the App was integrated into the QI cycles of the national initiative 'LaQshya’—a labour room QI initiative launched by the Ministry of Health & Family Welfare in Oct 2018.19 Similarly, to adapting the App, a rigorous process ensued to integrate the App into the LaQshya guidelines and ensure it was used most effectively and efficiently to aid learning.
The recommendation for using the App in the LaQshya programme included:
Using ‘MyLearning’ to improve and sustain the knowledge of health staff between mentorship visits.
Making the App available for mentors to use throughout the QI cycles during their mentorship visits to health facilities to reinforce knowledge and skill learnt in previous training.
Standardising information on clinical guidelines across all LaQshya facilities.
Moreover, Maternity Foundation recommended how the App could be used across four main areas: self-directed learning through job aids, drills, discussions and objective structured clinical examinations, when conducting mentorship sessions to ensure uniformity and quality training was provided. Mentor proficiency of the App and Safe Delivery Champion status was a prerequisite before conducting any facility-level QI mentoring. Tablets preinstalled with the App were provided at each LaQshya facility’s nursing station to ensure health providers had ease of access.
Since the integration into LaQshya, a total of 11 184 users (13% of the total active users) have reported that they started using the App as part of the LaQshya initiative. The users are from 553 districts across 33 states and UTs and 43% of the users have registered on MyLearning and 11% have achieved Safe Delivery Champion status (table 1).
Midwifery integration
Alongside the initiatives focused on the intrapartum period, the GoI identified a need to strengthen the care and services delivered during the antenatal and postpartum period as well. Optimum midwifery services are among the most effective ways to reduce maternal, newborn and infant mortality.20 Scaling up quality midwifery care can lead to reductions in stillbirths, neonatal deaths and maternal deaths as Nove et al suggest ‘Scaling up to universal coverage by 2035 (scenario 3) could result in 67% fewer maternal deaths (40 fewer per million), 65% fewer stillbirths (300 fewer per million), and 64% fewer neonatal deaths (300 fewer per million)’.21
Therefore, to further improve the quality of care for pregnant women, mothers and newborns the GoI decided to roll-out the Midwifery Initiative. Through this initiative, GoI seeks to promote natural birthing by promoting a positive birthing experience, reducing overmedicalisation, respectful maternity care and decongesting higher-level healthcare facilities. The vision of the Midwifery Initiative is to roll-out midwifery services through establishing midwifery-led care units in the labour room of high caseload public healthcare facilities by creating a cadre of Nurse Practitioners in Midwifery (NPM) in India. With this vision, GoI released the Midwifery Guidelines in 2018.
To train the NPMs and ensure an elevated level of care and practice, the Indian Nursing Council (INC), in 2021, identified the App to be a relevant tool to support midwifery training. The INC included the App into the training to be used as a self-directed and experiential learning tool supported by scenario-based learning to help them understand and practice well. INC included the App in the ‘NPM’ and the ‘NPM Educators’ curriculum.22
Preservice education curriculum integration 2020–2021
Preservice training is the first step to acquiring fundamental skills for HCWs, particularly nurse midwives. Midwifery training requires a focus on skill development and confidence building through the real-life application of skills. Applied or contextual learning is much more effective in knowledge retention than simple didactic lectures.23 It allows students to integrate ‘content knowledge with knowledge of the context’.24 The INC recognises the relevance of the App as a self-directed learning tool in preservice education and later as an up-to-date reference tool on-the-job for nurses and midwives. To support students to establish the foundation for their continuous learning journey, in July 2021, the INC integrated the App Certification as a mandatory module in the revised BSc Nursing curriculum for completion between semesters VI and VII during their study.22 Thus, all new BSc Nursing students will work through the App and become a Safe Delivery Champion as part of the education during their seventh semester. In 2018–2021, only 6% of all the users were students. With the integration of the App into the BSc Nursing curricula, it is expected this will increase over the years.
Accreditation of App by INC
The INC also approved the App as a tool for continued professional development with effect from November 2021. Members who achieve the ‘Safe Delivery Champion’ certificate receive 15 continued nursing education credit hours.
Results and lessons learned
Since the launch of the Indian version of the App, usage has been gradual across districts and states in India. Uptake of the App has been better in the states and districts where targeted efforts were made to roll-out the App, such as Chhattisgarh, Madhya Pradesh, Uttar Pradesh, Maharashtra and Bihar.
A growing body of evidence supports using the App in India. In 2019, the App was introduced in 33 facilities across six districts in Bihar. Overall, 249 nurses used the app for 3 months. Overall, 229 nurses completed a pretest and post-test knowledge assessment on four domains: active management of third stage labour, postpartum haemorrhage, neonatal resuscitation and management of pre-eclampsia and eclampsia. Significant (p<0.05) improvements were observed across all domains. However, much scope for improvement remained after 3 months, suggesting that efforts are needed to support continued learning.
Similarly, significant improvement in knowledge was also observed in a preservice setting. Usmani et al18 found that the App was effective in improving nursing students’ knowledge regarding active management of third stage labour, postpartum haemorrhage and neonatal resuscitation. More recently, a study conducted in Uttarakhand and Jharkhand states compared knowledge and confidence outcomes of participants receiving an introduction to the App with participants who received an introduction to the App and additional bimonthly support for 6 months. Knowledge and confidence of the HCWs significantly increased from baseline to end line by 4% points (p<0.001), and participants who received continuous support had a higher mean score difference in knowledge and confidence compared with those who did not receive facilitation (p<0.001).25
App user data
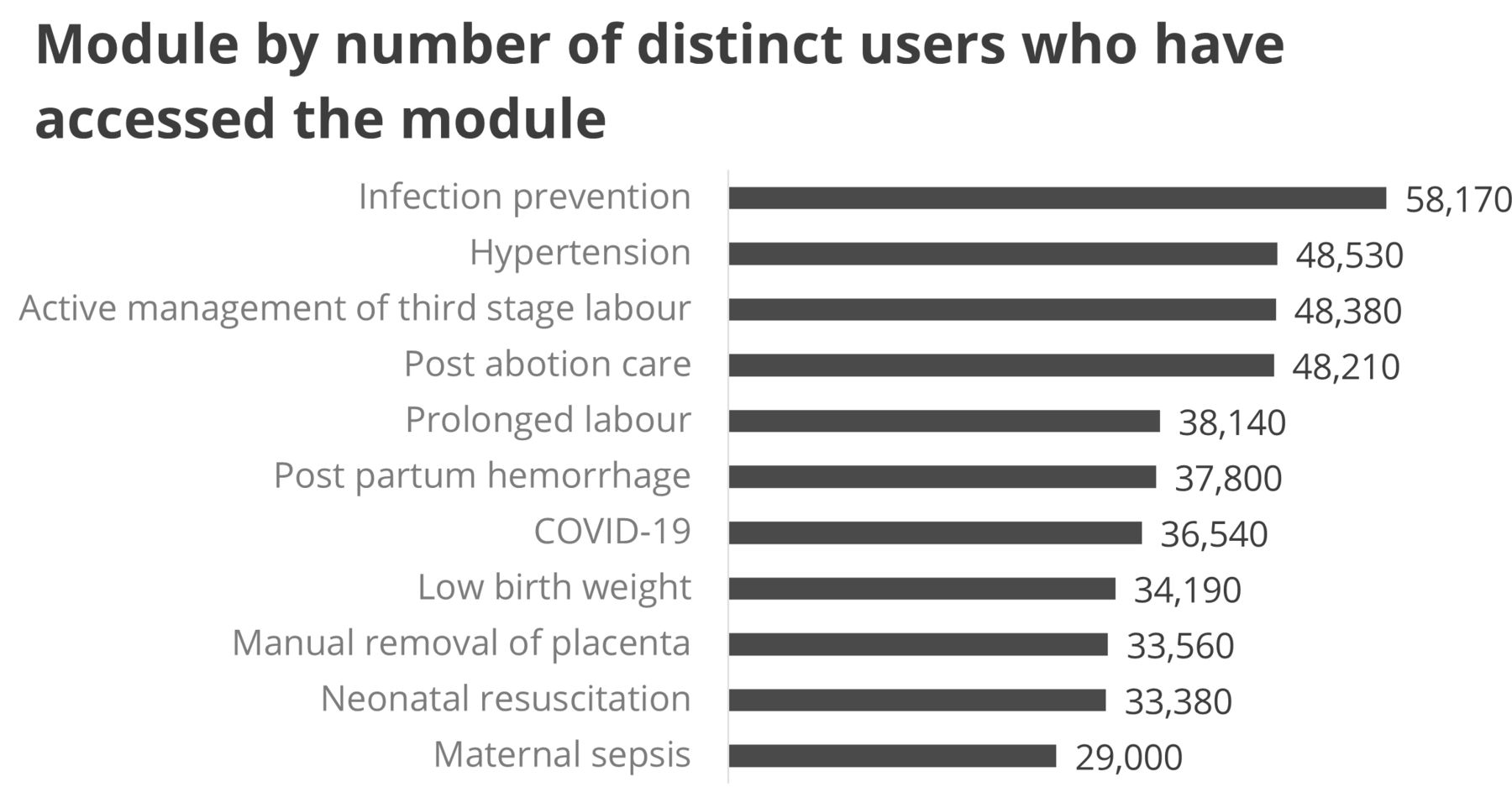
User data show utilisation of the App across all the thematic areas. High usage (approximately 48 000) has been recorded for the infection prevention, hypertension, active management of third stage labour and postabortion modules indicating that users found these modules more relevant (figure 1).
{kind=link}
Module by number of distinct users who have accessed the module.
‘MyLearning’ is the most frequently used feature of the App by users in India. This happened as the App was scaled and integrated into various initiatives and programmes and achieving Safe Delivery Champion status was made mandatory in LaQshya and for the BSc Nursing education. Content wise, the introductory videos are the most frequently watched (30% of users). Following this, the COVID-19 video has been watched the most (17% of users) although it has been added recently. This suggests that whenever new clinical information is added, given the greater need to learn and update knowledge, (such as COVID-19 information), there is more traction and utilisation of the App. Fewer users have accessed the action cards, practical procedures and drugs indicating a need to encourage more users to access this content or rethink the design of the App features.
Learning from the App roll-out
The roll-out process happened at multiple levels over the past 5 years. The lessons learnt from the process and engagement with the GoI and other partners are enlisted below.
National adaptation and integration was a prerequisite
Many resources were invested in the development of the App; it took almost 2 years of development. Although the process of adaptation, alignment and approval from GoI was a major task, it was also an essential step. For the Indian version of the App to be available as a complete tool and readily available for integration, the codevelopment and approval were necessary. The App’s integration into the LaQshya programme paved the way for the integration into the Midwifery Programme, which further supported the inclusion into the BSc Nursing Curriculum, making the App an educational tool for HCWs throughout their entire service journey.
Power of partnership (government ownership, state buy-in, strong partnerships)
Leadership at the highest level in the Ministry of Health and the Department of Health at the state level believed in the power of information technology and were actively involved in the roll-out of the App. The decentralisation of the Indian health system posed a challenge for the roll-out because integration at the national level was not in itself enough to ensure roll-out at the state level. However, the flexibility of the roll-out approach enabled states to adapt to their specific context and priorities, which increased the state-level ownership. Leveraging other technologies such as group video sharing of presentations or self-explanatory videos played an essential role in delivering large-scale training and reaching end-users directly. These simplified implementation models, training packages and strong partnerships at various levels helped us reach users without having on-the-ground presence in each state.
On-the-ground presence
Achieving and sustaining momentum without on-the-ground presence is a challenge. Despite a well-designed implementation plan and good partner intentions, it proved difficult for Maternity Foundation to operate through implementing partners and remote support alone. It was challenging to keep the momentum and seize relevant opportunities without an on-the-ground presence. A high attrition rate of the project staff, shifting priorities of stakeholders and availability of funds had an impact on the scale-up and sustainability. Maternity Foundation realised the importance of engaging directly with MoHFW to ensure the inclusion of the App within existing and upcoming government programmes. By the end of 2018, Maternity Foundation, which was managing the work in India remotely, brought a full-time person on board to manage the work. Project staff remains important in the wider roll-out of quality improvement initiatives, and hence the roll-out of the App so for the coming years will also be vitial in the initiative. However, by integrating the App into curricula and e-learning platforms, a pathway to sustainability has been created and will be sustainable without project-specific staff.
The learning platform of the App
State and health facility leadership played a pivotal role in encouraging progress on the MyLearning platform. State leadership facilitated healthy competition among HCWs and publicly recognised Safe Delivery Champions at various state and district level functions. At the health facility level, Safe Delivery Champion badges were handed out, certificates were posted on notice boards, and ceremonies were conducted to celebrate champions. Some states made the App Champion certificate mandatory for the HCWs and programme managers have included the number of Safe Delivery Champions in their monitoring system. These efforts further motivated and encouraged staff at facilities to achieve Safe Delivery Champion status.
Using App data insights and community of practice
Continuous monitoring and feedback are needed for effective and sustained roll-out. Extracting and sharing data insights from the App with state governments and partners proved helpful to keep up the motivation for continued roll-out efforts. At the state level, communities of practice were established—a WhatsApp group was formed for all LaQshya facilities for sharing and learning best practices. State-level mentors also used this platform to encourage facility teams to initiate and complete MyLearning. Sharing insights and case examples at various national platforms and fora also helped create awareness and reach more states.
Focused training on the App
During the roll-out and training, it was realised that many HCWs were inexperienced with smartphones so focused training on the App as an innovative technology was fundamental. During training, special focus regarding the process of the downloading of the App and the stepwise process of onboarding was explained along with the features of the App.
Next steps
To further support the health system in India and strengthen the role and suitability of the App, Maternity Foundation will focus on three areas going forward: technology and interoperability, clinical content, and further institutionalisation.
Technology and interoperability
A key focus for strengthening the App in the coming years is to boost the core technology of the App as well as integrate machine learning methods to enhance the personalised learning experience of users. We will also continue to work with partners such as Asterika and World Continuing Education Alliance who own other platforms and offer users the Safe Delivery content to maximise access to the clinical content.
Content for the App
We continue to increase the content offered on the App. We aim to move beyond obstetric and neonatal emergency management to add more content related to antenatal care, family planning and other content according to identified needs.
Enhancing the reach through institutionalisation
Building on the past achievements, Maternity Foundation India is now focused on the longer-term institutionalisation of the App to help transform training programmes to unlock HCWs' learning potential across India. We plan to continue to support the capacity building of HCWs by supporting the development of in-service and preservice learning packages, scaling implementation and partnerships and supporting the government to replicate these models avoiding the creation of parallel learning systems and duplication.
Limitations
This paper has focused on the journey of scaling the App where Maternity Foundation prioritised building awareness of the App and integrating it into existing programmes and initiatives. This has meant that the measurement of the success and impact of the App are limited to improved clinical knowledge and skills; and practices have not been included in any observations/measurements. Therefore, Maternity Foundation have been unable to capture information related to how improved knowledge and skills transfers to clinical practice, case management and/or protocol compliance. Maternity Foundation plan to explore this area in future roll-out and, on a project, specific basis.
Conclusion
Maternity Foundation has successfully implemented and scaled the App within various capacity strengthening initiatives across India. The process has not been linear but through strong partnerships, ownership, and national and state governments championing the App, it gradually became a formal tool for capacity building of HCWs. Through the successful integration into the LaQshya initiative, additional opportunities to scale the App arose and Maternity Foundation responded quickly and supported the integration of the App.
The demand for the App and related support by key stakeholders in India suggests that the Maternity Foundation is addressing an unmet need to build critical knowledge and skills among HCWs. The ability to respond quickly by identifying the need of adding new language versions and thereby reach more HCWs with updated guidelines and protocols have proven well suited in supporting the GoI in the health system strengthening initiatives launched over the past 4 years.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We thank the Ministry of Health and Family Welfare, National Health Mission, NQOCN, UNICEF, USAID, Jhpiego, IPE Global for their continued support in integrating the Safe Delivery App into their programmes and supporting the scale-up. Moreover, we would like to thank the healthcare workers in India for embracing the use of the Safe Delivery App in their work. Finally, we would like to thank MSD for Mothers who support in funding the work in India.
References
Footnotes
Twitter @SudkeAjitkumar
Contributors TSS was responsible for the conceptualisation of the idea. AG, AB, BM and TSS drafted the manuscript. AS reviewed the manuscript. LTS reviewed and revised the manuscript. LTS is the guarantor.
Funding MSD for Mothers, grant number: MFM-20-132989. Publication of this article is made Open Access with funding from the Nationwide Quality of Care Network.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.