Article Text

Abstract
Objective To reduce the incidence of metabolic bone disease (MBD) among very low birthweight (VLBW) infants admitted to neonatal intensive care unit from baseline of 35% by 50% over 2 years by implementing a quality improvement (QI) initiative.
Methods A multidisciplinary QI team used evidence-based interventions and the healthcare improvement model to reduce MBD rate in VLBW infants. The specific interventions included routine enteral supplementation of calcium and phosphorus using Human Milk Fortifier (HMF) to expressed breast milk by day 14 of life (Plan/Do/Study/Act (PDSA) cycle 1), parenteral and early enteral supplementation of calcium and phosphorus (PDSA cycles 2 and 3). We included VLBW infants admitted within the study period at birth and excluded babies with congenital malformations, skeletal disorders and those who died before 2 weeks of age. Compliance with adding HMF by day 14, compliance with adding calcium and phosphorus in total parenteral nutrition (TPN) from day 1 of life and compliance with starting HMF when the baby reached 100 mL/kg/day of feeds were used as process indicators. The incidence of MBD was used as an outcome indicator during the study. The incidence of MBD was tracked using the Statistical Process Control methodology.
Results The baseline MBD rate in 2015 was 35%. After the first PDSA cycle, 20% developed MBD (p=0.02). The same was sustained for a period of 1 year with the rate of 22%. After the second and third PDSA cycles, there was a drop in the MBD rate to 17%, and sustained for 3 months with 21%.
Conclusion Implementation of QI initiatives decreased the MBD rate from 35% to <20%. Early parenteral calcium and phosphorus supplementation in TPN and optimising enteral supplementation with multicomponent fortifiers appear to have significant reduction in the incidence of MBD.
- Quality improvement methodologies
- Evidence-Based Practice
- Healthcare quality improvement
- Statistical process control
- Paediatrics
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Quality improvement methodologies
- Evidence-Based Practice
- Healthcare quality improvement
- Statistical process control
- Paediatrics
WHAT IS ALREADY KNOWN ON THIS TOPIC
Metabolic bone disease (MBD) is a known complication of prematurity caused by undermineralisation of bones arising from inadequate calcium and phosphorus during antenatal and postnatal period.
WHAT THIS STUDY ADDS
Simple interventions of optimising the calcium and phosphorus intake through breast milk fortification and parenteral supplementation in total parenteral nutrition help in the reduction of MBD of prematurity.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This quality improvement project provided a mechanism to reinforce evidence-based feeding guidelines and develop dedicated policy especially for MBD prevention in very low birthweight babies.
Introduction
Metabolic bone disease (MBD) of prematurity, earlier known as osteopenia of prematurity, is an important complication of prematurity. MBD is inversely related to gestational age.1 The exact incidence of MBD is not known due to a lack of consensus on the standardisation of the definition of MBD. MBD is estimated to occur in 16%–40% of very low birthweight (VLBW) babies.2 The prevalence of MBD is increasing because of recent advances in neonatal care resulting in survival of extreme preterm babies. Despite aggressive parenteral nutrition and standardised enteral feeding protocols, MBD continues to be a major cause of morbidity among VLBW infants.
There is no standard definition for diagnosis of MBD. Dual energy X-ray absorptiometry (DEXA) is the gold-standard method for assessing bone mineral density.3 Because of the hazard of radiation exposure and the cost involved, DEXA is still being used as a research tool in resource-limited settings. Another promising tool is quantitative ultrasound of bone (QUS) using speed of sound technology. But due to non-availability of ultrasound probes and lack of neonatal reference values, it is not used to assess bone mineral content in routine clinical practice. Studies have used the radiological definition based on X-rays taken at 6-week postnatal age.4 By the time radiological changes have appeared, the bone demineralisation of 40%–50% would have occurred.5 Biochemical markers of MBD guide us in the early identification and prevent progression of the disease and its complications. Therefore, in our study, we have used the biochemical definition for MBD, based on serum alkaline phosphatase (ALP) levels. Babies with serum ALP level >800 IU/L or >600 IU/L with rising trend and the rising ALP could not be attributed to any other cause were labelled as having MBD.2
In our unit, the overall incidence of MBD was 35% among VLBW infants. The team collected data retrospectively from the case sheets and nominal register to establish the baseline incidence of MBD in the unit. This quality improvement (QI) initiative aimed at reducing the incidence of MBD among VLBW infants admitted to neonatal intensive care unit (NICU) from the baseline of 35% by 50% over 2 years by implementing a bundle of standardised supplementation practices.
Methods
Setting
The study was conducted in a level III NICU in Chennai. The Department of Neonatology caters for both inborn and outborn babies with an average of 4500 deliveries per year and 1000 admissions to NICU per year. During the study period, the overall mortality rate was 8/1000 live births, and survival among VLBW and extremely low birthweight (ELBW) babies were 96% and 90%, respectively. Fifty per cent of the mortality was due to preterm babies <26 weeks’ gestation. The NICU is fully equipped with 24 intensive care beds/high dependency beds and 40 nursery beds.
This QI project involved implementing evidence-based interventions to reduce MBD rate in VLBW infants admitted to the NICU. All VLBW infants admitted to NICU during the study period and whose parents consented for the study were included at birth. Babies with congenital malformations, skeletal disorders and those babies who died before 2 weeks of age were excluded from the study. A multidisciplinary QI team was formed consisting of a primary investigator, two consultant neonatologists, two senior residents, four staff nurses and one pharmacist.
The baseline incidence of MBD among all VLBW babies admitted to NICU was established. The team met monthly to review literature regarding pathophysiology, presumed aetiology and evidence-based research that support MBD prevention. They established strategic aim and key driver interventions, and designed changes as shown in figure 1. The QI team was responsible for chart reviews to audit compliance with baseline as well as during increased spikes in MBD rates.
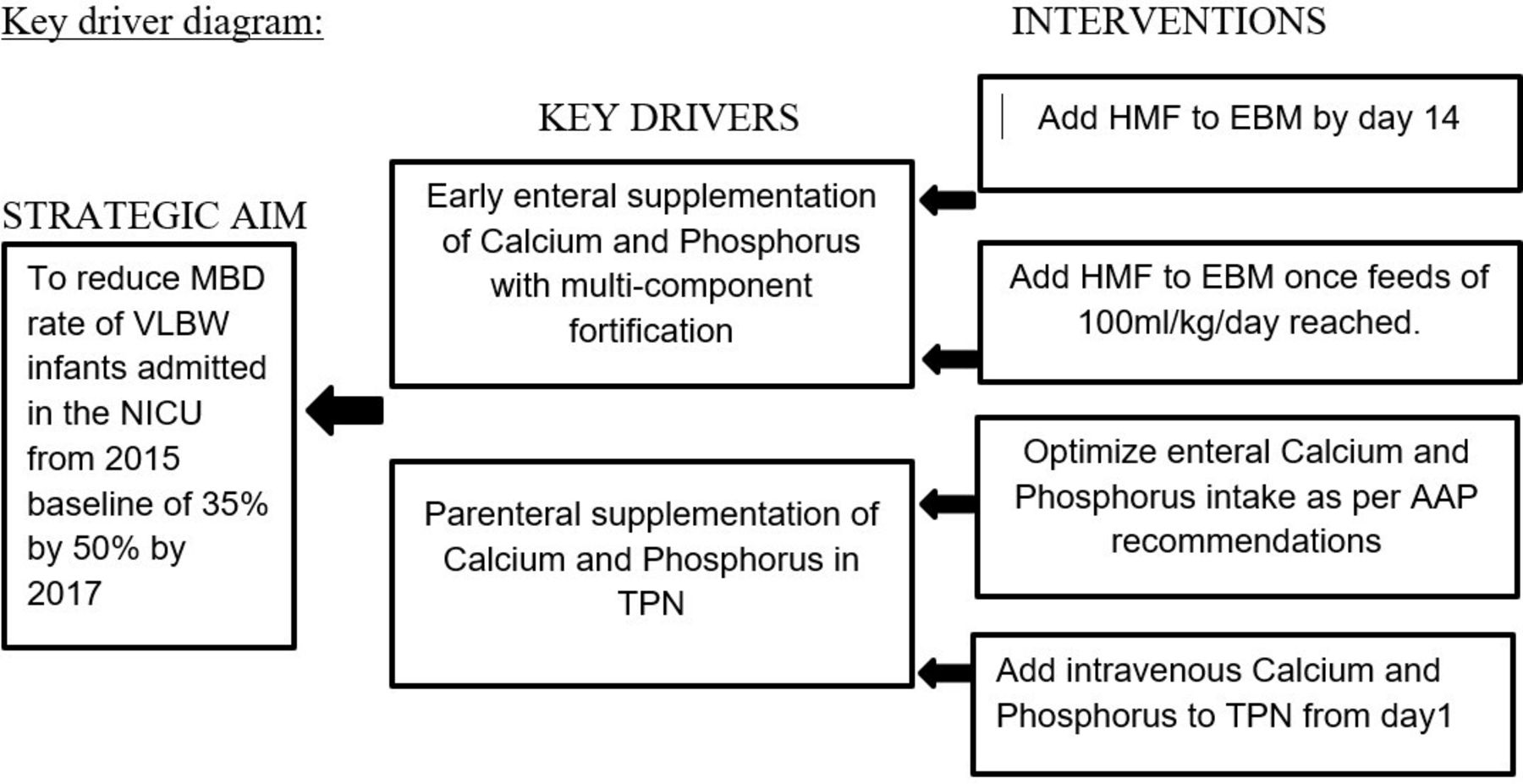
Key driver diagram summarising specific interventions driving key baseline changes aimed at achieving the specific aim of MBD rate reduction by 50%. AAP, American Academy of Pediatrics; EBM, expressed breast milk; HMF, Human Milk Fortifier; MBD, metabolic bone disease; NICU, neonatal intensive care unit; TPN, total parenteral nutrition; VLBW, very low birth weight.
Key driver interventions
Early enteral supplementation of calcium and phosphorus with multicomponent fortification.
Parenteral supplementation of calcium and phosphorus in total parenteral nutrition (TPN).
Intervention 1: early enteral supplementation of calcium and phosphorus by multicomponent fortification of expressed breast milk (September 2015–March 2016)
The team reviewed the pre-QI flow charts and fishbone diagrams to decide on the intervention. The previous policy was to add multicomponent fortifier Human Milk Fortifier (HMF) only if there was inadequate weight gain in spite of reaching 175–200 mL/kg/day of feeds and mono-component supplementation of calcium and phosphorus if serum ALP >750 IU/L. This policy was revised and the team prioritised early routine enteral calcium and phosphorus supplementation with the multicomponent fortifier HMF to expressed breast milk (EBM) as the first PDSA (Plan/Do/Study/Act) cycle to reduce MBD. We chose to implement this intervention first as it was simple, easy and feasible. It would not need too much of resources and equipment, and could also be of value to the patient.
Central line was accessed and aggressive TPN started on day 1 of life without calcium and phosphorus for all VLBW babies. Trophic feeds (10–15 mL/kg/day) of EBM or donor milk were started on day 1 of life and feeds were increased by 20–30 mL/kg/day as per unit protocol. TPN was stopped once feeds of 125 mL/kg/day were achieved. HMF was added to EBM on day 14 of life and/or at least 125 mL/kg/day of enteral feeds reached. Feeds were increased to achieve a target volume of 175–200 mL/kg/day. Fortification was started at a concentration of 1:50 (1 sachet of HMF added in 50 mL of EBM/donor milk) and if this was tolerated for 48 hours, then increased to 1:25 (1 sachet of HMF added in 25 mL of EBM/donor milk as per manufacturer’s recommendations). When EBM was fully fortified with HMF, it would provide minimum of 150 mg/kg/day of calcium and 75 mg/kg/day of phosphorus. Nurses were trained in the preparation of fortified milk. They were educated about its storage. Enteral intake of calcium and phosphorus was targeted according to the ESPGHAN (European Society for Paediatric Gastroenterology Hepatology and Nutrition) recommendations with calcium of 100–140 mg/kg/day, phosphorus of 65–90 mg/kg/day and vitamin D 1000 IU/day.6 Monitoring for MBD (serum calcium, serum phosphorus and ALP) was done weekly from 2 weeks of life until discharge.
Intervention 2: multiple changes towards reduction of MBD rate (June 2017–September 2017)
With the outcomes of intervention 1 and review of literature regarding MBD, the team came up with other evidence-based interventions to further enhance calcium and phosphorus supplementation. Parenteral calcium and phosphorus were added to the TPN as PDSA cycle 2. If the line is central in position, then 6 mL of 10% calcium gluconate and 0.35 mL of potassium phosphate were added to 100 mL of TPN. This provided calcium of 60 mg/100 mL TPN and phosphorus of 32 mg/100 mL TPN. If the line was not central in position, then 3.6 mL of 10% calcium gluconate and 0.2 mL of potassium phosphate were added to 100 mL of TPN. This provided calcium of 36 mg/100 mL TPN and phosphorus of 19 mg/100 mL TPN. Targeted intravenous intake of calcium was 20–90 mg/kg/day, and phosphorus was 35–70 mg/kg/day.6 7 Molar ratio of calcium and phosphorus for TPN was maintained at 1.5:1 to prevent precipitation. The orders for the TPN were written by the doctor on duty with the help of an Excel-based TPN worksheet. TPN was then prepared by the pharmacist with the help of the senior nurse. TPN was prepared under laminar airflow. Dextrose, amino acids, electrolytes, multivitamin, calcium and phosphorus were added in the same order for TPN preparation to prevent precipitation. The TPN was visually inspected for precipitation and if present, was discarded. TPN was stopped once enteral feeds of 125 mL/kg/day were achieved. HMF was added to EBM once feeds of 100 mL/kg/day were achieved as PDSA cycle 3. In the team meeting, the consensus was to change the target enteral calcium and phosphorus supplementation according to the American Academy of Pediatrics (AAP) recommendations. AAP recommends calcium, phosphorus and vitamin D supplementation of 150–200 mg/kg/day, 75–140 mg/kg/day and 400 IU/day, respectively.8
The team also reviewed the usage of drugs like methylxanthines, diuretics and steroids which are risk factors for MBD. Unit policy was not to use sedation routinely during ventilation. The usage of postnatal steroids and diuretics was less than 1% in our unit. These interventions and policy changes were discussed in the team meeting every month. Change in this policy was educated to all doctors and nurses, and the same was displayed in the NICU, nursing working desk, computer table and TPN preparation room. Owing to the natural history of the disease and the prevalence of MBD, the team decided to have monthly meetings and the statistical charts were displayed periodically throughout the study period every 3 months.
Analysis and measuring the quality of care
Development of process and outcome indicators
The team decides to use indicators for tracking calcium and phosphorus supplementation. Compliance with adding HMF by day 14 was used as a process indicator during intervention 1. Compliance with adding calcium and phosphorus in TPN from day 1 and compliance with starting HMF when the baby reached 100 mL/kg/day of feeds were used as process indicators during intervention 2. The incidence of MBD was used as an outcome indicator during both the periods of interventions 1 and 2.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our study.
Statistical analysis
Descriptive statistics were represented as number and percentage, mean and SD or median and IQR as appropriate. Compliance with the intervention process was analysed using Statistical Process Control (SPC) charts.9 Whenever the values were above or below 3 SDs, the common cause or specific cause variation was looked for. The tests of significance used for the outcomes were Χ2 test for categorical variables. All the statistical analyses were done using SPSS V.16.0 and SPC software. A p value of <0.05 was considered statistically significant.
Results
A total of 296 VLBW infants were enrolled in three phases. Period 1 represented the baseline period with 82 babies. Period 2 comprised of 146 neonates with 50 in intervention phase 1 and 96 in the sustainability phase 1. Period 3 included 68 neonates with 35 in the intervention phase 2 and 33 in sustainability phase 2 periods. The percentages of ELBW babies were 27%, 25% and 41% in period 1, period 2 and period 3, respectively. The mean gestational age of babies in periods 1, 2 and 3 was 30.4 weeks, 29.7 weeks and 29.42 weeks, respectively. The mean birth weight of babies in periods 1, 2 and 3 was 1132 g, 1139 g and 1062 g, respectively.
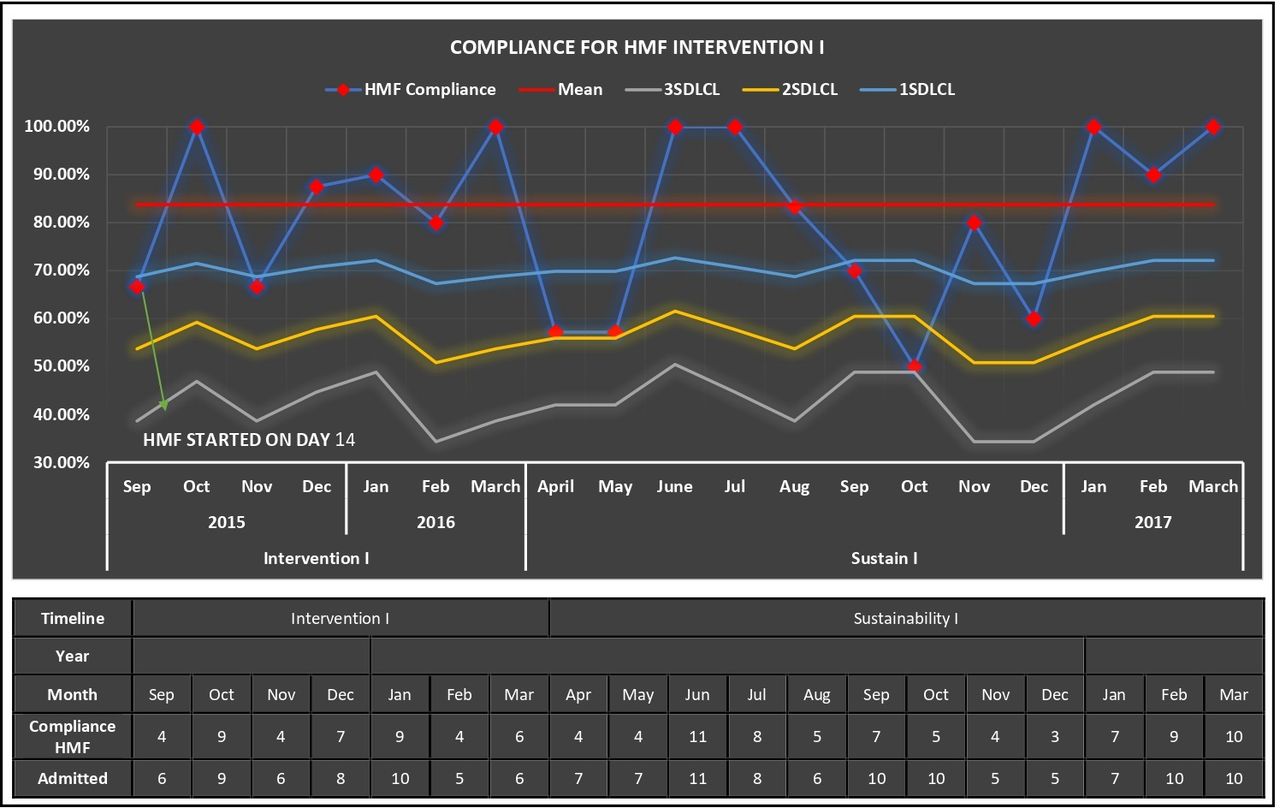
In the baseline period, the proportion of babies who were started on HMF was 11% (9 out of 82 infants). There was an increase in compliance with adding HMF to EBM on day 14 of life during period 2 and the mean compliance achieved was 86% (figure 2). There was a gradual decline in compliance during July, August and September, and a sudden drop in October of sustainability period of intervention 1, but none of the points on the chart dropped less than the lower control limits. The team addressed this in the meeting and found that there was limited supply of HMF due to logistics reasons. After discussion with the in charge of the pharmacy and the authorised dealer of HMF, it was made available in the pharmacy and supplies were ensured. Once the supplies were restored, the compliance improved and was sustained. All babies were on EBM when HMF was supplemented during the study.
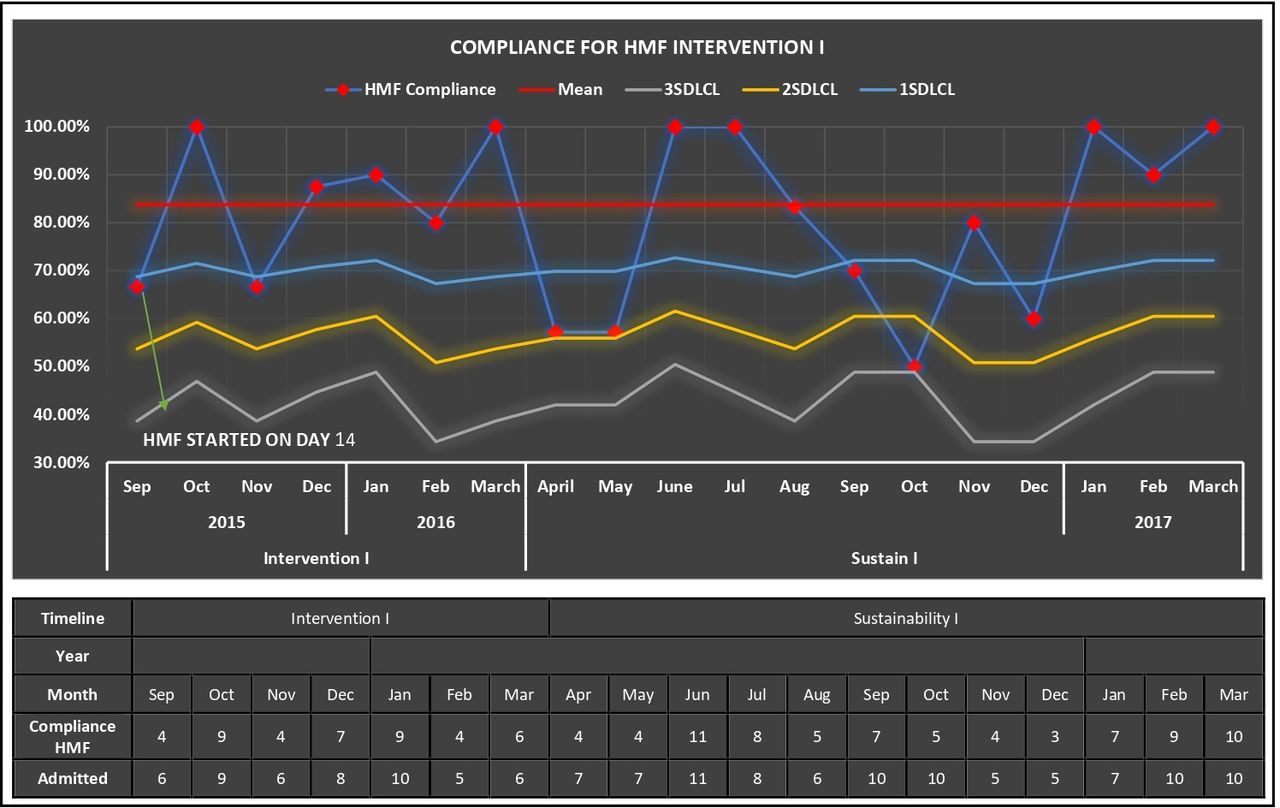
SPC chart for starting HMF on day 14 (PDSA 1). HMF, Human Milk Fortifier; PDSA, Plan/Do/Study/Act; SPC, Statistical Process Control.
The compliance with adding calcium and phosphorus in TPN was 83% during intervention 2, which increased to 100% in the sustainability period (figure 3). The compliance for adding HMF early at 100 mL/kg/day feeds improved significantly to 91% during the intervention 2 period. There were no points below the mean for the period (figure 4).

SPC chart for starting parenteral calcium and phosphorus in TPN on day 1 (PDSA 2). PDSA, Plan/Do/Study/Act; SPC, Statistical Process Control; TPN, total parenteral nutrition.
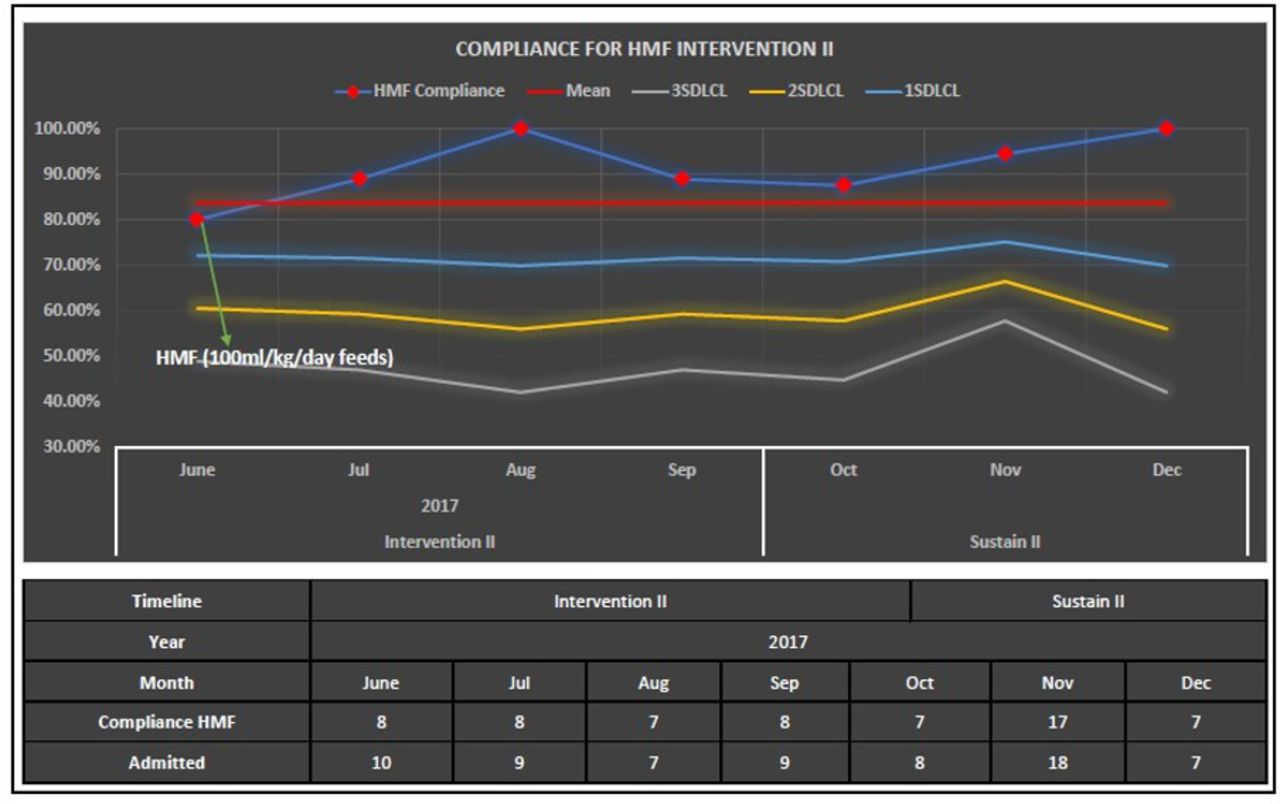
SPC chart for starting HMF early at 100 mL/kg/day feeds (PDSA 3). HMF, Human Milk Fortifier; PDSA, Plan/Do/Study/Act; SPC, Statistical Process Control.
The baseline MBD rate was 35% (29 cases for 82 infants). After initiation of early enteral supplementation of calcium and phosphorus by multicomponent fortification of EBM in September 2015, only 20% (10 cases of 50 infants) developed MBD (p=0.02). The same was sustained for a period of 1 year (April 2016–March 2017) with the rate of 22%. After the initiation of intervention 2 in June 2017, there was a drop in the MBD rate to 17%, and sustained for 3 months (October 2017–December 2017) with 21% (figure 5). Our baseline incidence of MBD among <1000 g babies was higher with 82%. The incidence dropped to 56% during period 2, and further decreased to 42% during period 3.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
SPC chart for the incidence of MBD throughout the study period. MBD, metabolic bone disease; SPC, Statistical Process Control.
Discussion
In this QI initiative, we were able to bring down the MBD rate among VLBW infants in our NICU from baseline incidence of 35% to 19% by implementation of key driver interventions over a 2-year period.
Our interventions of enteral and parenteral supplementation of calcium and phosphorus for MBD prevention were derived from previously published reports. In India, there was no recommendation for routine fortification of EBM. The WHO and national bodies like National Neonatology Forum of India do not support the routine use of multicomponent fortification and recommend fortifier usage in <32 weeks and <1500 g who fail to gain adequate weight despite breast milk volume consumption of 180 mL/kg/day.10 In an online survey conducted in 2013 on the use of HMF in India, 104 tertiary care neonatal units participated. Overall, 88% neonatologists were using HMF in NICU, of which 11% used it routinely in babies with birth weight less than 1800 g, 32% of them used in all VLBW babies, and 43% used HMF as and when there is inadequate weight gain.11 Likewise, in our unit, the previous policy was to fortify EBM only if there was inadequate weight gain with full enteral volume of feeds.
Our baseline incidence of MBD (35%) among VLBW was similar to that published in literature of 16%–40%.5 Mitchell et al reported an incidence of 28% MBD among VLBW infants, of which 56% had radiological rickets.12 During period 1 (baseline period), the incidence of MBD was 35%. Only 11% of them were started on HMF for inadequate weight gain. The concerns were that the protein content of available HMFs was bovine in origin, the issues of increased osmolarity, feed intolerance, necrotising enterocolitis (NEC), contamination, infection and lack of regular supplies. The possible hazardous effect of feed intolerance or NEC was studied by other authors13 14 and showed that there was no significant increase in NEC rates or feed intolerance in the fortified group. This was discussed in team meetings and the same information was disseminated to all others in the unit.
Due to the non-availability of intravenous phosphorus preparation at that point of time, we proceeded to implement the first key driver intervention of enteral supplementation by routine fortification of EBM by day 14 of life during period 2 (PDSA 1). The intravenous preparation shortage appeared to be universal. Calcium gluconate and potassium phosphate were the top two in the list of parenteral nutrition products in short supply in the American Society for Parenteral and Enteral Nutrition product survey.15 We followed the ‘standard’ type of fortification where HMF with fixed amount of macronutrients and micronutrients was added to breast milk on day 14 of life when babies would have achieved enteral feeds of at least 150 mL/kg/day. After the first intervention was done, the rate of MBD significantly reduced to 20% and was sustained for a duration of 1 year with MBD incidence of 21%.
In our NICU, it was a practice to start early aggressive TPN from day 1 of life for all VLBW infants. Though the association between parenteral calcium and phosphorus supplementation and prevention of short-term bone strength decline after birth in preterm infants has been emphasised in various studies,16 the non-availability of phosphate preparation prevented us from using parenteral calcium and phosphorus. During period 3, once the availability of parenteral preparations was assured, we implemented the second key driver intervention of parenteral calcium and phosphorus supplementation in TPN from day 1 (PDSA 2). Multiple other interventions, which were identified after the PDSA 2 towards reduction of MBD rate, were also implemented. Measures undertaken included further enhanced enteral supplementation of calcium and phosphorus by adding HMF earlier at 100 mL/kg/day feeds (PDSA 3), aiming to achieve AAP recommendations for calcium and phosphorus,8 which was higher than the ESPGHAN recommendations which was used earlier. Like other authors, we faced solubility issues with parenteral calcium and phosphorus preparations. There was precipitation seen in the TPN fluid twice, which was analysed. Once it was the excess amount of phosphorus (exceeding the recommended 1.7:1 molar ratio of calcium to phosphorus), and in the second instance, it was probably procedural and did not occur when TPN was reconstituted again.
The compliance with the interventions improved significantly with regular appraisals and group discussions. There was a stepwise increase in compliance with adding HMF from baseline 11% in period 1 to 83% and 91% in period 2 and period 3, respectively. The compliance with starting parenteral calcium and phosphorus in TPN increased and reached 100% during period 3. Due to logistic reasons, HMF was not available for 10 days during period 3 and was addressed in the weekly group meetings.
During period 3, MBD rate dropped further to 17% from 20%, after the implementation of parenteral supplementation of calcium and phosphorus in TPN, though during the sustainability period, the MBD rate again increased to 21%. This could have been due to higher proportion of ELBW neonates in this period. The cumulative calcium and phosphorus intake over the entire period of 8 weeks showed that the intake had increased significantly between period 2 and period 3. This is attributed to adding calcium and phosphorus in TPN from day 1 of life, as well as bridging the gap between parenteral and full volume enteral feeds by early fortification at 100 mL/kg of feeds. The change in the unit protocol to supplement as per AAP recommendations,8 which aimed for higher calcium and phosphorus supplementation, compared with ESPGHAN,6 would also have contributed.
The incidence of MBD among ELBW is always higher. It has been estimated as 55% based on bone mineral content.5 McIntosh et al (1981–1985), in an observational study of ELBW infants, reported 47.5% incidence of radiological rickets,17 while in a more recent retrospective observational study by Viswanathan et al, reported MBD rate of 31% among ELBW infants using QUS.4 Our baseline incidence of MBD among ELBW babies (82%) was higher, probably because we used biochemical parameters for the diagnosis.
Studies have shown that infants treated with methylxanthines and furosemide cause increased urinary calcium excretion, thereby increasing risk of MBD.18 19 In our study, the usage of methylxanthine had increased during period 3 compared with period 2 because we had a greater number of ELBW babies in the intervention 2 group, in whom methylxanthine usage is higher. Usage of diuretics and postnatal steroids was limited. A recent study20 has suggested that physical activity programmes reduce demineralisation in VLBW babies. We did not have a dedicated physical activity programme for promoting bone mineralisation.
Balancing effect
We faced solubility issues with parenteral calcium and phosphorus in TPN twice. Both the times the TPN worksheet was rechecked, and the staff nurse educated on the procedure of adding calcium and phosphorus in TPN. None of the babies had hypercalcaemia.
Strength of the study
To the best of our knowledge, this is the first QI intervention towards reducing MBD rate.
The overall generalisability of this project is high. It is feasible, low cost and has potential for high benefit.
Limitation of the study
The incidence of MBD was based on ALP values and the bone mineral content could not be measured.
We initiated both PDSA 2 and PDSA 3 at the same time; hence, individual effects on the MBD rate could not be ascertained.
The sample size of the study was small especially during PDSA 2 and 3; hence, we could not demonstrate a statistically significant change in the outcome.
Lessons learnt and challenges faced
We faced many challenges during the implementation of the QI project. First and foremost was the change in the policy of fortification of EBM for all VLBW infants, that is, adding HMF to EBM by day 14 of life in PDSA 1. It was very challenging to convince all the consultants as there were serious disagreements and concerns of feed intolerance and risk of NEC. This was even more obvious during PDSA 2 and 3 when HMF was added to EBM very early when the feed volume of 100 mL/kg/day was reached, mostly during the first week of life. We had a meeting with all consultants and stakeholders and reviewed the present literature on multicomponent fortification. The residents and postgraduates were made to present the literature and evidence on multicomponent fortification. Seminars and journal clubs were presented. We also made use of the social media, created a separate WhatsApp group for the same where everyone could put in their queries, and articles with supporting evidence were posted for the same. This helped us to convince everyone in the neonatal team and thus the change in policy was adopted. We faced problems in procuring intravenous phosphorus preparation when the project was implemented. Hence, we had to proceed with enteral supplementation first and take up parenteral supplementation later in PDSA 2 when intravenous phosphorus was available. There was also scarcity of HMF sachets supplied owing to the economic condition of India at that point of time. A lot of logistic issues had to be addressed during the study which we did not anticipate. We did face precipitation issues in TPN a couple of times when calcium and phosphorus were added. We had to review the process of TPN preparation and go through each and every step to find out the problem. We also made the pharmacist and the in-charge nurse to reprepare the TPN to see if it occurs again. All the doctors and staff were educated and same was demonstrated to everyone. If we were to undertake this project again, we would probably start by ensuring a steady supply of intravenous phosphorus and HMF sachets in the pharmacy first. We would also like to review the current literature on the definition, pathophysiology, investigations and management of this MBD in VLBW neonates owing to the chronicity of the disease and the rapidly changing evidence and concepts in the field of neonatology, so that we are updated and we adopt to the state-of-the-art guidelines for the same, making diagnosis and management accurate. We hope that our work leaves a positive impact and motivates others to take up this project to reduce the problem of MBD in preterm neonates.
Conclusion
Simple adoptable policy changes have been effective in reducing MBD. This QI project provided a systematic approach in implementing protocol to reinforce that early parenteral calcium and phosphorus supplementation in TPN and optimising enteral supplementation with multicomponent fortifiers significantly reduce the occurrence of MBD in VLBW babies.
Future direction
Non-pharmacological measures like physical activity programmes may have to be implemented in the NICU. Future studies are needed to study the effect of fortification at a feed volume of 20–40 mL/kg/day feeds and effect of using human milk/mother’s milk-based fortifier on the incidence of MBD.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Institutional Research Ethics Committee, Sri Ramachandra Medical College and Research Institute, Chennai, Tamil Nadu, India (Ref: CSP-MED/15/AUG/24/36). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We hereby acknowledge all the members of our quality improvement team and statistician Mr Michael for their valuable support and contributions to our quality improvement project.
References
Footnotes
Contributors Study planning—KMV, UB, PA and BN. Study conduct—KMV, AC and MSJS. Data collection—KMV. Data analysis—KMV, UB and AC. Manuscript writing—KMV, UB, PA and BN. Guarantor- PA
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. Publication of this article is made Open Access with funding from the Nationwide Quality of Care Network.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.