Article Text

Statistics from Altmetric.com
Background
The NICU expenses to the hospital are classified into fixed (salaries to the personnel, equipment costs, etc) and variable costs (supplies). These costs are a major decisive factor for fixing the patient bill.1 2 Floor cleaning is an essential part of maintaining asepsis in the Neonatal Intensive Care Unit (NICU). Although there are numerous agents, there is limited evidence to guide the choice of floor cleaning agents in the NICU.3 4 The microbicidal activity and the economic impact of these agents are variable. Ovum woman and child specialty hospital is a 15-bedded level-III tertiary care referral centre in Bangalore rural. The NICU is spread over three patient care areas (including isolation and stepdown areas) over 1850 square feet. We used 2% glutaraldehyde (Bacillocid special) once in 6 hours for floor cleaning. The chemical disinfectant consumption for glutaraldehyde alone amounted to an expense ranging between Rs. 23 590 and Rs. 26 960 in May and June 2021 (Rs. 100 per patient per day). There was concern about the increased costs of these agents for a hospital functioning in a rural setup with affordable pricing for the patients. Reducing per capita healthcare costs is an essential component of the triple aim in healthcare launched by the Institute for Healthcare Improvement. We decided to address this problem with a quality improvement (QI) methodology using the Point of care QI model.
Methods of improvement
A multidisciplinary QI team was formed consisting of the housekeeping in charge, infection control nurse of NICU, manager, 2 consultants of NICU and lead neonatologist of the hospital. The study was conducted in the NICU between May 2021 and March 2022. In the first team meeting, the reasons for floor cleaning agents increased costs was analysed using the root cause analysis. The consultants and nurse decided to review the available chemical disinfectants and their microbicidal action. The housekeeping in charge and manager were responsible to look into the dilution and inadvertent wastage of the solution during cleaning. In the second meeting, after a week, it was found that the solution usage was as per the manufacturer. Based on evidence, a detailed discussion of available chemical disinfectants was presented based on evidence.3 Glutaraldehyde-based solution, in comparison to hypochlorite, had the advantage of action even in the presence of organic matter, killing Mycobacteria and spores of Bacillus. The cost of hypochlorite-based solutions was relatively less. As infections posed by Mycobacteria and Bacillus were low in NICU, the team decided to try the hypochlorite-based solution in a few shifts (change idea). One team member raised a concern about increased healthcare-associated infections (HCAI) with the new policy. The team members decided to implement the change cautiously with careful monitoring of HCAI rates (balancing measure).
The NICU had a baseline incidence of HCAI rate of 8 per 1000 patient days in the preceding 2 years (2019 and 2020). We aimed to reduce the floor cleaning costs of the NICU by 50% without a 10% increase in HCAI over 3 months (July 2021 to September 2021). An episode of HCAI was labelled based on the German neonatal nosocomial infection surveillance system.5 The infection control team did the surveillance for HCAI. The data on the consumption of floor cleaning solutions were obtained between the 25th of the previous month to the 24th of the current month (indent cycle of NICU) from the indent data of the hospital management system. A number of shifts glutaraldehyde and hypochlorite were used were the process measures. The monthly costs incurred per patient per day on both the solutions for the NICU were the outcome measure.
In the first Plan-Do-Study-Act cycle (PDSA) (2 July 2021–31 July 2021), the team decided to use 1% hypochlorite for floor cleaning only in the afternoon shift and continue with glutaraldehyde-based solutions for the remaining three shifts. The change in protocol of floor cleaning was informed to the team of housekeeping personnel at the beginning of the month and a reminder was placed as a poster at the NICU noticeboard. In addition, the monitoring for HCAI was continued.
With no significant changes to the rate of HCAI, the team decided to extend the use of hypochlorite solution to three shifts and continue with glutaraldehyde in one shift in the second PDSA (2 August 2021–31 August 2021). The change in the floor cleaning protocol was similarly informed and updated in the notice board as in the first PDSA. The monthly results of cost consumption and HCAI rates were displayed on the hospital notice. We used the run chart rules proposed by Anhøj.6
Results
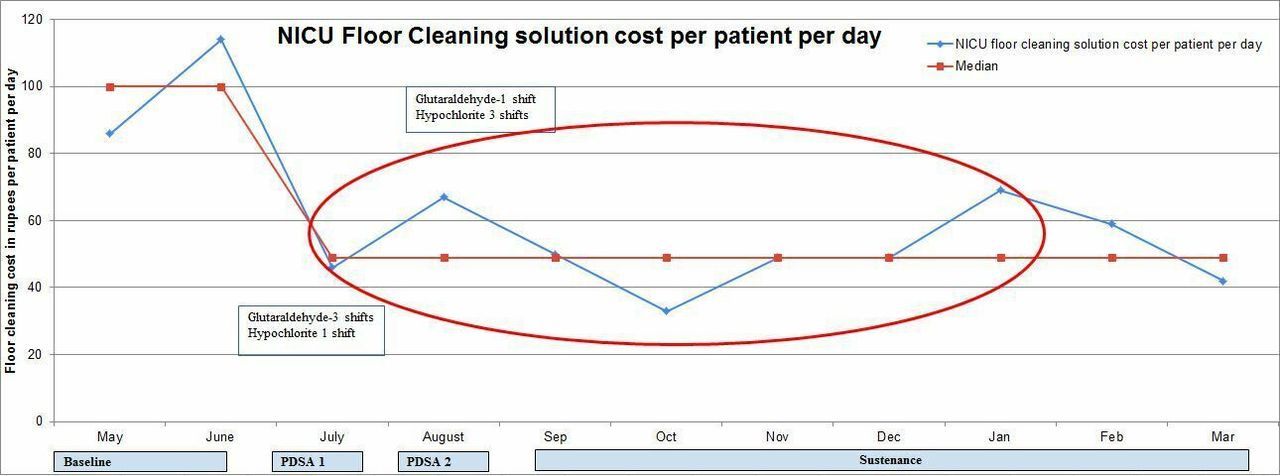
After implementing the new policy stepwise, there was a significant reduction in cost consumption on floor cleaning solutions without any change in the HCAI rate. There was a reduction in NICU cost consumption from a range of Rs. 23 590–Rs. 26 960/- (Rs. 100/patient/day) to a range of Rs. 7941–Rs. 15 355/- (Rs. 49/patient/day) after the change.
We used the run charts to analyse our quantitative data. We used 2 months (May and June 2021) costs per patient per day to calculate the baseline median. We identified a shift from July 2021 to January 2022 (figure 1). The median HCAI rate during the study period was 3.7 per 1000 patient days, less than the expected rate of preceding years (online supplemental figure 1).
Supplemental material
{kind=link}
Run chart showing NICU cost consumption for floor cleaning solution per patient per day. The oval depicts the shift of changes. NICU, Neonatal Intensive Care Unit; PDSA- Plan-Do-Study-Act cycle
Conclusion
We reduced the operational expenditure of housekeeping in NICU by around 13 000 rupees a month without any increase in HCAI. To our knowledge, this is the first report of a hospital using QI methodology to reduce costs on housekeeping. This saved cost is equivalent to a monthly salary of the housekeeping personnel of the hospital. The study analysed an indirect measure of no increase in HCAI to support the change idea instead of a direct measure of microbiological surveillance is a limitation of the study. We believe that other hospitals, especially in the resource-limited setup, could use a similar approach to ease their consumption cost and continue quality care.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge the support and encouragement of Mr. Umesh who engaged their housekeeping staff in the improvement effort. We also acknowledge the support of Mr. Arjun, Operations Executive for supporting the initiative and helping with the data.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @abhiaradhyas, @drpraveen_v
Contributors ASA: conceptualised the study, supervised data collection, data analysis, critical inputs to the manuscript and drafted the initial manuscript. LM: designed data collection tool, data collection, data analysis and approved the final manuscript. VR: assisted in data collection and data analysis, approved the final manuscript. PV: supervised data collection, critical inputs to the manuscript and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. Publication of this article is made Open Access with funding from the Neonatal Care & Research Institute private limited.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.